
Abstract
Background: There were no recent reports of community-based surveys on the incidence, level and causes of amputation in Japan.
Objectives: To identify any changes in the incidence, level, causes of amputation and gender distribution.
Study Design: A community-based survey.
Methods: The subjects were Kitakyushu-citizens amputated between 2001 and 2005 and selected based on medical certificates for the physically disabled person’s certificate.
Results: The incidence of amputation (/100,000 population per year) was 6.9 overall, 1.4 for upper limbs and 5.8 for lower limbs. The average age at amputation was 63.5 ± 20.1 years and the male:female ratio was 1.9:1. The most frequent levels of amputations were partial hand amputation (84.4%) for upper limbs, and transtibial amputation (42.3%) and transfemoral amputation (36.8%) for lower limbs. The major causes were injuries (54.3%) for upper limbs, and peripheral vascular disorder (49.0%) and diabetes mellitus with peripheral circulatory complications (28.6%) for lower limbs.
Conclusions: The incidence of amputation was 6.9 overall, 1.4 for upper limbs and 5.8 for lower limbs, and the male:female ratio was 1.9:1. In comparison to a previous survey the percentages of amputation due to peripheral circulatory disorders and injuries increased and decreased, respectively, and the rate of female amputations increased.
This study provides useful data about change of the recent epidemiology of amputation in Kitakyushu, Japan. These data are essential to perform clinical practices in amputation rehabilitation, including prescription of prosthesis, general fatigue for aged amputees, and complication of peripheral circulatory disorders.
Background
The incidence of amputation in Europe and the USA ranges from 10–60/100,000 population.1-6 Dillingham et al. conducted a nine-year survey covering 11 states in the USA from 1988 to 1996, and found that the incidence of amputation was 52.4/100,000 population per year, wherein 82% were due to peripheral vascular disorder. 4 The incidence of amputation due to peripheral vascular disorder increased from 38.3 to 46.2 during this nine-year period, trauma-related amputation decreased from 11.4 to 5.9, and amputation due to malignant tumors slightly decreased from 0.6 to 0.4, while congenital deficiency accounted for 0.8% of all amputations without any change. The most frequent cause of amputation in Japan had been trauma but recently the percentage of amputations due to peripheral circulatory disorders, such as arteriosclerosis obliterans and diabetic gangrene, is increasing. There have been no recent reports of community-based surveys on amputation in areas representing average life expectancy of Japan, and there is no sufficient information on the current incidence and causes of amputation in Japan.
According to a survey by Sawamura 7 on amputation based on the physically disabled person’s certificate in 20 cities in Hyogo Prefecture in Japan for the 25-year period from 1968 to 1992, the incidence of amputation was 6.2/100,000 population per year, and trauma accounted for 70% of the causes of amputation. Although there were no changes in the total number of amputations during those 25 years, the percentage of amputations due to arteriosclerosis obliterans and diabetes mellitus was increasing. 7 According to a survey on amputation based on the physically disabled person’s certificate in Okayama Prefecture for the five-year period from 1984 to 1988, they reported that 58.2% of lower limb amputations were caused by peripheral circulatory disorder. 8 Hayashi et al. conducted a mail survey of lower limb amputees whose prosthetic legs were made during the six-year period from 1992 to 1997, and reported that peripheral circulatory disorder was the cause in approximately 3% of subjects who underwent amputation before the 1960s, but had increased to 37% among the subjects who underwent amputation in the 1990s. 9 These reports from Japan are of surveys conducted from the 1980s to 1990s,7-9 and recent data are unknown. In addition, the residential areas and details of these subjects are unclear,7,9 only amputation due to peripheral vascular disorder has been surveyed, 8 and the incidence of amputation is unclear due to lack of any community-based surveys. 9
An appropriate community-based survey in an area representing an average population of Japan is required to uncover the incidence and causes of amputation in Japan. Kitakyushu City is a local city with a population of one million and is believed to reflect the average condition of Japan.10,11
The purpose of this study was to perform a community-based survey of amputation based on the physically disabled person’s certificate in Kitakyushu City, and to reveal whether there are any changes in the incidence, level and causes of amputation and also in gender. Our hypothesis is that the incidence of amputation due to diabetes mellitus and peripheral vascular disorders has increased in Kitakyushu City.
Methods
The physically disabled person’s certificate is an official certificate for persons with physical disabilities such as hemiplegia, spinal cord injury, amputation, etc. An amputee with such certification can receive benefits for medical expense, prosthesis, wheelchair, and cane, tax reduction or exemption, disability pension, and social welfare support depending on the classification and grade of their disability. A person who has undergone amputation asks a designated physician under Article 15 of the Act on Welfare of Physically Disabled Persons to make a medical certificate. It includes descriptions of the site and cause of amputation, muscular strength, range of motion, and activities of daily living, and applies for this certification with this medical certificate at the disabled citizens’ welfare division in the ward office where they are registered as a resident. One of the authors (KH) judges all applications from patients registered as residents in Kitakyushu City at the Kitakyushu Disabled Citizens’ Welfare Center, and determines the classification and grade of each disability. Even if a Kitakyushu citizen undergoes amputation at a hospital outside Kitakyushu City, the application is sent to the same center to determine the classification and grade. This certification is greatly beneficial to amputees and they generally obtain the certification within two months after amputation or within two years. It is possible to investigate the situation regarding all amputees in Kitakyushu City when a survey on amputation is conducted based on these medical certificates because the rule provides that the Welfare Center shall keep all of these medical certificates for 10 years.
The subjects of this study consisted of Kitakyushu citizens who underwent amputation from January 2001 to December 2005. The study collaborator (KH) viewed 18,150 medical certificates examined at the Welfare Center from January 2001 to December 2007, and 349 subjects who underwent amputation from January 2001 to December 2005 were selected under the supervision of one of the authors (KH). Based on the descriptions in the medical certificates, the age at amputation, gender, and site, number, and cause of amputation were examined. The number of amputations was determined based on the patients’ medical certificates. The sites of amputation were classified into: upper limb amputation, including forequarter amputation, shoulder disarticulation, transhumeral amputation, elbow disarticulation, transradial amputation, wrist disarticulation, and partial hand amputation (transcarpal, transmetacarpal and transphalangeal); and lower limb amputation, including hemipelvectomy, hip disarticulation,transfemoral amputation, knee disarticulation,transtibial amputation, ankle disarticulation, and partial foot amputation (Chopart, Lisfranc, transmetatarsal and toe). The causes of amputation were classified based on the International Classification of Disease 10 (ICD10) 12 into malignant neoplasm, diabetes mellitus with peripheral circulatory complications (diabetic gangrene, diabetic peripheral angiopathy, etc.), peripheral vascular disorder (arteriosclerosis of arteries of extremities, thromboangiitis obliterans, arterial embolism and thrombosis, acute artery occlusion, varicose veins of lower extremities with ulcer, etc.), infection (cellulitis, decubitus ulcer, ulcer of lower limb, infectious arthropathies, osteomyelitis, etc.), injuries, burn/frostbite, and congenital malformation.
The survey results were input into a commercially available aggregation software program. Age is presented as mean ± standard deviation. The SPSS 11.0J software package (SPSS Japan, Tokyo) was used for statistical processing. Amputations were separated into three groups based on the three most frequent causes, peripheral vascular disorder, diabetes mellitus with peripheral circulatory complications and injuries. Comparisons of the age at amputation between the three groups were conducted using a one-way analysis of variance and the Bonferroni test, with a significance level of 5%. In addition, this study was reviewed and approved in advance by the institutional committee of the ethics at Kitakyushu Disabled Citizens’ Welfare Center, where the actual data were collected.
Results
Profile of amputation and incidence
The population of Kitakyushu City in January 2003 was 1,006,333 11 and the incidence of amputation per 100,000 population a year was 6.9 overall (4.6 for male and 2.4 for female). The male:female ratio was 1.9:1, and the median age at amputation was 66 years of age (interquartile range: 25; 62 years of age for males and 77 years of age for females). Subjects 65 years old or over comprised 55.4% of all subjects, and lower limb amputation was 79.9% of all amputations (Table 1).
Profile of amputation and incidence in Kitakyushu City.
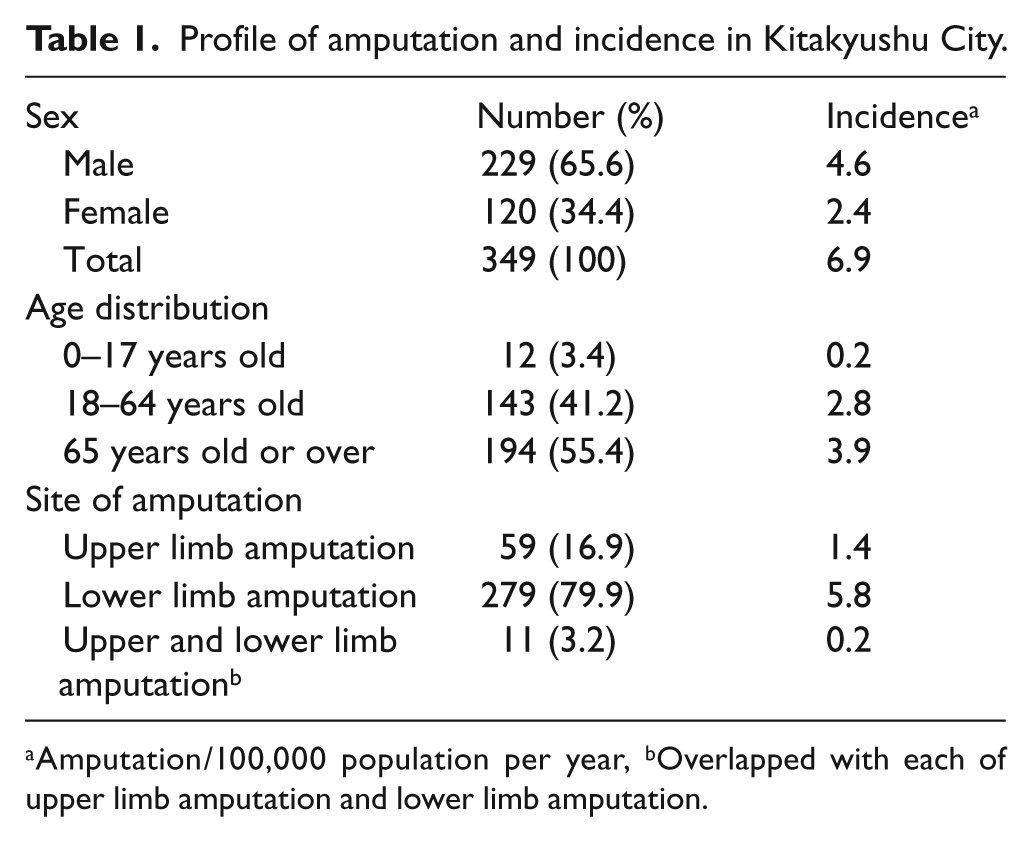
Amputation/100,000 population per year, bOverlapped with each of upper limb amputation and lower limb amputation.
Initial amputation included 264 subjects, thus accounting for 75.6% of all cases, a second amputation included 41 subjects (11.7%), a third amputation included two subjects (0.6%), a fourth amputation included two subjects (0.6%) and an unknown number of amputations included 40 subjects (11.5%).
Level of amputation
Partial hand amputation, such as finger amputation, was the most common among the 77 upper limb amputations (including seven cases of bilateral amputation), accounting for 84.4% (Table 2). On the lower limb transtibial amputation accounted for 42.3% (including 57 cases of bilateral amputation) and transfemoral amputation for 36.8% (Table 2).
Level of amputation in Kitakyushu City.
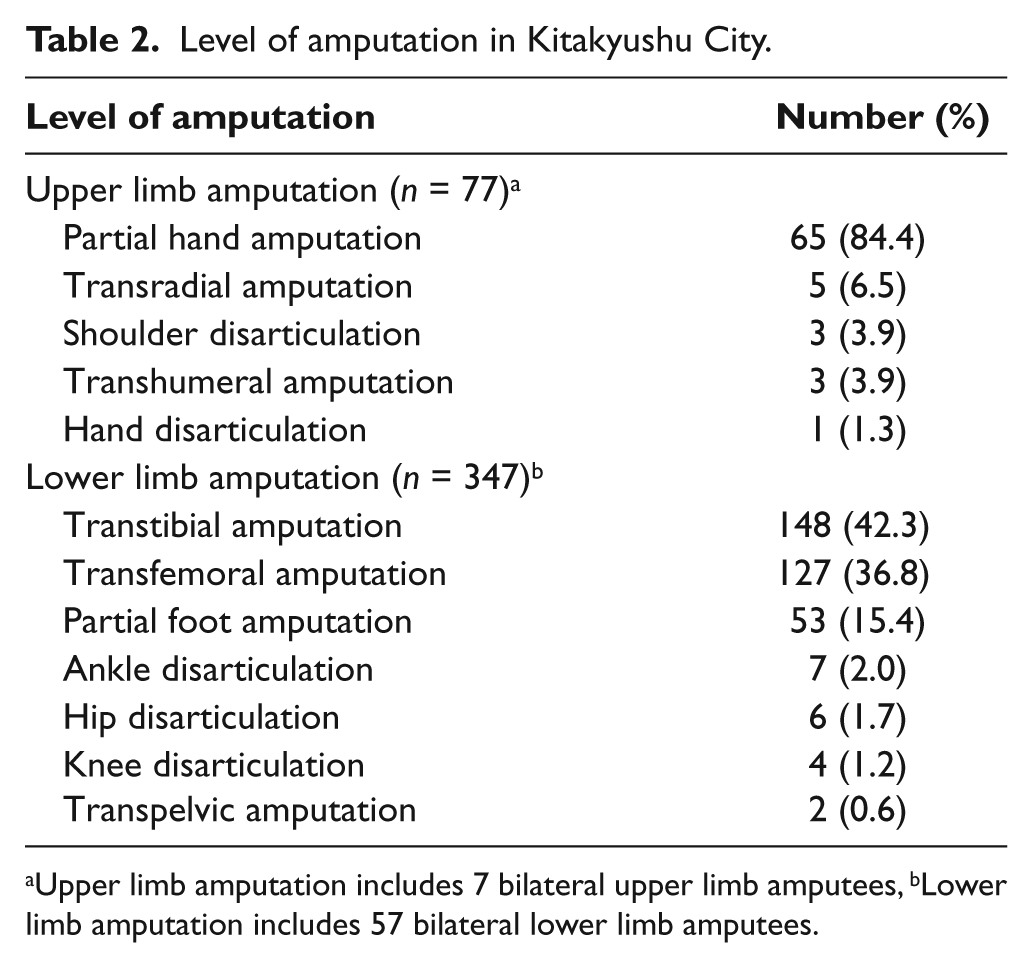
Upper limb amputation includes 7 bilateral upper limb amputees, bLower limb amputation includes 57 bilateral lower limb amputees.
Cause of amputation
The causes of amputation included peripheral vascular disorder (41.6%, incidence: 2.9), diabetes mellitus with peripheral circulatory complications (24.6%, 1.7), and injuries (18.3%, 1.3) (Table 3). Peripheral circulatory disorders combining peripheral vascular disorder and diabetes mellitus with peripheral circulatory complications accounted for 66.2% of all amputations, and accounted for 77.6% of all lower limb amputations.
Cause of amputation in Kitakyushu City.
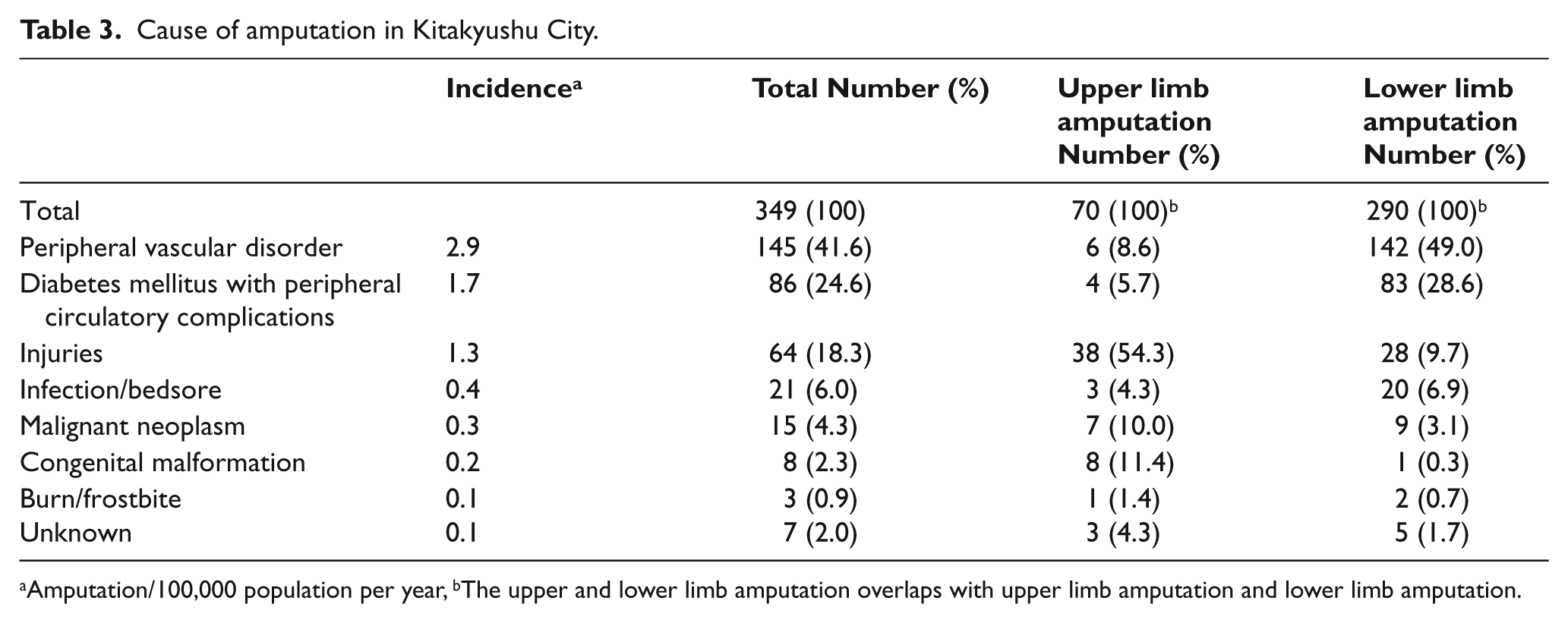
Amputation/100,000 population per year, bThe upper and lower limb amputation overlaps with upper limb amputation and lower limb amputation.
The causative diseases by age group are shown in Table 4. Peripheral circulatory disorders accounted for 83.5% of the elderly subjects aged 65 or over, injuries accounted for 33.3% of middle-aged and young subjects, and congenital malformation accounted for 66.7% in children. Moreover, the average ages at amputation were 75.6 ± 13.6 years, 62.6 ± 13.6 years, and 48.5 ± 19.0 years for peripheral vascular disorder, diabetes mellitus with peripheral circulatory complications, and injuries, respectively, with significant differences between the three groups (one-way ANOVA, Bonferroni test, p < 0.05).
Classification by age and etiology in Kitakyushu City.
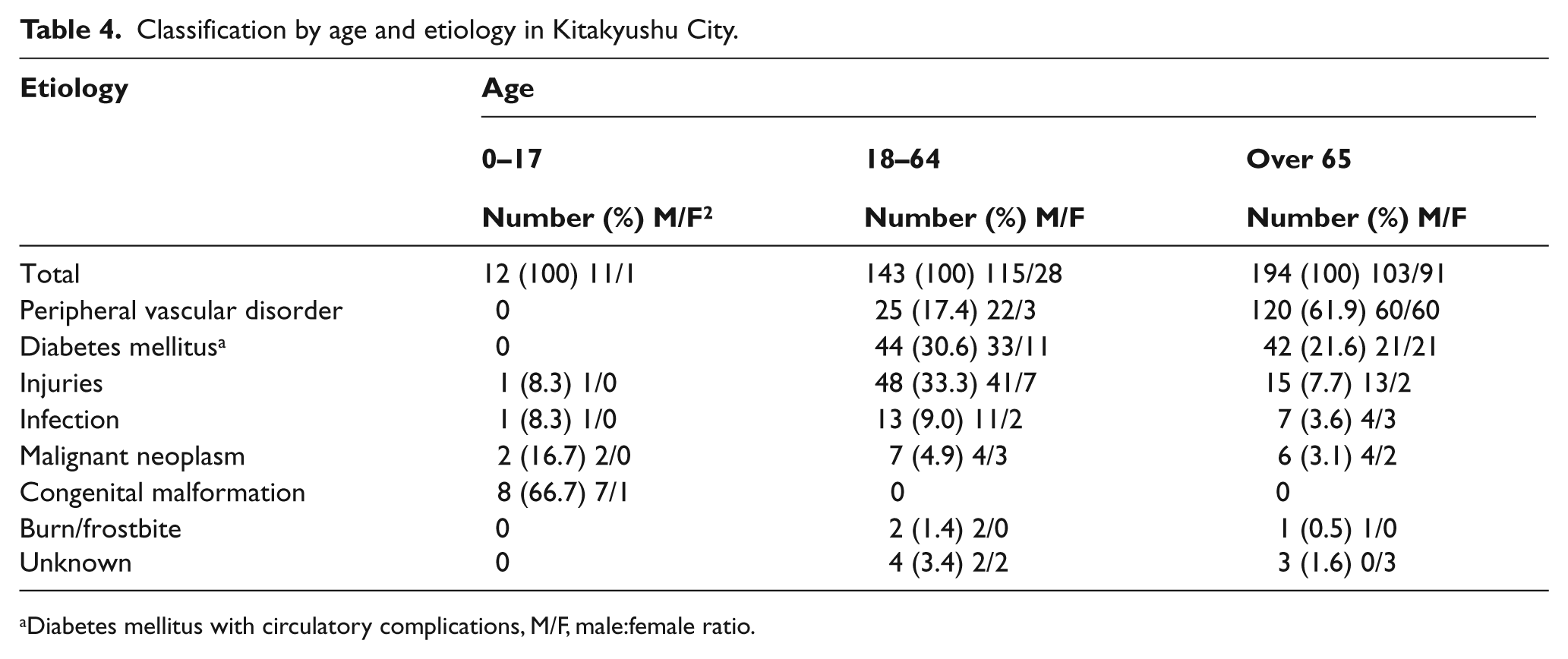
Diabetes mellitus with circulatory complications, M/F, male:female ratio.
Discussion
The analysis revealed: (1) the overall incidence of amputation was 6.9, specifically 1.4 for upper limb amputation and 5.8 for lower limb amputation; (2) the male:female ratio was 1.9:1, with an increased number of female amputees; (3) peripheral circulatory disorder combining peripheral vascular disorders and diabetes mellitus with peripheral circulatory complications accounted for 66.2% of all causes of amputations.
Kitakyushu City has a high level of medical care, amputation is performed at general hospitals in the city, and the prescription of prostheses and relevant rehabilitative training are also implemented in rehabilitation hospitals in the city. Both the physicians and rehabilitation staff have a good knowledge of the system of the physically disabled person’s certificate and recommend that all amputees obtain the certificate. In addition, although it is likely that there were a few patients who died in the early stage after amputation as well as an exceptional patient who did not wish to apply for the certification, almost all amputees obtained such certification. Therefore, the incidence of amputation could be obtained at a high level of accuracy by conducting a survey on amputation among Kitakyushu citizens based on the medical certificates of the physically disabled person’s certificate. Furthermore, as of 2003, the age distribution and male:female ratio of Kitakyushu citizens were close to the respective national values, and the standard of living was also comparable to the national average,10,11 so the results of this survey on amputation are considered representative of the average situation in Japan.
Incidence and level of amputation
The incidence of amputation in the current survey was almost the same as that reported by Sawamura 7 (6.9 vs. 6.2; Table 5). Unwin conducted a survey on amputation in 10 cities with a population of 200,000 or more in six countries, 13 and the incidence of lower limb amputation (/100,000 population per year) was 3.8 in Japan, 2.8 in Spain, 6.9 in Italy, 9.2 in Taiwan and 16.4–19.8 in Britain and 34.9–43.9 in North America. Lower limb amputation was more frequent in Europe and the USA than in Japan, and peripheral vascular disorder was involved as the major cause. The incidence of lower limb amputation in Japan was 5.8 according to the current survey, which is higher than the incidences reported by Sawamura 7 and by Unwin. 13 The reason for this is that our survey was conducted approximately 10 years after those surveys, peripheral vascular disorders and diabetes mellitus have increased in number and, furthermore, the selection method of samples may be more accurate. Lower limb amputation has been increasing in Japan, but it has not reached the levels seen in Britain (16.4–19.8 13 ) and North America (34.9–43.9 13 or 47.23 4 ).
Comparison of amputation between current and previous studies in Japan.
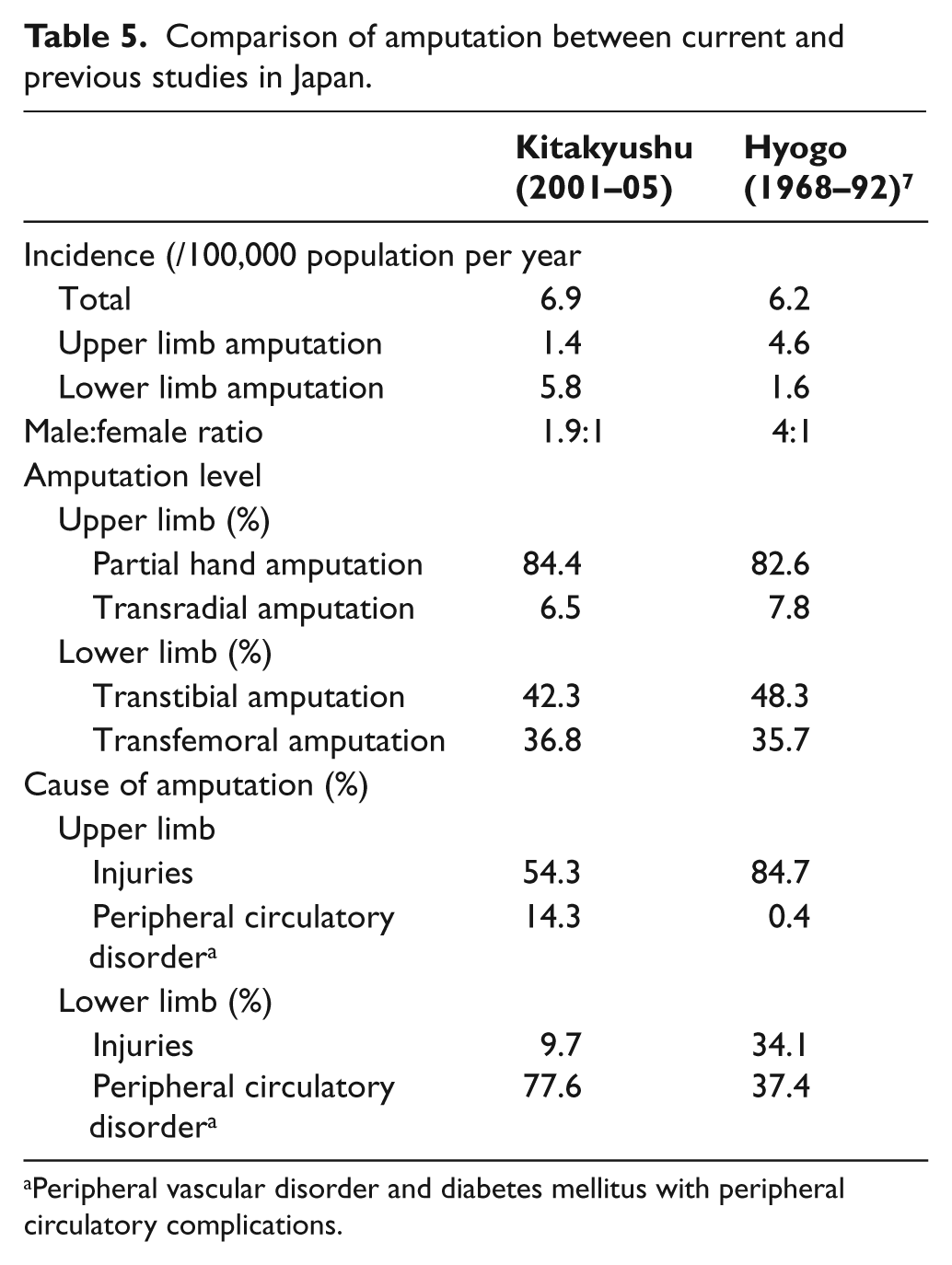
Peripheral vascular disorder and diabetes mellitus with peripheral circulatory complications.
Partial hand amputation accounted for 84.4% of upper limb amputations. Sawamura reported that a partial hand amputation accounted for 82.6%, 7 and Dillingham et al. showed that partial hand amputation accounted for 91.7%. 4 It is believed that there are neither changes in the percentage of the sites of upper limb amputation over time nor in the differences between Japan and the USA.
Transtibial amputation accounts for 42.3% of lower limb amputation, transfemoral amputation for 36.8%, and partial foot amputation for 15.4%, and these results are almost the same as those reported by Sawamura 7 . Dillingham et al. 4 reported that transtibial amputation accounted for 28.0%, transfemoral amputation for 26.0%, and partial foot amputation for 43.6%, and these percentages greatly differ from the current results. The difference in the percentages of lower limb amputation may derive from the frequency and severity of peripheral circulatory complications, method of medical and surgical intervention, and physical constitution of each individual amputee (Table 2).
The male:female ratio
The male:female ratio of amputation was 1.9:1 in this survey, and the percentage of females is steadily increasing from 4:1 in the survey by Akashi et al. in the 1970s, 14 3:1 in the survey by Nagashima et al. in the 1980s, 8 and 3.6:1 in the survey by Hayashi et al. in the 1990s. 9 This male:female ratio of 1.9:1 is equivalent to that in Finland according to Heikkinen et al. 6
Cause of amputations
Peripheral circulatory disorders were the most frequent cause which comprised 66.2% of the overall amputations in the current series, whereas the survey by Sawamura 7 indicated 10.7% of the overall amputations to be due to peripheral circulatory disorders. Therefore, instead of a decrease in the number of amputations due to injuries, amputations due to peripheral circulatory disorders have increased (Table 5).
Dillingham et al. described the percentage of vasogenic amputations to be over eight times higher than that of traumatic amputations and increased by up to 27% in nine years, but traumatic amputations and neoplastic amputations decreased by 0.2% and 42.6%, respectively. 4 This is because factors such as diabetes mellitus, hyperlipidemia, and smoking have increased the percentage of vasogenic amputations and, furthermore, traumatic amputations have decreased due to improved safety measures and progress in limb-conserving surgery.
A survey on amputation by Hanspal among 5,767 subjects in Britain revealed that lower limb amputation accounted for 92% of all cases of amputation, 15 72% of which were caused by peripheral circulatory disorder, and half of them were caused by diabetes mellitus. On the other hand, upper limb amputation accounted for 5% of all the amputations, 56% of which were due to injuries. The percentage of lower limb amputations due to peripheral circulatory disorders in the current study was consistent with that reported by Hanspal. 15
The age at amputation may differ depending on the causes of amputation. Persons with vascular amputation were older than those with diabetic amputation, and persons with diabetic amputation were older than those with traumatic amputation. Nagashima et al. also reported that the age at amputation due to arteriosclerosis obliterans is 74.5 years old while the age at amputation due to diabetes mellitus is 61.4 years old. 8 Therefore, the number of amputations due to peripheral vascular disorders are thus considered to increase with age.4,16
Most reports on the incidence of amputation are not based on ‘at risk’ populations, but generally on the total population. Jeffcoate 17 and Johannesson 18 suggested that such incidence may be expressed in terms of the total (diabetic and non-diabetic) or ‘at risk’ (diabetic) population. According to the recent data of the Ministry of Health, Labour and Welfare, the number of patients with diabetes mellitus across Japan is 10,800,000, and it is estimated that 84,000 people are currently suffering from diabetes mellitus in Kitakyushu City. Supposing that the high risk people are patients with diabetes mellitus, the incidence of diabetic amputation in 100,000 high risk people per year is calculated to be 20.5, whereas the incidence of non-diabetic amputation in 100,000 non-diabetic people per year is 5.3. Consequently, the diabetic people face amputation at a 3.9-fold higher rate than the non-diabetic people.
Recent trends of amputation
The current survey indicated that the rate of amputation due to peripheral vascular disorder and diabetes mellitus has increased in Japan. It is believed that the factors for this increase include an extended life expectancy as a result of good healthcare, the growing percentage of elderly persons in society accompanied by the falling birthrate, and more westernized diets in Japan. One representative cohort study in Japan is the Hisayama epidemiology study that has been conducted since 1961, 19 which is a follow-up survey on health among all residents in the town of Hisayama (located 50 km west of Kitakyushu City, with a population of approximately 8,000) as a sample population of typical Japanese subjects. Recently, the rates of obesity, hyperlipidemia, and abnormal glucose tolerance have increased, and regarding the cause of these increases, the carbohydrate energy rate in dietary intake has decreased from 68.6% in 1965 to 57.2% in 2004. However, the lipid energy rate has increased from 15.6% to 24.4% and, among lipids, the percentage of animal lipids has increased from 29.9% to 47.5%. 20 This tendency is seen not only in the town of Hisayama, but also throughout Japan, and it has been reported that excess intake of animal lipids is closely associated with increases in metabolic disorders such as abnormal glucose tolerance. In Kitakyushu City, dietary changes similar to those reported in Hisayama Town have arisen, 20 and these factors may have increased the incidence of lower limb amputation due to peripheral circulatory disorder. There was one limitation associated with this study, namely, we found it difficult to precisely determine the incidence of amputation due to diabetes mellitus. There are two reasons for this. First of all, we could not precisely determine the total number of diabetic individuals in Kitakyushu City. Secondly, it is difficult to identify all diabetes mellitus patients with minor amputation, for example, toe amputation, who have not yet received the physically disabled person’s certificate. In future, it will be necessary to perform a population-based cohort study on the incidence of lower limb amputation in the diabetic and nondiabetic general population in Japan.
Conclusion
This community-based survey on amputation in Kitakyushu City, Japan, revealed the incidence of amputation was 6.9 overall, 1.4 for upper limbs and 5.8 for lower limbs, and the male:female ratio was 1.9:1. Partial hand amputation was the most frequent site of upper limb amputation, and transtibial and transfemoral amputations were the two most frequent sites of lower limb amputation. Peripheral circulatory disorders accounted for 66.2% of all causes of amputations. In comparison to the previous survey in Japan (performed between 1968 and 1992), the percentages of peripheral circulatory disorders and injuries increased and decreased, respectively, and the rate of female amputations increased.
Footnotes
Acknowledgements
We would like to sincerely thank Dr Kazue Hanada, for selecting cases of amputation, Dr Minako Kondo, for preparing the original data, and Ms Miyuki Ohmaru, Director of the Kitakyushu Disabled Citizens’ Welfare Center for cooperation.
This study was conducted with research funding and scholarships for the Department of Rehabilitation Medicine at the University of Occupational and Environmental Health [grant number 21314].
The authors report no conflicts of interest.