
Abstract
Background: Back pain and ambulation deterioration among ambulatory individuals with cerebral palsy (CP) are common as they grow older and walking aids are often prescribed to improve stability and promote maximal weight-bear on lower limbs during gait.
Objective: To investigate the effects of walking aids on back muscle activity and whole body kinematics among adolescents with spastic diplegia.
Study Design: A repeated-measures design was adopted with participants tested under different walking conditions.
Methods: Ten participants were recruited and Lofstrand forearm crutches were selected. Both the activity of lumbar erector spinae and the kinematics of head, trunk, pelvis and lower limbs during walking were monitored using telemetric electromyography and motion analysis system respectively.
Results: Comparisons between walking unaided and walking with unilateral and bilateral crutch(es) were made. Significant decreases in speed, cadence, erector spinae activity and lower trunk extension were observed during crutch walking together with significantly increased stride time and anterior pelvic tilt.
Conclusions: These findings suggested that Lofstrand crutch(es) reduced muscular demands and lumbar lordosis with increased lower back mobility. The results shed light on the prescription of walking aid in the management and prevention of chronic back pain for ambulatory individuals with CP from a life span perspective.
This study revealed that four-point reciprocal crutch walking can be prescribed to reduce muscle activity, and hence decrease stress at back, during gait among ambulatory individuals with CP that may serve as an adjunct to back pain management in this population group.
Background
Cerebral palsy (CP) is a disorder of the central nervous system in early childhood resulting in motor impairments. 1 Although it is due to a non-progressive encephalopathy, its secondary complications change over time. CP is a lifelong condition but, unfortunately, it has largely been perceived as a ‘childhood disability’ receiving primarily ‘paediatric rehabilitation’. 2 With improved survival in CP in the last 20 years,3,4 the disorder has become one of the largest physical impairment groups among adolescents and adults. 2
Lifespan approach has been advocated in addressing progressively deteriorating functions among people with CP.5,6 In this approach, a comprehensive plan aimed at improving their quality of life is established through maximizing their participation across the lifespan. 7 By analysing problems reported in adulthood, predisposing factors that negatively impact life in later years can be identified. Therapists can then develop proactive strategies at an earlier age. 5 Chronic pain has been reported in children and adolescents with CP8-10 as well as in adults with the condition,6,11-13 suggesting a high prevalence of pain with increased age. Jahnsen et al. 14 reported that nearly one third of adults with CP had chronic pain. It affects both adults with mild and severe motor impairments. 15 Back, hips and lower extremities are consistent sources of pain among people with CP and back pain is the most frequently reported.12,14,16,17
The aetiology of chronic pain in CP remains unclear. Some researchers attributed it to musculoskeletal factors such as abnormal joint stress and muscle over-activity as a result of the movement disorders that characterize CP.18,19 However, pain issue in CP is more complex than musculoskeletal concerns alone. Environmental factors (e.g. walking aid) play a crucial role. Jensen et al. 20 reported a tendency, though not statistically significant, of reduced back and lower limb pain with age, when many adults with CP started to use walking or mobility aids. This suggests prescribing such aids may improve not only ambulatory function, but also pain. However, further study on the role of walking aids in relation to back pain among people with CP is scarce.
Independent walking will be lost in many ambulatory individuals with CP when reaching adulthood.5,14,16 Engel et al. 8 commented that mobility was the greatest functional consequence of pain among adolescents with CP. In a survey of young people with the disorder, Krakovsky et al. 21 concluded that ‘walking’ was one of the four significant functional losses as a result of pain. In a seven-year survey on walking deterioration among adults with CP, Opheim et al. 17 reported that the prevalence increased from 39% to 52% and was most common among respondents with bilateral involvement. A significantly higher pain score was reported among those with deteriorated walking capacity. A complex dynamic exists between ambulation deterioration and pain throughout the lifespan of ambulatory individuals with CP. Although walking aids are often prescribed with deteriorated walking capacity, little is known about their effects on gait, spinal mobility and back muscle activity of the users.
Methods
Effects of walking aids on back muscle activity and whole body kinematics were investigated. Adolescents with spastic diplegia were recruited from special schools for the physically handicapped with the following inclusion criteria: (1) ambulant walker capable of walking unaided for at least 10 m; (2) no back or lower limb pain in the past three months; (3) no surgical intervention in the past six months; and (4) able to follow experimental instructions. Hip flexion contracture was assessed by the Thomas test. 22 Ethical approval was obtained from the University Ethical Committee and informed consent was signed by parents.
The three-dimensional locations and orientation of body segments were monitored by a motion analysis system (Vicon 370, Oxford Metric, UK) with six infrared cameras. The movement of head, upper and lower trunks, pelvic and lower limbs was tracked by 24 reflective markers of diameter 25 mm (Figure 1). For the lower trunk, a rigid cluster with three markers was strapped securely by an elastic belt at the L1 level (Figure 1).23,24 All kinematic data were captured at 60 Hz and the angular movements between body segments were determined using the Cardan Method. 25 Surface telemetric electromyography (EMG) (Telemyo 2400R, Naroxon Inc., USA) was employed to monitor the activity of bilateral erector spinae. The EMG signals were low-pass filtered with cut-off at 400 Hz and sampled at 1500 Hz. 26 A pair of silver/silver chloride surface electrodes was attached to the muscle bulk tip of left and right erector spinae at the L3 level with a ground reference electrode27-29 (Figure 1). Skin abrasion and alcohol cleansing were performed prior to electrode attachment. To allow interparticipant comparison, the EMG data of individual participants were normalized by their own maximum voluntary contraction (MVC). The MVC test was administered with the participant lying prone with hands at their buttock and arched back against the investigator’s resistance at the T1 level. No movement was allowed during the MVC test and the EMG signals were recorded for five seconds. The MVC test was repeated three times for each participant and the maximum value among the three trials was used for subsequent normalization of the EMG signals.
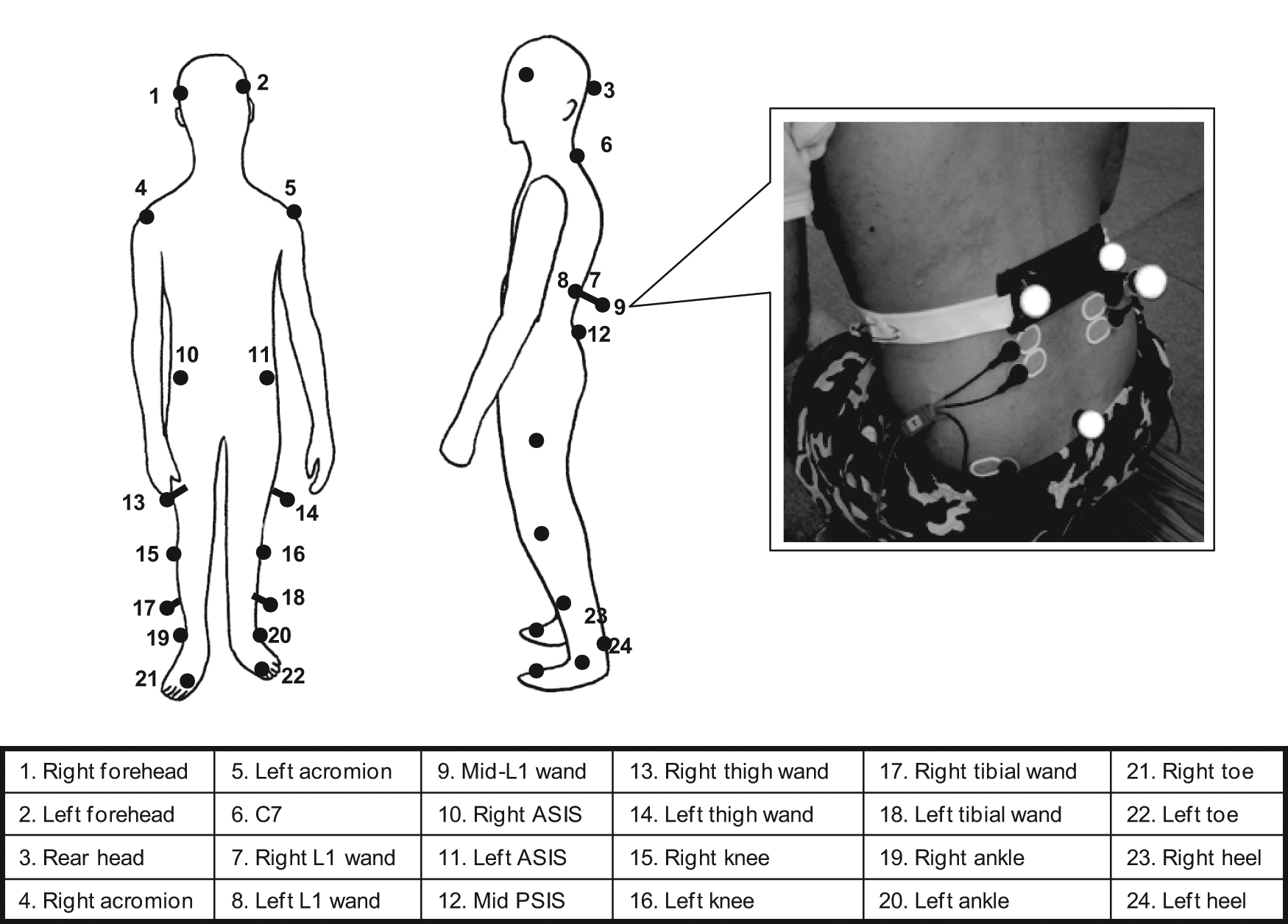
Front and side views of the 24-marker configuration and the rigid cluster at the L1 level and surface electrode placement for bilateral erector spinae.
Light weight aluminium Lofstrand forearm crutch (0.8 kg) was used. The crutch measurement was standardized as the distance from ulnar styloid with elbow at 15° flexion to 15 cm away from lateral malleolus with the participant lying supine. All participants wore shorts and a short-sleeved T-shirt during the experiment. They were instructed to walk at a self-determined speed along a 10-m walkway barefoot. Four-point reciprocal gait (right hand left foot and vice versa) was adopted during crutch walking with training prior to data acquisition. Each participant performed the following three walking conditions in a randomized order: (1) walking with one crutch on the dominant hand (the hand used to write or eat); (2) walking with two crutches on both hands; and (3) walking unaided. Each participant completed five trials for each walking condition with adequate rest between each. All 15 trials were completed within a single experimental session.
For the kinematic measurements, temporal-distance parameters including walking speed, cadence, stride time, and stride length were determined. Range, maximum and minimum values of head, upper trunk, lower trunk, and pelvic motion as well as bilateral hip, knee, and ankle motions of each gait cycle were determined. For the EMG measurements, peak and mean normalized EMG data over one gait cycle were obtained. The first complete gait cycle was extracted from each walking trial and data obtained from the five extracted cycles were averaged for each walking condition for data analysis. One-way repeated measures analysis of variance (ANOVA) was employed to compare the average data of the three walking conditions (i.e. walking condition factor) followed by Helmert contrast analysis for comparing the means between individual levels. For variables with bilateral data (e.g. EMG data, stride length), two-way repeated measures ANOVA was employed with dominant-nondominant-side as the second factor (i.e. the side factor). The level of significance for ANOVA was set at 0.05. For the contrast analysis, Bonferroni correction was applied and the level of significance for multiple comparisons was set at 0.025.
Results
Ten participants with spastic diplegia (five males and five females, mean age: 12.1, range: 8–15 years old) were recruited. Demographic data of the participants are shown in Table 1. Four participants were relying on a pair of Lofstrand crutches for daily walking but they were capable of walking 10 m independently without crutches. The remaining six participants had no previous experience in crutch walking. Symmetrical hip flexion contracture was found in three participants with an average of 5.5°. Four participants were left-hand dominant.
Demographic data of the participants with spastic diplegia.
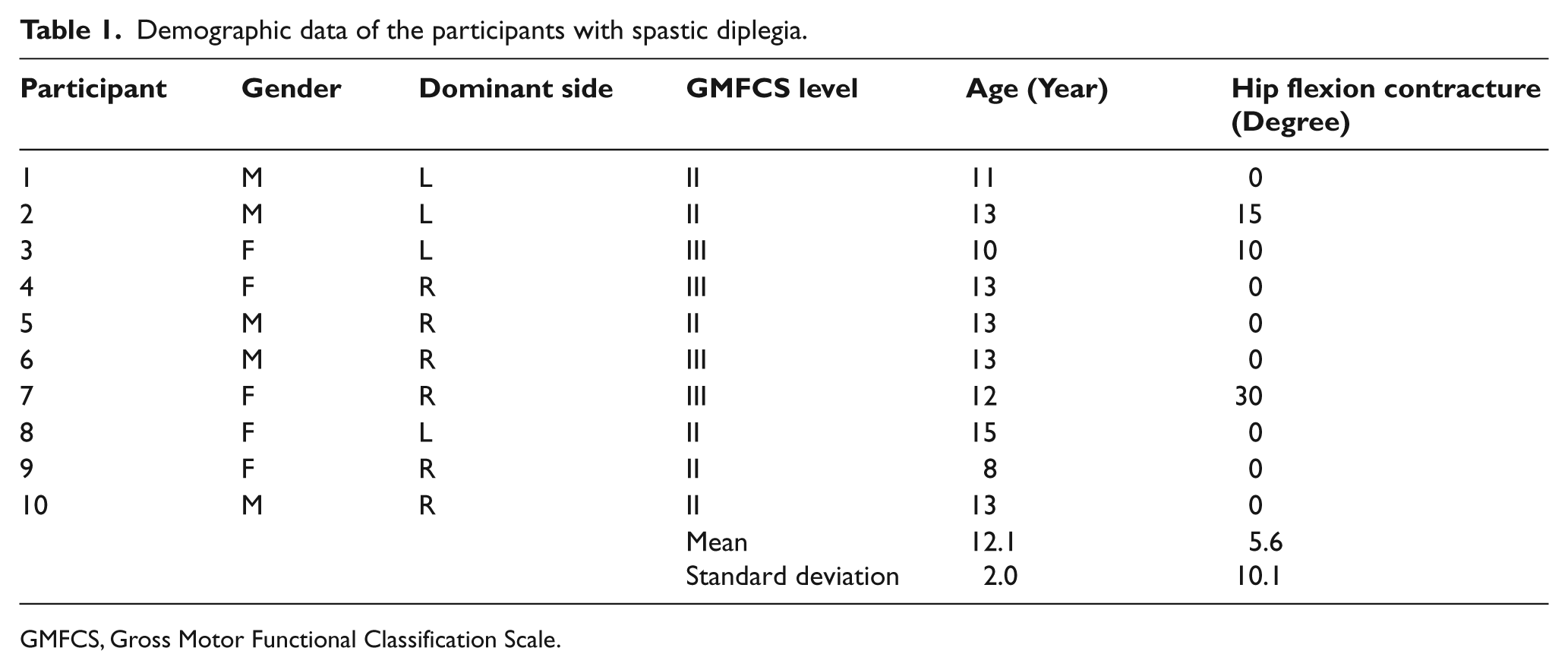
GMFCS, Gross Motor Functional Classification Scale.
A pattern of decreasing walking speed and cadence with increasing stride time was observed from walking without crutch (i.e. no crutch) to walking with unilateral crutch (i.e. one crutch) and to walking with bilateral crutches (i.e. two crutches) (Figure 2). Significant differences were found in walking speed, cadence and stride time. In subsequent contrast analysis (Helmert) (Table 2), significant differences were shown in all three gait parameters at the first level of contrast (no crutch vs. one- and two-crutch conditions).
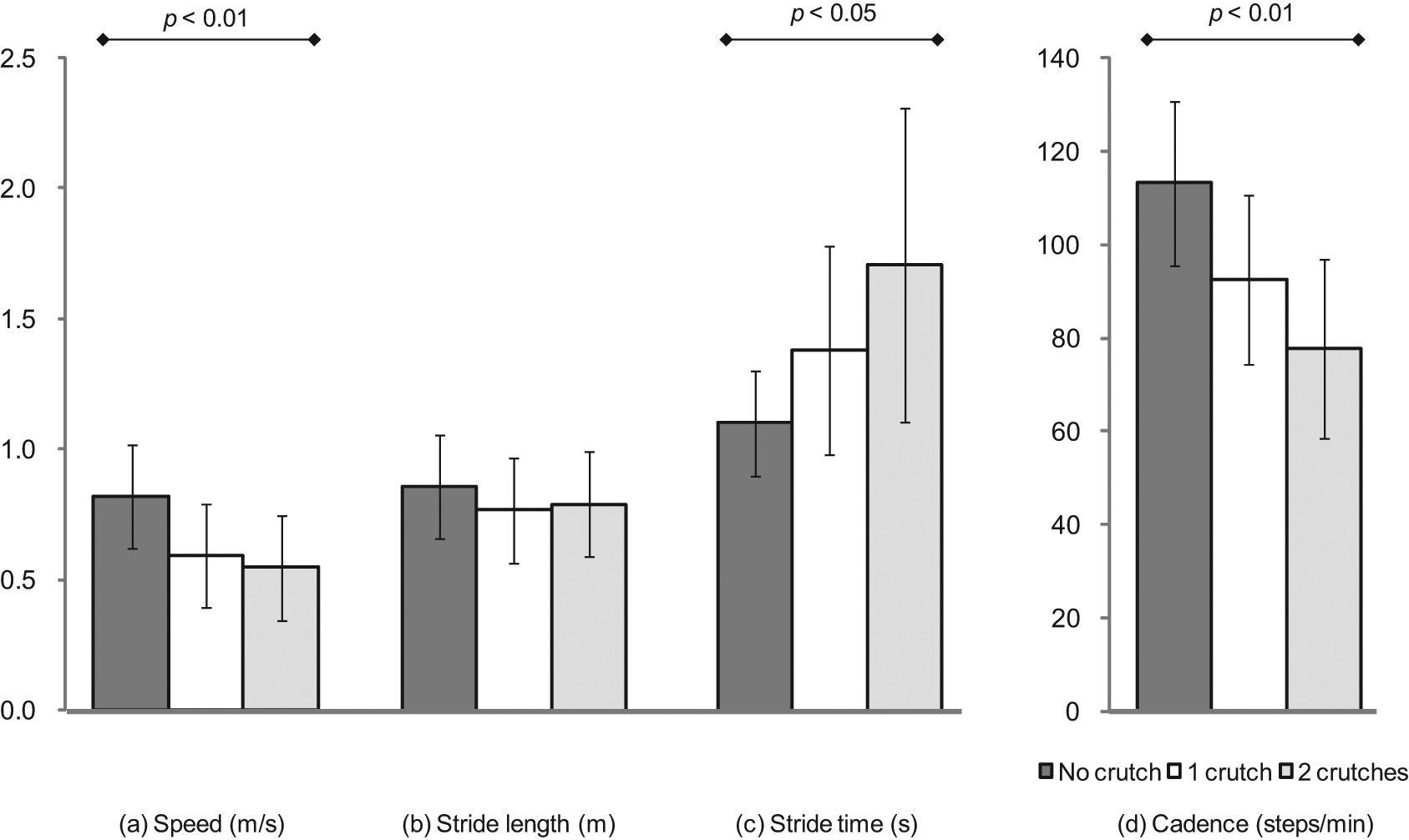
Pooled results of (a) walking speed, (b) stride length, (c) stride time and (d) cadence from the 10 participants during walking without crutch, walking with unilateral crutch on dominant side and walking with bilateral crutches.
Results of the first and second levels of Helmert contrast analysis for walking speed, cadence, stride time, and mean electromyography (EMG) of the erector spinae.
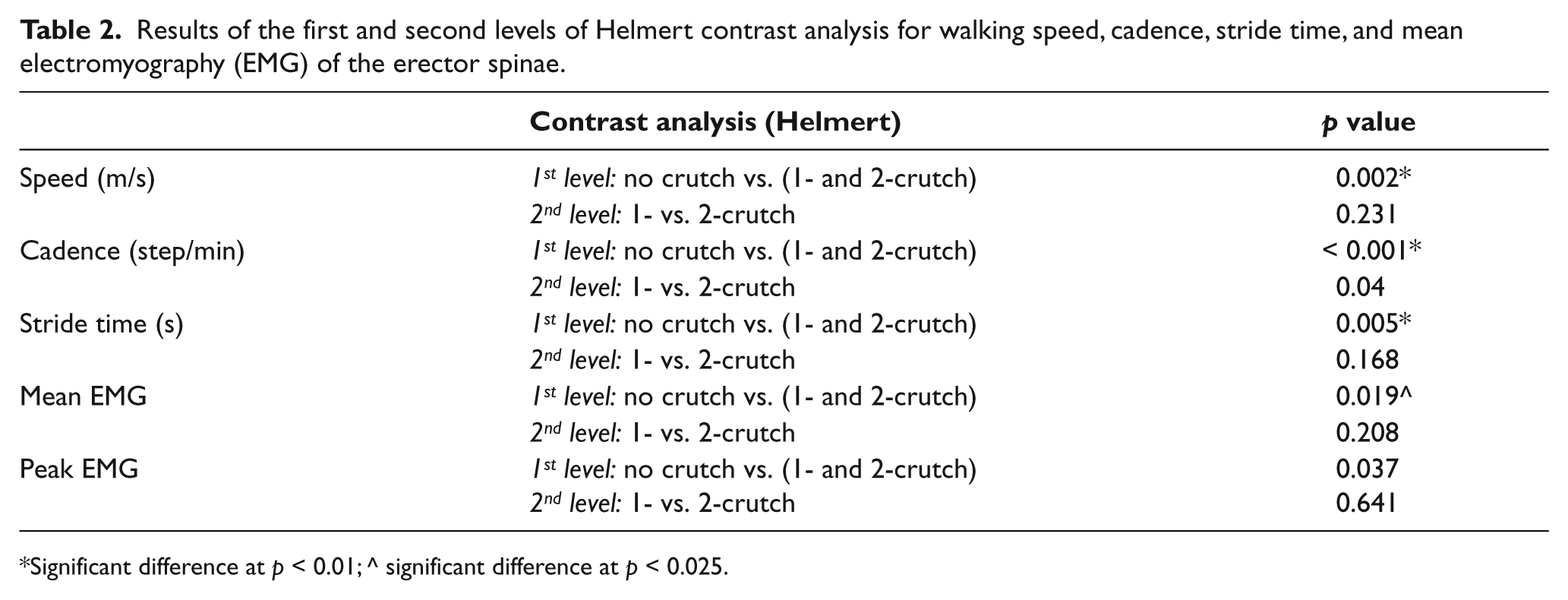
Significant difference at p < 0.01; ^ significant difference at p < 0.025.
For kinematic variables with bilateral data, no significant interaction was observed between the walking condition and side factors. Significant differences were found in the maximum and minimum extension of lower trunk, as well as the range of motion of anterior pelvic tilt and its maximum and minimum values (Figure 3). Apart from the sagittal plane, no significant effect of the walking condition factor was observed in other planes of pelvic motion. Contrast analysis revealed a significant increase in the amplitude of sagittal pelvic motion during crutch walking. In addition, the pelvis was more anteriorly tilted as reflected in both the maximum and minimum pelvic motion in the sagittal plane (Table 3). On the other hand, the lower trunk was found to be less extended with respect to the pelvis as shown from the change in the maximum and minimum lower trunk extension when the crutch(es) were used. All other lower trunk kinematic variables showed no significant difference among the three walking conditions. Significant effects of the walking conditions were also observed with more extended knees during stance in crutch walking.
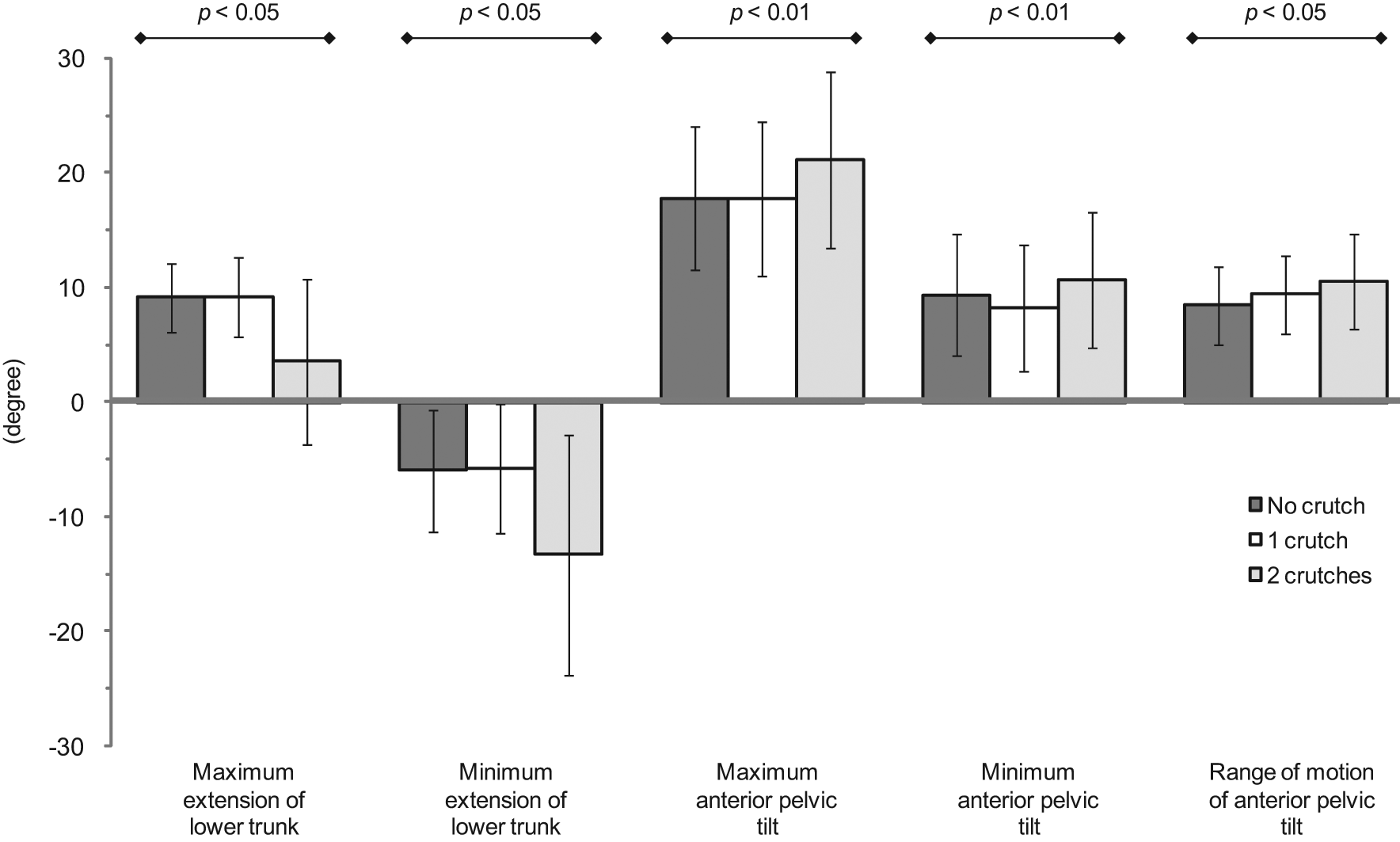
Pooled results of kinematic variables of lower trunk and pelvis with significant difference among the three walking conditions.
Results of the first and second levels of Helmert contrast analysis for the kinematic variables of lower trunk and pelvis.
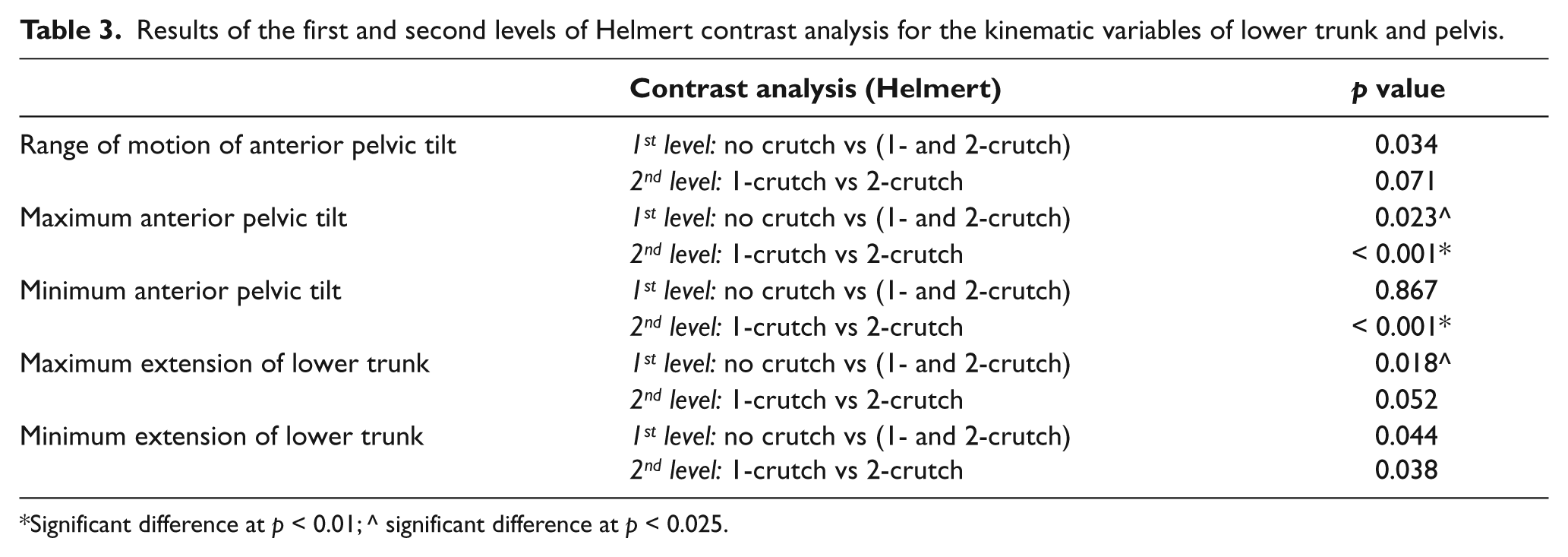
Significant difference at p < 0.01; ^ significant difference at p < 0.025.
The normalized EMG data were transformed into a linear envelope through full-wave rectification and low-pass filtered. Two EMG parameters, peak and mean EMG, were then determined. Despite careful instructions with demonstrations and practice, the normalized EMG data of Participant 5 were found to be greater than one and were discarded for subsequent analysis. This may be due to the fact that muscle activity during a functional task can be greater than that elicited in isolation (i.e. during MVC) in people with neurological impairments. No interaction effect was found between the walking condition and side factors and significant difference was found in both peak and mean EMG which were lower during crutch walking (Figure 4). Subsequent contrast analysis on the mean EMG revealed significant difference at the first level but not at the second level of contrast (Table 2).
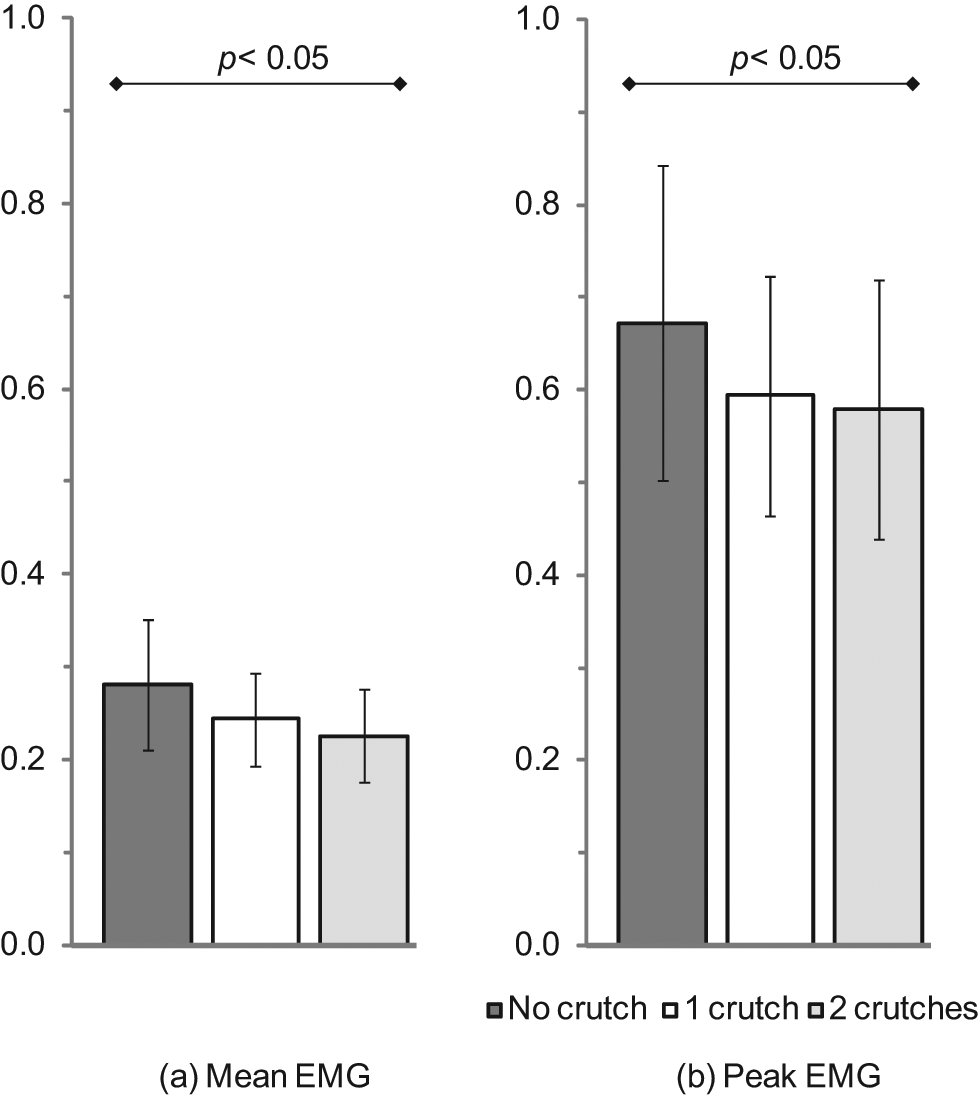
Pooled result of (a) mean electromyography (EMG) and (b) peak EMG of the nine participants (participant 5 excluded) during walking without crutch, walking with unilateral crutch on dominant side and walking with bilateral crutches.
Discussion
Prevalence of CP is around two to three people per 1,000 live births in the population. 30 Spastic diplegia constitutes the most common type of CP and around 30–50% of young people with diplegia are ambulatory. 31 Harada et al. 32 found that 44% of ambulatory dipelgics experienced low back pain and none of their respondents experienced back pain below age nine versus 38% between ages 10–19. Hip flexion contracture is common in diplegia.33,34 In this study, hip flexion contracture ranging from 10–30° was found in three out of the 10 participants (Table 1). Insufficient hip extension during gait is absorbed mostly at the lumbosacral joint with increased anterior pelvic tilt and lumbar hyperlordosis. The more severe the hip flexion contracture, the greater the probability of low back pain in later years. 35
As a first step in understanding the effect of a walking aid on back biomechanics, Lofstrand crutch was selected for its better support in comparison to canes and because it was less obstructive in marker tracking in comparison with frames and wheeled walkers. The temporal-distance parameters revealed that the participants walked significantly slower during crutch walking. The use of crutch(es) enlarged the base of support during swing and stance phases that contribute to a more stable gait. The improved stability did not bring about a significant change in stride length but instead an extended stride time that has resulted in a lower cadence and a slower walking speed. It is postulated that the participants benefited from the slower walk by allowing them more time to control their movements.
The EMG findings indicated a reduced erector spinae activity during crutch walking. Both peak and mean EMG of the erector spinae were significantly lower when the crutch(es) was used. However, no significant difference was found between unilateral and bilateral crutch walking (Table 2). Reduced muscle work of erector spinae as reflected by a reduction in its EMG activity may reduce stress at back, and hence reduce the risk of developing back problems in the future. It has been reported that the energy requirement of people with spastic CP was three times higher than a normal counterpart of comparable age. 36 With proper gait training with the use of crutch(es), the reduced back muscle activity together with an extended stride time may allow people with spastic CP to walk at a lower metabolic cost. Further study on the role of Lofstrand crutch(es) in reducing energy consumption of its user during gait is recommended.
A strong association exists between ambulation and spondylolysis/spondylolylisthesis in ambulatory individuals with diplegia. Murphy 37 found that spondylolysis at L5–S1 was common in ambulatory individuals with diplegia and, if not diagnosed early, might progress to spondylolisthesis. In a study of lumbar spine in spastic diplegia, Harada et al. 32 found that chronic back pain occurred in 75% of their subjects with lordosis > 70°, in 55% of those with spondylolysis and in all subjects with spondylolisthesis. Neither spondylolysis nor spondylolisthesis were detected in non-ambulatory individuals with CP 38 and the prevalence of spondylolysis among weight-bearing individuals with CP was lying between 21% and 30%.39,40 The present study attempted to ascertain the effects of crutch walking on factors (e.g. hyperlordosis) that may predispose sypondylolysis/spondylolylisthesis in spastic diplegia. Kinematic data revealed that the amplitude of sagittal pelvic motion was significantly increased during crutch walking. This was accompanied with a significant increase in anterior pelvic tilt particularly during bilateral crutch walking. Biomechanically, with the body CG shifted forward, an internal extension moment should be generated so as to prevent the body from toppling forward. In the absence of the crutch(es), back extensors will be called into action. Due to the short leverage of back muscle pull, a strong muscle force is needed to counteract the external moment resulting in an excessive stress at back. With the crutch(es) in contact with the floor, the extension moment generated from the ground reaction has adequately counteracted the forward toppling moment. This was supported by the EMG findings with reduced erector spinae activity during crutch walking. The reduced back muscle activity might reduce the stress on the spine. Clinically, adults with CP suffering from chronic back pain are usually walking with hyperlordotic spine that may predispose spondyloysis and spondylolylisthesis, and hence low back pain, in the future. Kinematic data revealed an approximately 6° shift in the sagittal plane motion towards lumbar flexion (i.e. 6° reduction of lordosis) when the crutches were used. This finding may have implications for back pain management among adolescents and adults with the spastic type of CP.
The presence of pain makes a physical disability more difficult to manage and a vicious cycle exists between back pain and ambulation deterioration. In the lifespan approach, therapists have the responsibility of balancing ambulation capacity, preventing potential back pain as well as managing existing back pain for ensuring maximal participation. A passive approach, such as ultrasound, heat and transcutaneous electrical stimulation, provided only short-term pain relief. 20 Previous attempts on active approach (e.g. swimming, exercises) in pain management for people with CP have demonstrated promising results, particularly for the ambulatory ones.41-43 As spondylolysis and spondylolisthesis are underlying causes contributing to chronic back pain among ambulatory individuals with diplegia, an active approach directed at the removal of their predisposing factors may break the vicious cycle. Murphy 37 reported that minimizing anterior pelvic tilt in ambulatory children with CP might prevent spondylolysis in later years. Prosser et al. 44 demonstrated continuous back muscle activation during gait in children with CP and training on reducing excessive muscle activity during walking was recommended. Although walking speed, back muscle activity and lumbar hyperlordosis were reduced during crutch walking, it was accompanied with an increased anterior pelvic tilt. Thus, the use of Lofstrand crutches with four-point reciprocal gait may be considered on a short-term basis as an adjunct to the active approach of managing a current attack of back pain by reducing stress at back during ambulation. However, the present study was conducted on participants who were free from back pain and further study on people with CP suffering from chronic back pain is warranted. In addition, effects of other more commonly used walking aids for people with CP, such as a frame and a wheeled walker, should also be investigated.
The major limitation of the study was its small sample size due to its stringent inclusion criteria. All recruited participants were pain free, able to walk unaided for at least 10 m repeatedly and with a demonstrated ability to acquire the reciprocal gait of crutch walking. Since crutch walking was a novel task for six out of the 10 participants, all six walked unnaturally during crutch walking that may contribute to large variation in the obtained results rendering insignificant difference between conditions. Moreover, the attachment of markers and EMG instrumentation created unnatural gait during data acquisition. Irritations arising from the adhesive tapes used to secure the attached hardware were also reported.
Conclusion
This study was a first attempt to establish the role of a walking aid on whole body kinematics and back muscle activity among adolescents with spastic diplegia. This study demonstrated that erector spinae muscle worked less during crutch walking. It also revealed that the lower trunk was less extended during crutch walking but accompanied with a more pronounced anterior pelvic tilt. These findings may have implications for addressing back pain issues among people with spastic types of CP in terms of back muscle activation and lower trunk and pelvic kinematics.
Footnotes
Acknowledgements
The authors would like to thank Ms Harriet Ko, Technician, Motion Analysis Laboratory, The Duchess of Kent Children’s Hospital at Sandy Bay, for her assistance during the experiment.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.