
Abstract
Background:
The UK will host the Paralympics in 2012 and the Commonwealth Games in 2014 showcasing the talents of elite athletes and aiming to inspire the population to become involved. However, low levels of physical activity are prevalent: only 40% of men and 28% of women meet the minimum UK physical activity recommendations. The population of people with limb absence is no exception.
Objectives:
To determine if people with amputation are participating in physical activity and sport; whether post-amputation activity levels match pre-amputation levels; and if there are motivations and barriers to participation.
Study Design:
Literature review.
Methods:
Five reviewers systematically searched all peer reviewed and gray literature in seven bibliographic databases and the Cochrane Library.
Results:
Following rigorous elimination, 12 articles were finally included in the review and critically appraised. Four themes were identified: components; rehabilitation outcomes; body image; and motivations and barriers to participation.
Conclusion:
People with limb absence are not participating in physical activity conducive to health benefits, and only a minority participate in exercise and sports. Participation following amputation does not mirror that of pre-amputation levels, and more barriers than motivations exist to adopting or maintaining a physically active lifestyle.
Clinical relevance
This literature review aims to inform those involved in rehabilitation and ongoing care of those with limb absence about what motivates or precludes their participation in physical activity, exercise and sport. Such knowledge could be applied to improving health and wellbeing in this population.
Background
The Paralympics will take place in London in the summer of 2012. In addition, the Commonwealth Games are to be hosted in Glasgow in 2014 providing an exciting and unique opportunity to profile physical activity, exercise and sports for the able-bodied and those with a disability. In 2002, the Commonwealth Games introduced Elite Athletes with a Disability (EAD) to the events. This was repeated in 2010 in Delhi and will be the case in Glasgow. All generations will be exposed to the obvious media coverage surrounding these events.
In this Prosthetics and Orthotics International special edition much emphasis is placed on the elite para-athlete performer. However, the purpose of this particular review is to learn from the literature on how to promote physical activity, exercise and sport in non-elite, everyday prosthesis users. Although elite athletes form only a small proportion of the population, countless people with a sedentary lifestyle are encouraged to view them as role-models who will inspire them to become physically active. This is also true for elite athletes with a disability who may inspire their less active peers. The Glasgow Legacy Framework 1 for the forthcoming 2014 Commonwealth Games suggests that Scottish sporting champions can be role models to inspire people to become more physically active. The desired outcome following the Commonwealth Games is to encourage a cultural change in the people of Glasgow and increase their participation in physical activity and sport. 1 Both the Paralympics in 2012 and the Commonwealth Games in 2014 will be platforms for the celebration of sport and personal achievement. Preceding the Glasgow event, the UK government has responsibility for maximizing an increase in participation at community and grassroots level in all sport and across all groups following the Paralympics. 2 A second ambition of both events is to increase the capacity of the sports infrastructure through improved facilities, club formation and development and coaching training and education.1,2 However, a recent review of the impact of major sports events on health found little evidence for uptake of activity in populations around major events. 3 The review concluded that the available evidence is not sufficient to confirm or refute expectations about the health or socioeconomic benefits for the host population of previous major multi-sport events. The forthcoming Paralympic Games and Commonwealth Games, cannot be expected to automatically provide health benefits yet a healthier more active population are certainly desirable legacies after the events. The inclusion of the limb-absent population in these legacies to their benefit should be a priority for those involved in their rehabilitation and care despite this contradictory evidence.1-3
Importantly, the UK population with limb amputation is predominantly elderly and there are low levels of fitness and activity within this group. 4 Despite an increase in opportunities for people with limb absence to participate in competitive sports due to better prosthetic components and the growth and development of sports organizations for the disabled, the numbers of prosthetic sports limb users also remain relatively low. 5 In the authors’ experience, for those more able users, a gentle walking rehabilitation goal such as that undertaken by a large proportion of the UK amputee population, can be limiting. Because of the generally sedentary and elderly amputee patient demographic in the UK, it is more usual for those in a rehabilitation program to achieve a level of physical functioning which may not challenge the person to move beyond a basic walking goal. It is believed that by raising the awareness of practitioners through research and education, participation in physical activity, exercise and sport can be encouraged with resulting sustained health benefits for those with amputation. In an example, the evidence which examines walking interventions shows the benefits of tailored interventions delivered in group-based or individual settings.6,7 There is a suggestion that those with limb absence could and should engage in physical activity to improve their health and social inclusion. 8 This type of upstream intervention is required to reduce the alarming figures on the low levels of physical activity in the UK: only 40% of men and 28% of women meet the minimum recommendations for physical activity in adults. 9 Indeed, in Scotland ‘72% of women and 59% of men are not active enough for health’, making physical inactivity the most prevalent risk factor for coronary heart disease, and more prevalent than obesity and smoking. 10
This review originated from the idea that it might be possible to make a difference to the lives of those with amputation who were motivated to become recreational or elite athletes. Against a backdrop of preparation for the elite international sports events of the next three years and beyond, the authors wish to promote the idea that sport is accessible to those who are athletically inclined. The authors also recognize the importance of the majority being able to maintain basic levels of daily physical activity; adults of age 19 to 64 should aim to be active daily even if they do not wish to participate in sport. Over a week, activity should add up to at least 150 minutes of moderate intensity activity in bouts of 10 minutes or more. 11 The limb absent population is no exception to these guidelines.
In a bid to understand the motivations and barriers in the general population, the authors examined evidence from a general population survey known as the Allied Dunbar National Fitness Survey 12 conducted during the early 1990s. This large descriptive UK survey suggests several motivations for participation in physical activity. These include the physical and emotional concepts suggesting people wish ‘to feel in good shape physically’, ‘to improve or maintain health’, and ‘to feel a sense of improvement’. Similarly, the same study reported barriers to physical activity uptake such as physical (‘I’m too old’), emotional (‘I’m not the sporty type’), and motivational (‘I haven’t got the energy’).
Following on, the authors were keen to understand if similar principles applied to those with limb absence who have low levels of physical fitness due to a combination of a sedentary lifestyle and underlying pathologies. These include disease processes such as peripheral arterial disease and diabetes. In aligning the authors research objectives with those already applied to the able-bodied population, two areas of outcome were soon identified; the first was to encourage those who did not require high performance prostheses to become more active by participating in daily physical activity; and the second to enable those who were already physically fit to realize their potential through the various levels of competition sport from school and community level sports to international level competition. It is recognized that this second outcome may or may not require standard or higher performance prostheses to participate.
This background led to the initiation of this comprehensively structured review of the available literature. The authors were keen to understand the following: are people with amputation participating in physical activity, exercise and sports? Are these people participating at the same level as they did before their amputation? And what are their motivations and barriers to participation? The aim was to gather data, and provide conclusions on what motivates or is a barrier to participation in physical activity, exercise and sport for those with lower limb absence. The authors were also curious about the thematic groups which could emerge from the relevant literature which might describe the behaviours of those currently engaged in physical activity and whether these themes were related in any way to the motivations and barriers to participation.
Methods
During 2011, a literature review was systematically performed by a prosthetic and physical activity for health research team based at the National Centre for Prosthetics and Orthotics, University of Strathclyde in Glasgow, UK. The review covers all peer reviewed and gray literature to date. The bibliographic databases ASSIA, CINAHL, Embase, Medline, Sport Discus, PsycINFO and AMED and the Cochrane Library were searched using a combination of keywords and subject headings (Table 1). References from selected articles were also searched for any key literature not previously identified.
Abbreviated summary of subject headings and keywords.
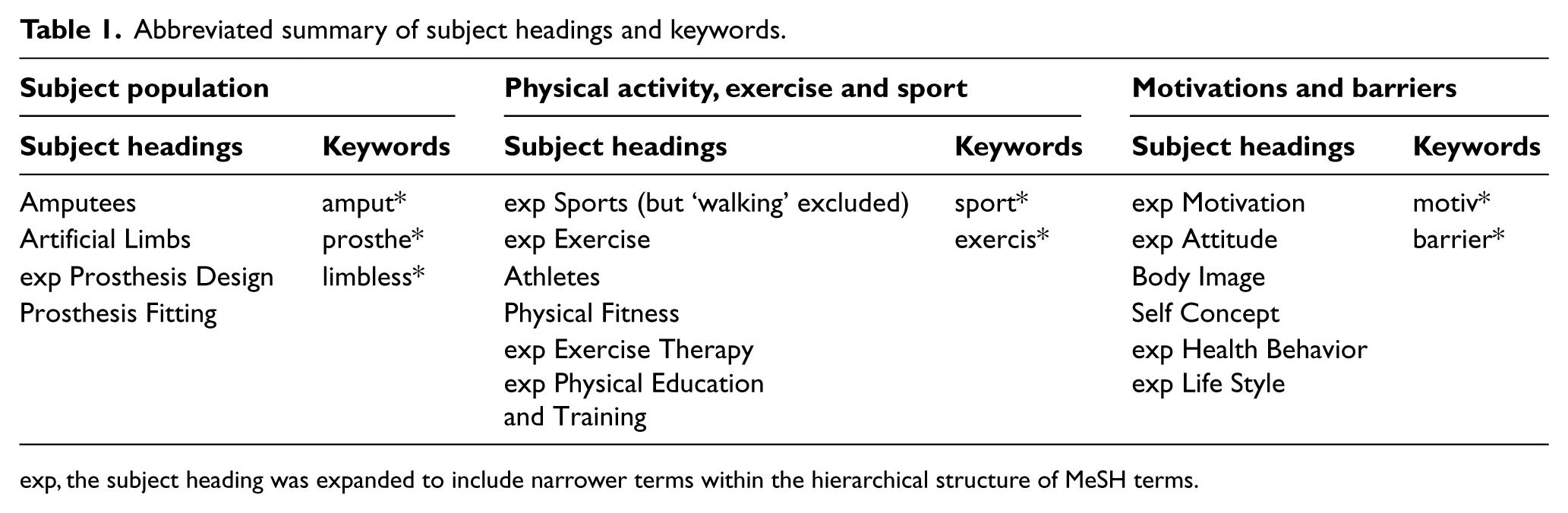
exp, the subject heading was expanded to include narrower terms within the hierarchical structure of MeSH terms.
A summary of the subject headings and keywords used in combination in the Medline search is presented in Table 1. This search strategy formed the basis for the other databases, although each database has unique thesaurus terms.
Studies were considered eligible for inclusion if they met the authors agreed criteria. Sensing that the topic field could be narrow, the authors were keen to minimize the overuse of exclusion criterion in order to broaden the search scope. The obvious inclusion criterion was people having acquired amputation or congenital absence. For sensitivity, the search aimed to identify studies on the limb-absent population. However, to be included in the review, the study participants had to be users of prosthetic devices. For example, studies which researched swimming when the users were not wearing a prosthesis were excluded. 13
Although there was an initial desire to examine the population of only lower limb prosthesis users, studies describing those with upper limb absence were included in order not to exclude key works. Studies testing mixed populations with disabilities were excluded unless amputee-specific data and findings could be extracted. This did exclude otherwise relevant papers14-17 but focuses the review on the experiences of the prosthesis user. No date restrictions were put on the search and studies were included regardless of participant numbers. No language restrictions were placed on the search but studies were only included if they were available in English or via translation.
Results from the completed literature search were downloaded to reference management software and the duplicates removed. During the review process, article abstracts were scanned for relevance by four reviewers. Full text copies of all potentially relevant studies were obtained. These articles were then considered for inclusion by at least two reviewers. Any disagreement between reviewers following consideration of the inclusion and exclusion criteria was resolved by discussion with a third reviewer.
A simple standardized data extraction form was developed to summarize information from the eligible articles. The form was developed from the Narrative Synthesis in Systematic Reviews project 18 and piloted on a selection of the articles. The form enabled reviewers to document the author and year; country of origin; study type; methodology; intervention; participants; context; outcomes; and results. In addition, the process of data extraction led to the identification of themes and the focussed recommendations for the completed review.
Results
In total, 697 articles were identified from the literature and once the duplicate papers had been removed, 684 papers were comprehensively scanned for relevance. The aforementioned inclusion and exclusion criteria were applied, 89 references appeared to meet the criteria, and the full text versions were sourced. Of these, 12 met all of the inclusion criteria and were included in the review.19-30 Using the headings from the data extraction form, Table 2 provides an overview of the 12 included studies.
Summary of 12 included articles.
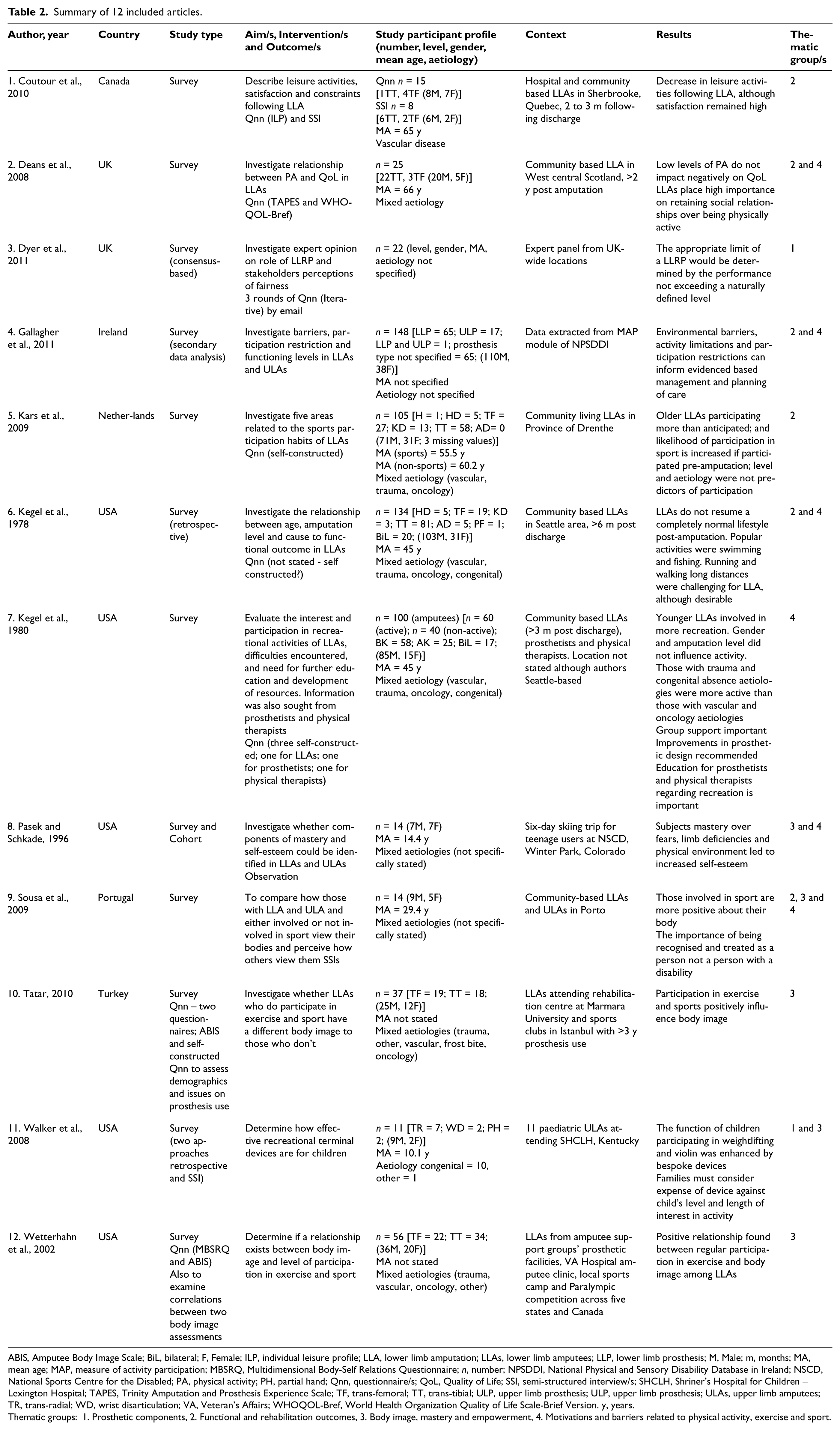
ABIS, Amputee Body Image Scale; BiL, bilateral; F, Female; ILP, individual leisure profile; LLA, lower limb amputation; LLAs, lower limb amputees; LLP, lower limb prosthesis; M, Male; m, months; MA, mean age; MAP, measure of activity participation; MBSRQ, Multidimensional Body-Self Relations Questionnaire; n, number; NPSDDI, National Physical and Sensory Disability Database in Ireland; NSCD, National Sports Centre for the Disabled; PA, physical activity; PH, partial hand; Qnn, questionnaire/s; QoL, Quality of Life; SSI, semi-structured interview/s; SHCLH, Shriner’s Hospital for Children – Lexington Hospital; TAPES, Trinity Amputation and Prosthesis Experience Scale; TF, trans-femoral; TT, trans-tibial; ULP, upper limb prosthesis; ULP, upper limb prosthesis; ULAs, upper limb amputees; TR, trans-radial; WD, wrist disarticulation; VA, Veteran’s Affairs; WHOQOL-Bref, World Health Organization Quality of Life Scale-Brief Version. y, years.
Thematic groups: 1. Prosthetic components, 2. Functional and rehabilitation outcomes, 3. Body image, mastery and empowerment, 4. Motivations and barriers related to physical activity, exercise and sport.
Nine of the articles have been published since 200019,22-24,26-28 with three papers being published in 1978, 20 1980 25 and 1996. 21 All of the articles originate in developed world countries and all studies are survey designs. Ten of the articles feature those with lower limb absence,19-25, 29 with two articles featuring those with upper limb absence.28, 30 Ten articles describe participants with mixed aetiologies (vascular, trauma, oncology and congenital).19-22,25,27 Two articles do not describe the reason for limb absence.23, 24
Upon further scrutiny of the 12 papers, and as the authors expected, clear themes emerged. The authors agreed that four themes represented the article content and acknowledged that individual articles could be included in more than one group. These themes were: prosthetic components; functional and rehabilitation outcomes; body image, mastery and empowerment; and motivations and barriers to physical activity, exercise and sport (Table 2). All of the articles describe the recreational and sporting pursuits of the participants. Since this was a focus of the literature review and a prerequisite for articles to be included, it was felt this descriptor would not feature as a standalone thematic group.
Discussion
Our review of the 12 studies that comprise this literature review focuses on a number of themes. As reported in a Dutch study, the results indicate that people are generally inactive (68% of the amputee population), which is a greater level of inactivity than their non-disabled peers (40% of the general population). 19 There are no other known epidemiological studies which report on the physical activity, exercise and sports involvement of limb absent people and this should be pursued. It is reported that there is a decrease in the level of leisure activity following lower limb amputation, although people’s satisfaction with their changed physical status remains high. 26 This is echoed in a 2008 UK-based study 27 suggesting that people place more importance on maintaining social standing and prioritizing relationships rather than adopting a level of physical functioning which may be entirely unfamiliar. It suggests that healthcare practitioners can help their patients understand the importance of social support and facilitate ways of providing this support. Kars’s study 19 found that the likelihood of participating in physical activity, exercise and sport following amputation increased if they participated prior to amputation. Generally, people who do return to leisure or sports activities opt for less strenuous activities such as swimming and fishing where either a prosthesis is not required or the person is not functionally dependent on it to participate. 20 The authors believe that if pre-amputation motivations to exercise can be captured and recreated in the post-amputation period, the negative effects of a sedentary lifestyle could be reversed. Further investigation on this theory is required.
Physical activity may be influenced by psychological function through an increased perception of mastery. The mastery hypothesis is derived from social-cognitive theory 31 and proposes that improved affect following physical activity is due to an increased sense of mastery or accomplishment. It follows that, with a sense of mastery of their prosthesis, a person with lower limb absence may increase their self-efficacy, thereby increasing prosthetic use and ultimately increasing their physical activity levels. The converse of this may also follow that by encouraging physical activity pre-operatively, and with reinforcement of physical activity post-operatively, self-worth and self-efficacy are increased. This theory is supported by a narrative review on the able-bodied population, which suggests that there is a relationship between physical activity and the emotional function component of quality of life. 32 Lessons can be learned from the field of motivation and barriers to physical activity in the able-bodied population which could serve as a comparison and exemplar to the population with amputation. This work is in early stage but should be progressed.
Five of the 12 included articles discuss the concept of body image related to limb loss.21, 22, 28-30 All of the studies show that those people who are involved in sport have more positive feelings about their bodies, with a positive relationship being reported between regular sport participation and body image. However, in Tatar’s Turkish-based study, 29 it cannot be differentiated whether exercise and sport positively influence body image, as those who have a pre-existing positive body image participated in sport. The use of a case-control study design is a positive feature of this study, a design type which also features in the study by Sousa et al. 28 The authors welcome this case-control type of prosthetic research and the data it yields. This is opposed to those types which rely on purely subjective observational data on what may be construed as an impressionable study group as featured in the Pasek study. 21
Findings based on the general population state that physical limitations and a lack of confidence can be barriers to becoming more active, and older and overweight adults can find participation physically demanding as well as embarrassing.12,33 There is perhaps an underestimation in the field on how strong the link is between amputation, body image and physical activity participation. As discussed previously, the social environment in motivating someone to exercise is important. There is again the suggestion that the rehabilitation environment plays a role in helping people overcome fears and anxieties with regards to participation. In this way, longer term commitment and adherence to regular physical activity may be achievable. The article by Gallagher et al. 23 addresses the environmental barriers which exist for people and recommends greater understanding in order to implement bespoke management at many levels of care. These barriers include services, attitudes, climate, the physical environment and income.
Two of the included studies discuss prosthetic components and their use in leisure time and sports activities.24, 30 Dyer used the Delphi method to investigate the role of running prostheses and stakeholders perceptions of fairness in the context of disability sport. While this article does not focus on motivations and barriers within the limb absent population, it is compelling to compare the findings from this work with the authors’ own clinical experiences of prostheses for sport. It is our belief that there could be poor perceptions within the prosthesis user community that participation in sport is only possible with specialized, high performance prosthetic technology. This perception may be true of participation at a competitive sports level, yet the majority of prostheses correctly prescribed in UK clinics today are functionally advanced enough to satisfy the majority of recreational sports user requirements. The study by Walker et al. 30 recommends that bespoke terminal devices for children with upper limb absence be prescribed upon individual consideration of children’s motivations to participate in recreational activities such as weightlifting and violin playing.
Finally, due to the relevance of a Canadian research study, mention should be made of this unpublished article, 34 appearing only in abstract and poster form which was uncovered during the literature search. The authors appreciate that this is an exceptional case, but as the research topic base is clearly narrow and this particular study mirrors the authors’ area of interest, it is felt discussion of the article is justified. The hypothesis was to examine motivation, access and barriers to sports for adults with amputation and this was done by semi-structured interview of 10 people who had sustained traumatic amputation of either upper and lower limbs and who were established prosthesis users. Questions posed included those on pain, health status, current and previous activities, mentors, domestic support and barriers to participation. Two types of motivation for doing sports were identified; universal benefits which included health benefits, social interaction and stress relief; and unique benefits which included increasing self-esteem and improving body image. The subjects reported three types of barriers to participation: 1) physical issues such as stump pain; 2) psychosocial issues including embarrassment; and 3) societal issues stating work hours and cost for example. It was concluded that for positive inclusion in sport the user should have a personal history of sport involvement, they should have mentors and accessible facilities. Organized sports need to be established, sport should be integrated with work, and future studies should examine the topic of addressing depression. Further, with psychological well-being closely linked with physical activity participation, 35 there is a clear need to investigate this avenue of research.
In terms of possible shortcomings of the review and the studies in question, the 12 included articles were all survey designs representative of the special population in question and allowing generalized observations to be made. The significance of the data from the studies was perhaps too broad in order to be specifically relevant to what motivates or precludes someone from being involved in physical activity. However, the broad ranging concepts which have presented have prompted the authors to question theories which can be investigated more fully in their future research. Data collection methods from Kegel’s studies20, 25 could be repeated to inform us of current trends in user involvement in physical activity, exercise and sports. With regards to the relatively small samples sizes which tend to feature in prosthetic research, efforts to recruit greater limb absent populations to participate in studies will always lead to more robust research findings. Finally, as mentioned in the Methods section, the authors would have included four other relevant and vigorous works were it not for the fact that the study populations had mixed disability conditions.14-17 It is important that data on the limb-absent subjects is extrapolated, defined and reported separately from that of people with different conditions in order that conclusions and recommendations can be clearly gleaned for each special population.
Conclusions
There is a paucity of literature related to the topic area in question. This review has found that people with limb absence are not participating in physical activity conducive to health benefits, and only a minority participate in exercise and sports. Participation following amputation does not mirror that of pre-amputation levels, and more barriers than motivations exist to adopting or maintaining a physically active lifestyle. Studies which explore concepts such as mastery of physical activity, exercise and sports skills, and body image related to self-esteem, can be drawn upon to further the work for the mutual benefit of prosthesis users and healthcare professionals. The authors would like to capitalize on the extensive physical activity for health research focused on the general population and use the findings to investigate similar concepts in the limb absent population who have underlying health issues. Where participation in events such as the Paralympics and Commonwealth Games may be an inspirational reality for a select few, achieving a level of daily physical functioning conducive to health benefits should be a daily reality for all.
Footnotes
Acknowledgements
The authors acknowledge the generous support of the National Centre for Prosthetics and Orthotics at the University of Strathclyde in conducting this literature search and review.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest. The authors alone are responsible for the content and writing of the paper.