
Abstract
Background: Little evidence exists for the orthotic management for individuals diagnosed with diabetic neuropathy and partial foot amputation.
Objective: This pilot study examined differences in balance and pressure distribution while individuals wore foot orthoses inside shoes (BA) and this same orthosis combined with an above-ankle (AABA) orthosis.
Study Design: Within-group repeated measures crossover design.
Methods: Participants with transmetatarsal amputation were assessed during randomized visits with the two interventions. Using a motion analysis system and force plates, we computed the instantaneous inclination angle between the center of mass and center of pressure to quantify balance. The F-Scan in-shoe sensor system was used to measure plantar pressures.
Results: Improvement in balance was measured with the use of the AABA orthosis for the participant who had the greatest time from the timed up and go test (TUG). Plantar pressure during terminal stance did not change between the two conditions. And, lack of ankle mobility appears to lead to less compliance.
Conclusion: Only individuals with reduced mobility may have improved balance with an orthosis that extends above the ankle. The TUG score may be an effective clinical exam to differentiate those individuals who may benefit from an AABA design as compared to a BA design.
Orthotic interventions aim to improve balance and distribute plantar pressures. This study suggests that the different effects on balance while walking with the BA and AABA devices are individually specific and the TUG outcome measure may provide a useful means to determine the appropriate intervention.
Background
Choosing the appropriate orthotic prescription for individuals with diabetic neuropathy and partial foot amputation is a complicated process. Clinical decisions about the impression method, the materials, the design and the alignment of the device are based on each clinical presentation of the individual and practitioner’s rationale. Despite the increased incidence of diabetes and partial foot amputation, the variability of the orthotic management and delicate state of the diabetic foot, research supporting best practice for individuals with partial foot amputation is surprisingly lacking.
A number of co-occurring biomechanical variables have a negative impact on balance for individuals with transmetatarsal amputation (TMA). First, ambulatory function displays less than normal dynamic dorsiflexion range throughout the gait cycle, 1 more inverted positioning at initial contact, irregular rollover and little or no push-off.2,3 Second, the shortened foot and smaller base of support reduces the plantarflexion power generation required for push off, which adversely affects stability.4,5 Finally, balance control of individuals with TMA due to diabetes mellitus and peripheral neuropathy is negatively affected due to the decreased plantar sensation and decreased muscle activation.6-11 Although a few studies have reported improvements in balance and gait variables while using an ankle-foot orthosis (AFO), 12 a recent systematic review concluded that more research is needed to learn about the specific effects of orthoses on gait balance. 13
Orthotic designs for individuals with partial foot amputation may be classified as below-ankle (BA) or a combination of above- and below-ankle (AABA). Previous research lends initial support to the use of partial foot orthoses for improved biomechanical function. Tang evaluated individuals whose TMA was mostly due to trauma and found improved temporal spatial parameters and more normalized sagittal plane ankle angles for individuals using a BA orthosis as compared to no orthosis. 14 In another study, the symmetry of vertical and anterior-posterior ground reaction forces improved with the use of the BA orthosis as compared to no orthosis. Compared to the BA orthosis, the AABA design had improved symmetry. 15 More recently, Dillon demonstrated that the AABA design is necessary to allow the ‘outside of the shoe’ center of pressure to progress beyond the distal end of the residuum, while with the BA design the center of pressure remained proximal to the end of the residuum. 16
Individuals with diabetic neuropathy and a history of ulceration have significantly greater plantar pressures while walking. 17 Following partial foot amputation, these dynamic plantar pressures are greater yet.18,19 Ducic measured decreased peak pressures at the heel and increased peak pressures at the distal end of the residuum in individuals with diabetes as compared to a control group. 6 These peak pressures increase the susceptibility for re-ulceration if left without an appropriate intervention to properly distribute the loads. In clinical orthotic practice, treatment goals include providing a stable base of support and distributing pressures on the plantar surface of the foot.
Previous research with individuals with traumatic (non-diabetic) partial foot amputations found improved function with the AABA design but an individual preference for the BA orthotic design. 15 This discrepancy between functional outcome and the patient’s preference is noteworthy, as it introduces the potential for poor clinical outcome due to noncompliance with treatment regimen. By gathering empirical data to support the use of one design over another, even if under specific criteria, could help facilitate strategies for improving adherence.
The purpose of this pilot study was to provide evidence for selection of orthotic designs in clinical practice. To justify the use of BA versus AABA devices, additional research evaluating their use is needed. Three specific research questions were proposed: 1. What are the different effects on balance during level walking and obstacle crossing between the two orthotic designs? 2. How does peak plantar pressure and plantar pressure distribution differ between the BA and the AABA design? 3. Do individuals with diabetic neuropathy and TMA prefer one design over another?
We hypothesized improved balance and reduced peak plantar pressure when individuals wore the AABA design as compared to the BA design. In addition, we hypothesized that those individuals who feel that the AABA design improved their balance would prefer it, but those who did not sense a benefit would prefer the BA design as compared to the AABA design. Because the functional ability and the potential for further complications vary depending on the disease process and the level of amputation, this study concentrated only on those with diabetic neuropathy and transmetatarsal level of amputation.
Methods
Three independent tests were performed to assess the biomechanical gait parameters, plantar pressure distribution and satisfaction of the two orthotic designs, the:
BA condition with shoes and insoles only;
AABA condition with shoes, insoles and the addition of the BlueRocker AFO.
In this ‘cross-over’ trial, each participant was randomly assigned to one of the two orthotic designs, instructed to wear the orthosis for four weeks before gait analysis and then tested. This was followed by a two-week washout period to eliminate possible carry-over effects and then the participant was assigned to the second orthotic design. Every participant received both interventions.
Participants and procedure
Six individuals with TMA gave written consent for participation and publication and were enrolled into the study after approval by the University of Oregon IRB (Table 1). Participants included individuals with a fully healed TMA due to diabetic neuropathy and an ability to walk without an assistive device. Any person with a history of head trauma and neurological impairment besides peripheral neuropathy were excluded from this study. The six control participants were age and gender matched. While their heights did not significantly differ from the partial foot amputation (PF) subjects, their weights were significantly less (p = 0.016). This discrepancy in weight between individuals diagnosed with diabetes and those without is typical in developed countries. The purpose of the control group was to demonstrate a typical performance of the balance and spatialtemporal parameters.
Participant characteristics.
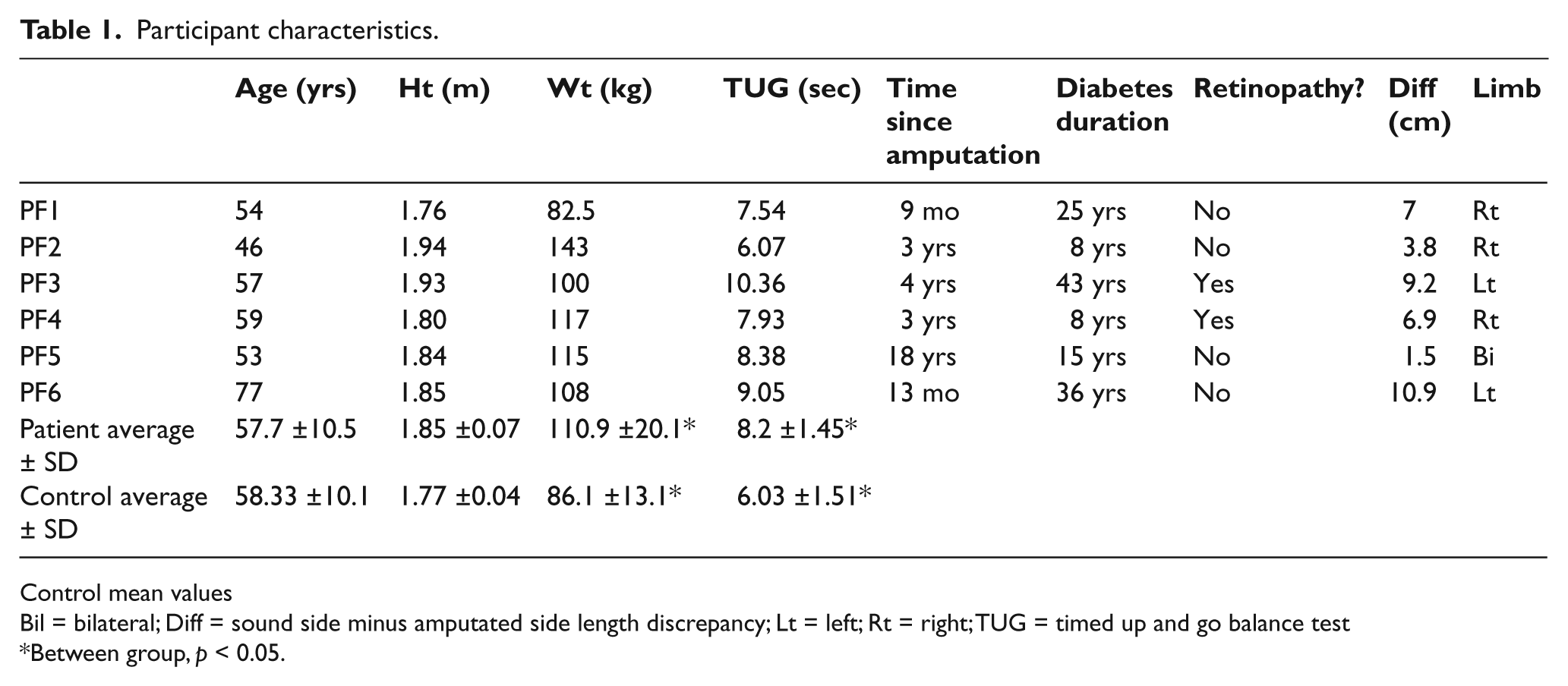
Control mean values
Bil = bilateral; Diff = sound side minus amputated side length discrepancy; Lt = left; Rt = right; TUG = timed up and go balance test
Between group, p < 0.05.
Participants were recruited from the community through contacts with local surgeons, podiatrists and orthotists/prosthetists. Each PF participant was seen by the same orthotist for assessment, casting, measurement and fitting of orthoses and shoes one month prior to each testing session. Participant’s feet were casted positioning the feet in subtalar neutral. If a rigid deformity existed, the foot was positioned as close to subtalor neutral as possible. Total contact insoles were fabricated with Plastizote™ (top layer), poron, a toe filler and a puff base using vacuum over a plaster model. The puff base was modified to accommodate foot rigidity and posting was added to position the tibia vertical in both sagittal and frontal planes during quiet stance. Drew Shoes™ (Drew Shoe Corporation, Lancaster, OH) were modified on the amputated side with a long shank. The insole was placed on top of the AABA orthosis BlueRocker© (Allard USA, Rockaway, NJ) maintaining vertical stance alignment of the tibia (Figure 1).

Blue Rocker Orthosis, rocker soled shoes and total contact foot orthosis (inside shoe).
Motion analysis evaluation included walking at a self-selected pace along a 10-meter walkway on level ground during two randomized conditions: without obstructions, and stepping over an obstacle of 2.5 or 10% of body height to simulate walking over a door threshold or curb. 20 The obstacle was a 1”-diameter PVC pipe positioned in the center of the walkway, between the two force plates. Participants were allowed to rest between trials.
With the hope of using this as a pre-prescriptive analysis, each participant was assessed using the timed up and go (TUG) test 21 while barefoot. Three-months after the collections, the participants were contacted to determine their preference between the two devices using the telephone version of the Prosthetic Profile of Amputee Questionnaire. 22
Measuring technique
An eight-camera motion analysis system (Motion Analysis Corp, Santa Rosa, CA) measured whole body motion. Marker trajectory data were identified using EvaRT 4.4 (Motion Analysis Corp, Santa Rosa, Ca, USA) and smoothed using a low-pass Butterworth filter (cutoff frequency = 8 Hz). A total of 29 reflective markers were placed on subjects’ bony landmarks to define a 13-segment model. 20 The center of mass (COM) position of each body segment was identified for the computation of the whole body COM. 23 The partial foot and shoe as well as the shoe and foot on the sound side were assumed as one segment by summing masses of the shoe and foot together. To determine if the AABA orthosis had an effect on the forward progression of the tibia as compared to the BA device, motion between the shank and the shoe were calculated as the ‘dorsiflexion angle’.
Ground reaction data were collected with two dual AMTI force plates (AMTI, Newton, MA) to calculate instantaneous center of pressure (COP) data at 960 Hz and time-synchronized to the kinematic data. Instantaneous COM-COP inclination angles, defined as the angle formed between a vertical line passing through the COP and the line connecting the COM to the COP, 24 were computed for every instant during the gait cycle. Adults with balance impairment demonstrated larger maximum medial COM-COP inclination angle during walking. 24 Gait velocity was calculated using the distance traversed by the whole body COM in a gait cycle, step width as the distance between the two ankle joint centers at the heel strike, and step length as the distance between heel markers during the double support period.
Plantar pressure was measured separately from gait analysis and collected using bipedal in-shoe F-Scan sensor system (Tekscan, South Boston, MA) at a sampling rate of 50 Hz with thin (0.15 mm), high-resolution (4 sensels/cm2) disposable sensors. The diabetic patients were tested with two conditions:
wearing rocker-soled shoes;
wearing the AA orthosis with shoes.
The sensors were taped on top of flat 1/8” insoles, because the sensors do not conform well to the total contact custom insoles. This data were collected on the same day to increase reliability.
Patient satisfaction was assessed with the telephone version of the Prosthetic Profile of Amputee Questionnaire. 22 Three additional questions were included: Do you feel more or less balanced while using the below-ankle orthosis? Do you feel more or less balanced while using the above-ankle orthosis? And, which do you feel improves your comfort while walking?
Data analysis
The independent samples Mann-Whitney U test was used to examine the between-group (participants with PF and controls) differences in demographic data. Two-way ANOVAs with repeated measure were used to examine the group (control vs. PF and BA vs. AABA) and obstacle height effects on gait temporalspatial or balance control measures. For the plantar pressure distribution, the mean values of the plantar pressure data were analyzed using the related samples Wilcoxin Signed Rank test. The significant level was set at α = 0.05 for all tests. Qualitative results from the patient satisfaction questionnaire are included for discussion purposes.
Results
Participants
The six participants with transmetatarsal amputation in this study varied in age, height and weight characteristics (Table 1). They were male between the ages of 46–77 years (57.7 ± 10.5 years) with varying durations of diabetes (8-43 years) and time since amputation (9 months–18 years). One individual (PF5) had bilateral amputations.
Measures
All PF participants had significantly longer TUG times compared to controls (p = 0.025). The duration of time that the PF group was diagnosed with diabetes had a positive correlation with TUG time (r = 0.82). PF3 whose, diabetes duration was the greatest (Type I), had the greatest TUG time (10.36 sec).
There were significant obstacle height effects on the gait velocity (Figure 2) and stride length in both control and PF participants (p < 0.001 and p = 0.001 respectively). No significant obstacle height effects were detected for medial COM-COP angle or step width. No significant differences in gait temporalspatial or balance measures were detected between the PF and control groups or between the AABA and BA orthoses (Table 2). Only participant PF3 had considerable improvement with the AABA as compared to the BA condition; the medial COM-COP inclination angle reduced by approximately 22% during obstacle crossing (Figure 3).
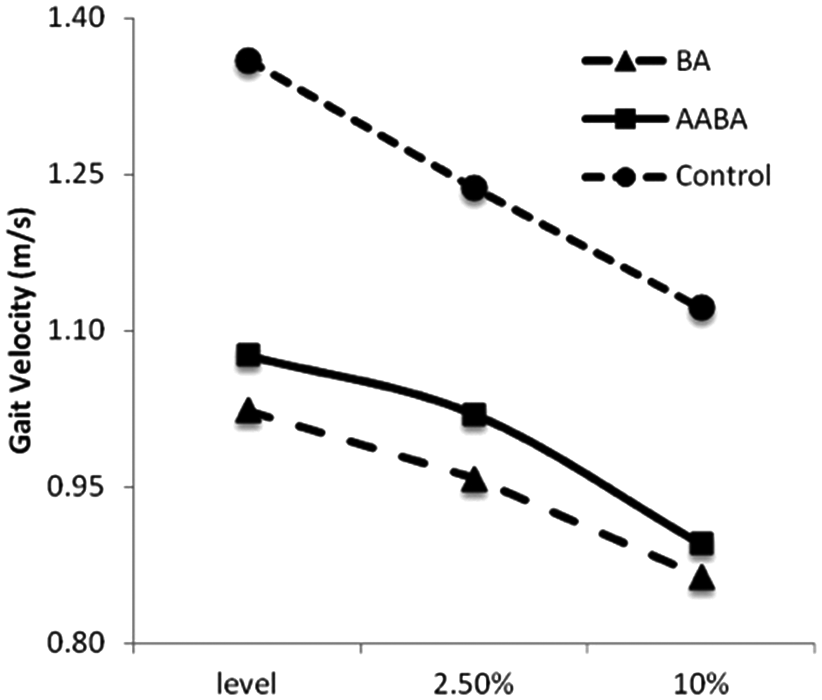
Gait velocities during level walking, 2.5% and 10% body height obstacle crossing trials for control, BA and AABA.
Gait temporal distance parameters during level walking, 2.5% and 10% body height obstacle crossing trials for control, BA and AABA.
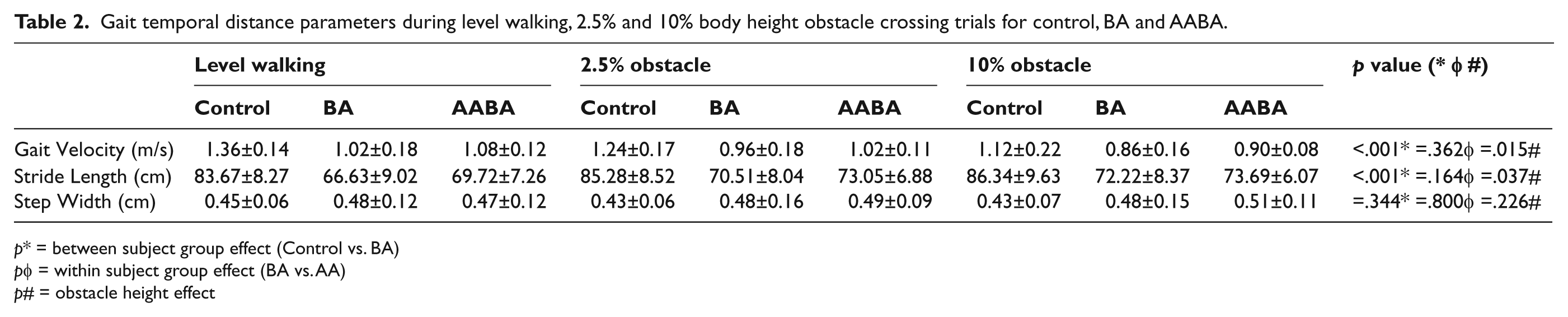
p* = between subject group effect (Control vs. BA)
pφ = within subject group effect (BA vs. AA)
p# = obstacle height effect
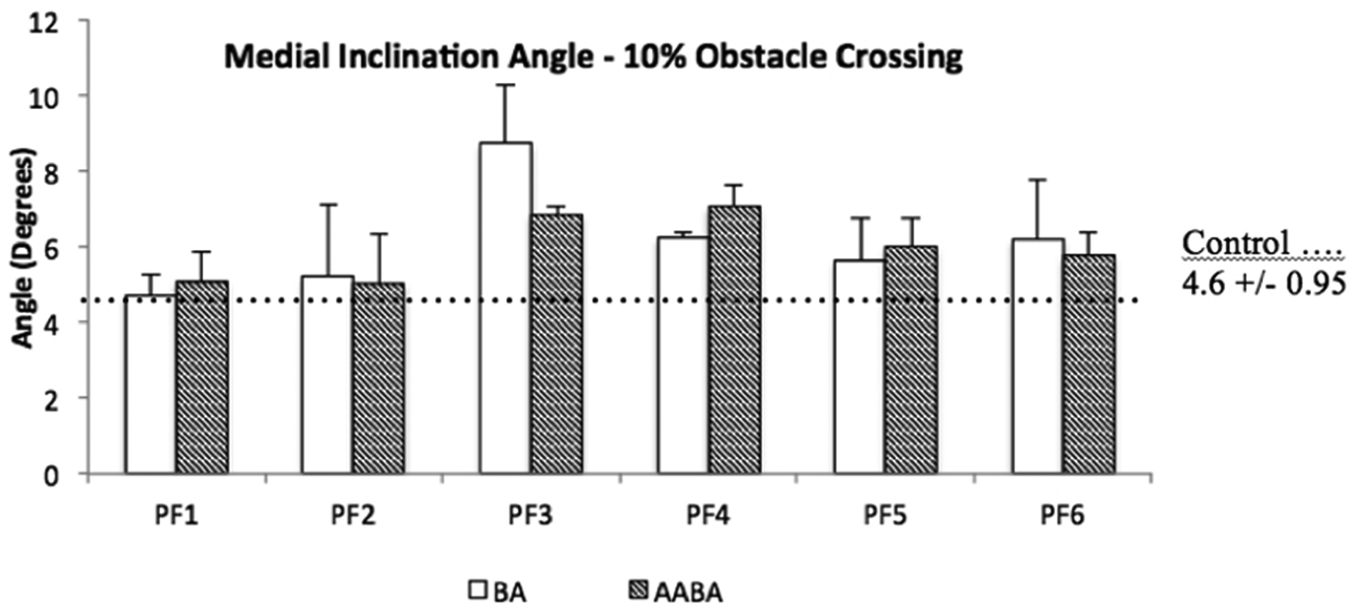
Peak COM-COP medial inclination angles measured when stepping over an obstacle of 10% body height.
In the sagittal plane, the AABA device reduced the motion between the participant’s shank and shoe (‘dorsiflexion angle’) approximately 10 degrees, with about 4.5 fewer degrees of plantar flexion at foot strike and 5.2 fewer degrees of dorsiflexion at terminal stance.
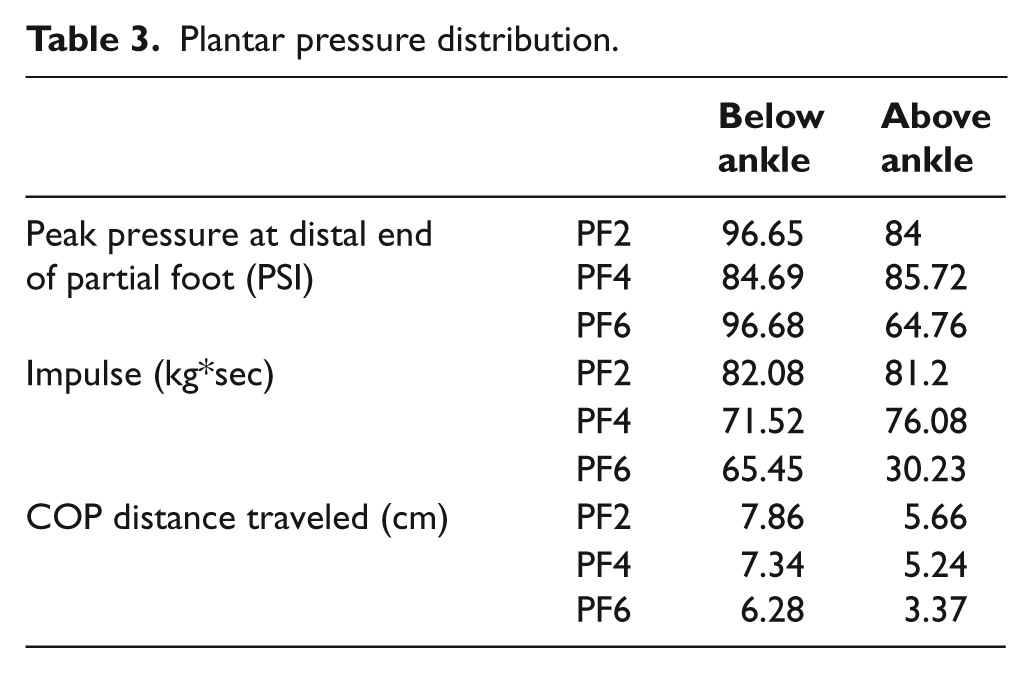
Plantar pressure data from only three participants were analyzed due to loss of data and worsening one patient’s medical condition. The peak plantar pressure, impulse and the COP distance traveled were not significantly different between the BA and AABA conditions (Table 3, Figure 4).
Plantar pressure distribution.
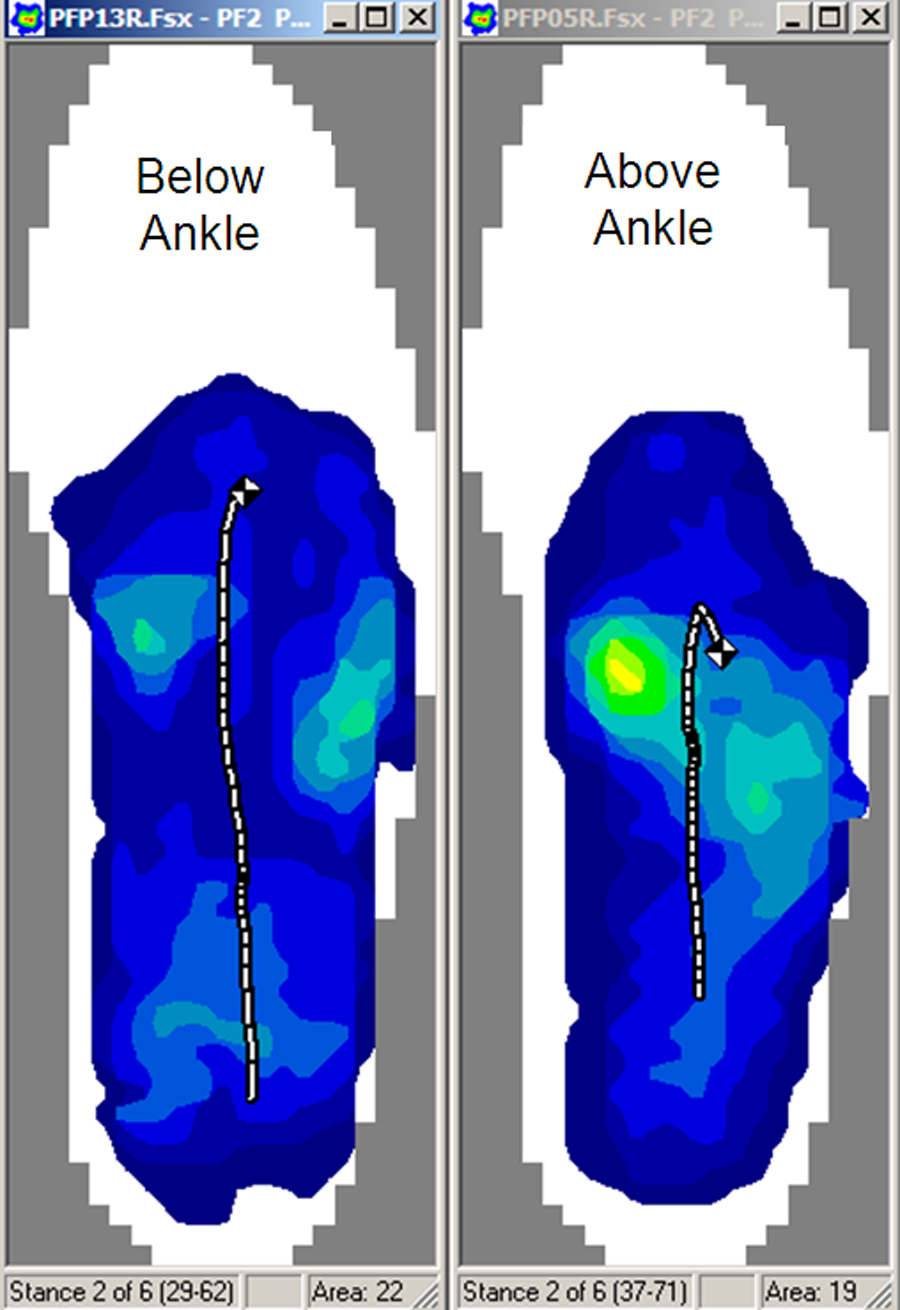
Representative COP trajectories of BA and AABA during level walking trials.
All individuals felt at least moderately satisfied with the comfort, appearance, weight and the way they walked with the BA orthosis; and most became well adapted to using the BA orthosis. Conversely with the AABA orthosis, one participant expressed dissatisfaction with the appearance and his gait; and three of the six subjects chose not to wear the AABA orthosis during the acclimation period. All subjects felt improved balance with the use of the BA orthosis as compared to nothing; while one individual, who had the longest TUG score, felt more balanced with the use of the AABA as compared to the BA orthosis while standing and walking.
Discussion
This pilot study examined balance, plantar pressure distribution and patient preference between below-ankle and above-ankle partial foot orthoses while walking on level ground and over obstacles to provide evidence for selection of orthotic designs in clinical practice. We found that gait balance control did not differ between the BA and the AABA groups. The small sample size is a limitation of the study; however our results of balance suggested that the changes between the BA and AABA groups are individually specific. One participant (PF3) demonstrated a ‘noticeable balance improvement’ with the AABA orthoses. This participant also had the greatest TUG time implying that those individuals with greater TUG time may have decreased functional mobility, thus suggesting a greater need for external support. The TUG score may be an effective clinical exam to differentiate those individuals who may benefit from an AABA design as compared to a BA design.
Both the control and the PF participants had reduced gait velocities as the obstacle height increased (Table 2). Obstacles pose a common reason for falling and require anticipatory postural adjustment. 25 The AABA device may provide postural support during this motor planning period through stabilization of the tibia as the body is moving towards single limb support. Further exploration about the relationship between the effect of an orthoses, which provides slight resistance to forward inclination of the tibia and proprioceptive feedback, during obstacle crossing may influence the design and selection of the intervention for individuals at risk of falls.
Plantar pressures did not change significantly between the BA and AABA conditions. However, in observing the data, the peak plantar pressure remained at the hindfoot while using the AABA device throughout stance and the distance that the COP traveled reduced by about 50%. This suggests that by limiting the forward progression of the tibia, the ‘within shoe pressures’ do not progress beyond to the distal end of the residuum. Conversely, Dillon used force plates under the shoes to measure COP excursion and found that the COP actually traveled beyond the distal end of the residuum with the use of the AABA devices. 16 Our decreases in the excursion of the COP differ from Dillon’s measures due to the methods used. Both measures are important to consider as in-shoe motion describes the direct contact between the plantar aspect of the foot and the shoe while the force plate measures are related to the kinematics and kinetics of the lower limbs.
Patient satisfaction may be one of the most critical and practical parameters to examine. Reasons that prevented the participants from using the orthoses included limitations in ankle ROM, difficulty in donning, the device being cumbersome, and greater comfort without the use of anything on their foot. These are common complaints of individuals who are asked to wear an orthosis.27 Incidentally, only the two participants (PF3 and PF5) who sensed a benefit with the use of the AABA design preferred to it over the BA design.
Conclusion
Clinical decisions about the selection of an above- or below-ankle orthosis for individuals with neuropathic partial foot amputations are based on factors such as the individual’s physical condition, activity level, compliance and motivation. These factors influence the design of the device. This study examined balance, plantar pressure distribution and patient preference for the selection of an AABA or BA partial foot orthosis.
We found that the different effects on balance while walking with the BA and AABA devices are individually specific. The AABA device may provide improved balance in stance as compared to the BA device, but only for those individuals who have imbalance during locomotion. Therefore, the clinical use of an outcome measure, such as the TUG, may provide a useful means to determine the appropriate intervention. Further studies are needed to identify clinical outcome measures that may be useful for selecting the appropriate intervention.
The participants in this study stated that they would prefer to walk with ankle mobility. Although the effect of ankle mobility on balance is unclear at this time, a low profile design that allows some ankle mobility while providing strength and durability to distribute pressure during terminal stance may encourage compliance. Ultimately, the most appropriate intervention is one in which the patient is committed. Even a well-designed orthosis is a failure if not used with fidelity
Footnotes
Acknowledgements
Taka Tarumi assisted with the motion analysis data collections. His time is greatly appreciated.
We are thankful for the funding support Northwest Health Foundation [grant number 10940]; which paid the participants for their time during the study. We are also grateful for the AFOs donated by Allard USA, Inc. and well as a discount on the extra depth shoes from Drew Shoe Corp.