
Abstract
The purpose of the study was to evaluate possible differences between genders in amputation incidence, revascularization activity before and survival after amputation. This population-based study was carried out in a well-defined geographical area, where all vascular surgical consultations and reconstructions are performed in one university hospital. All amputations performed in the region during 1990 – 1999 were identified from the hospital central registers. According to patient's identity codes, the Cause of Death Registry of Statistics Finland provided death data. Amputation data were cross-linked with the local vascular registry using identity codes. Women were found to be 8 years older than men (p < 0.0001). Major amputations comprised 73.4% in males and 77.7% in females. The age-standardized amputation incidence among males was 338 and among females 226 (per 106 inhabitants/year) (p < 0.001). The most prominent difference was seen in amputations due to trauma, where the age-adjusted major amputation incidence was over three-fold among males compared to females. The proportion of patients who had undergone vascular procedure before amputation was 23% in both genders. Median survival after amputation was 943 days in men and 716 in women (p = 0.01). When the higher age of women was considered, there was no significant difference between the genders. Survival was poorer among diabetics in both genders and the difference was significant in males. The amputation incidence was found to be higher in men compared to women in all etiologic subgroups except malignant tumour. Almost one in 4 patients had undergone vascular surgical reconstruction before amputation in both genders. There was no significant difference between the genders in survival after amputation. Subjects with diabetes had a poorer survival after major amputation than those without diabetes.
Introduction
The amputation incidence in Western countries is fairly fully reported and varies between 100 and 500 per million inhabitants annually (Luther et al. 2000; Lindholt et al. 1994; Ebskov et al. 1994; Wrobel et al. 2001; Pohjalainen and Alaranta 1999). The underlying cause of amputation has been in 80 – 95% vascular disease with or without diabetes (Wrobel et al. 2001; Pohjalainen and Alaranta 1999; Morris et al. 1998). During recent decades the treatment of chronic critical limb ischaemia became more active. The rate of vascular reconstructions has increased (Lindholt et al. 1994; Ebskov et al. 1994; Luther 1994) and the proportion of patients who had undergone a vascular surgical procedure before amputation increased (Luther 1994). Patients with amputations are usually elderly with several co-morbidities and survival after amputation is thus often short (Lepäntalo and Mätzke 1996; Feinglass et al. 2000). Despite the considerable number of studies on critical limb ischaemia and amputations, there are only few concentrating on gender differences and those which do exclude amputations due to trauma or tumour.
The aim of the present study was to evaluate differences between males and females in revascularization activity, amputation incidences and survival after amputation including all amputation etiologies.
Materials and methods
The study was made in a well-defined geographical area in Finland, Pirkanmaa, where all vascular surgical consultations and operations take place in one centre, Tampere University Hospital (TAUH). The amputations have been performed in the university hospital and five district hospitals. During the study period, the population averaged 440,000 inhabitants, of whom 16% were over 65 years of age.
All arterial procedures in the Pirkanmaa region have been collected in the Finnvasc-registry of TAUH from the year 1990. Data include patients' identity code (IC), pre-operative data with risk factors and indications for the procedure, peroperative data with procedure code and anatomy, complications and outcome during the first post-operative month.
Data on all amputations performed during the years 1990 – 1999 in Pirkanmaa were obtained from the anesthesia records of six hospitals. The collected data included identity code (IC), age, sex, date of procedure, procedure code and up to three diagnoses. According to the ICs, the Cause of Death Registry of Statistics Finland provided the dates and causes of death until August 2000. Furthermore, amputation data were cross-linked with the local vascular registry in Tampere University Hospital and all vascular surgical procedures performed before the amputation were included in the final data. Syme amputation and those above were considered as major amputation and amputations distal to ankle joint were considered as minor amputations.
Numbers are expressed as a mean and SD and/or range. The means were compared using Student's t-test. Comparison of proportions was made using Pearson's chi-squared or Odds ratio. A p value less than 0.05 was considered significant. Age-standardized incidence rates were calculated using Pirkanmaa as reference population and using three age groups: <65 years, 65 – 80 years and >80 years. Comparison in long-term survival between the groups was done by using Kaplan-Meier survival analysis and log-rank test. Data analysis was carried out using SPSS/Win (version 9.0).
Results
During the 10-year period, 734 amputations were performed on men and 637 on women, 338 and 277 per million inhabitants respectively (p < 0.01). Women were 8 years older than men (p < 0.0001). Vascular, including both acute and chronic ischaemia, and diabetic amputations comprised over 90% of all amputations in both genders. The most common level of amputation was above the knee and major amputations comprised 73.4% in males and 77.7% in females (Table I).
Basic information on the male and female amputation patients.
1Expressed as number of amputations per million inhabitants per year; 2Includes trans-femoral amputations, hip disarticulations and amputations through knee joint; 3Trans-femoral and Syme's amputations; 4Amputations distal to talocalcaneal joint; 5Patients that had undergone vascular surgical procedure during 1990 – 1999. N.S. Not significant.
Age-adjusted major amputation (above ankle level) incidences were calculated separately in four etiologic subgroups (atherosclerosis (aso), diabetes (including both type I and type II), tumour and trauma) (Table II). Amputation incidence was higher in men compared to women in all subgroups except tumour, and the most prominent difference was seen in amputations due to trauma, where the age-adjusted amputation-incidence was over three-fold among males compared to females.
Age-standardized major amputation1 incidences2 in main etiologic groups.
∗p < 0.05; 1Amputations above ankle level; 2Expressed as number of amputations per million inhabitants per year; 3Vascular etiology without diabetes; 4Diabetes with or without macrovascular disease.
The proportion of patients who that had undergone some vascular procedure was 23% in both genders. There was no significant difference between the genders in any age-group (Table IIIa). Male diabetics had undergone vascular reconstruction more often before the major amputation than female diabetics (27% and 15% respectively, p < 0.01), but in the other etiologic main groups there were no significant differences (Table IIIb, IIIc).
The proportion of amputation patients that had undergone vascular surgical procedure.
∗p < 0.05.
Survival was determined from the amputation date until the patient's death. Median survival in the total material was 821 days being 943 days (95% CI 811 – 1074 days) in men and 716 in women (95% CI 547 – 885 days) (p = 0.01). When the impact of age was taken into consideration by determining survival separately in three age groups, (A) 65 years of age, B) 65 – 80 years of age, C) >80 years of age), there was no significant difference between the genders (Figure 1(A – C)). There was a clear difference in survival after amputation between the three amputation levels.
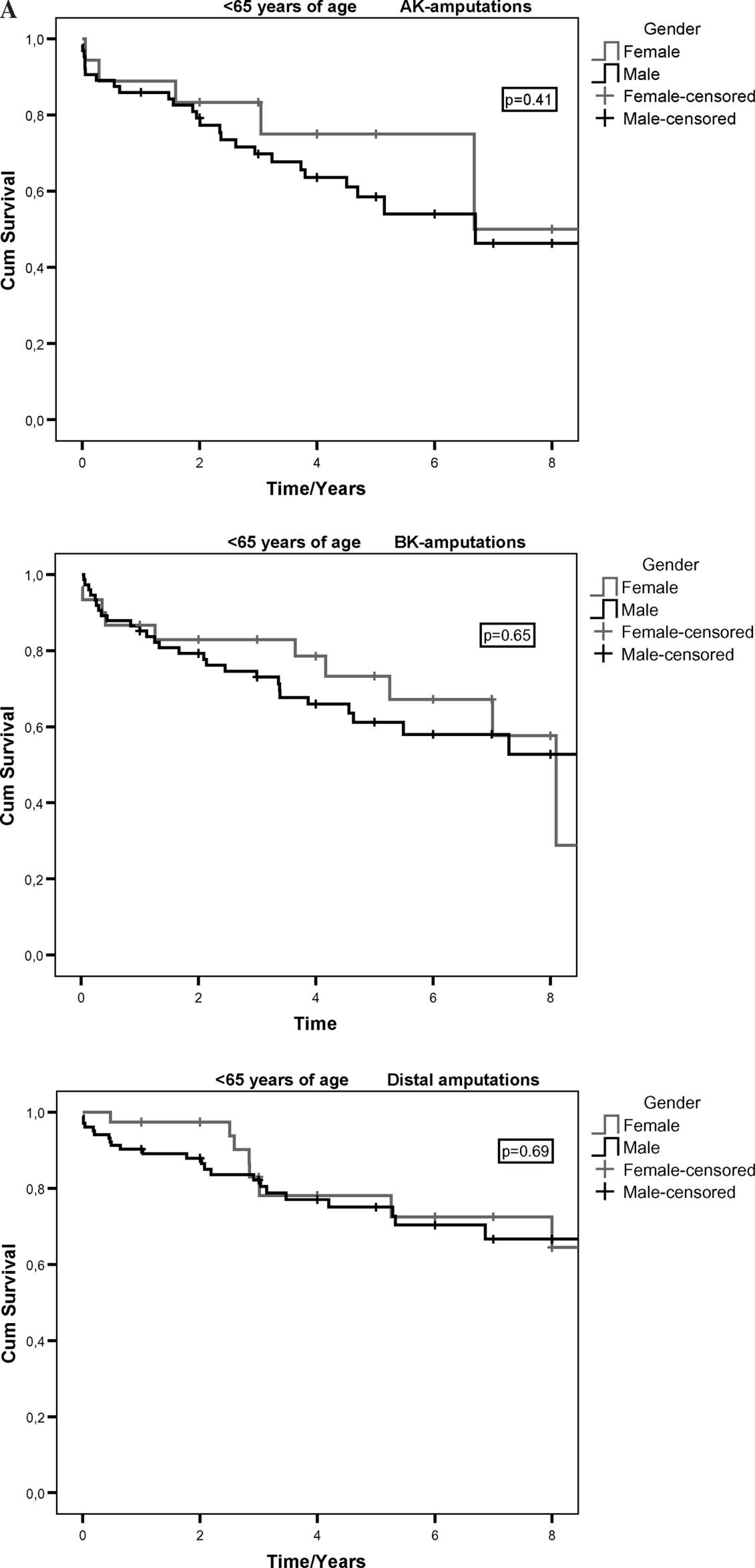
Kaplan-Meier survival curves after amputation according to age group and amputation level.
Although diabetic major amputation patients were younger than vascular patients without diabetes (mean age 76.7 and 73.2 years, respectively, p < 0.01), survival was poorer among diabetics compared to vascular patients without diabetes in both gender and the difference was significant among men. Kaplan-Meier estimates for 1-, 2-, and 5-year survival for diabetic vs. non-diabetic men were 0.51 vs. 0.59, 0.39 vs. 0.50 (log rank test < 0.05) and 0.09 vs. 0.26 (log rank test < 0.01) respectively.
Discussion
Reports on amputation incidence in various populations are relatively frequent. However, they usually include only vascular and diabetic amputations and those due to trauma or tumors have been excluded (Luther et al. 2000; Wrobel et al. 2001; Morris et al. 1998; Luther 1994; Feinglass et al. 2000). Also, reports on gender differences are sparse and include only vascular and diabetic amputations. The present study gives a comprehensive overview of all amputations and survival after in all hospitals in a defined area. Main impact has been paid on gender differences.
The authors found significantly higher amputation incidence among men compared to women in our region, age-adjusted major amputation incidence per million inhabitants being 328 among men and 172 among women. After age-adjustment, the difference became even greater. A higher amputation incidence in males was also found in a study by Feinglass and co-workers (2000) in Northern Illinois. The major amputation rate per million residents was 250 among men and 180 in women. Morris and colleagues (1998) studied lower limb amputation rates in diabetic and non-diabetic cohorts in Tayside, Scotland. They also found a similar gender difference: The amputation incidence per million person-years in non-diabetics was 230 among men and 170 among women.
The corresponding numbers among diabetics were 2810 and 1880. The figures are not directly comparable because the number of diabetics in our region is unknown and incidences are calculated in the total population. Also, in studies by Feinglass et al. (2000) and Morris et al. (1998), traumatic and tumour amputations had been excluded. However, it seems to be that gender difference in the present population is even higher.
Smoking is a significant risk factor for peripheral arterial occlusive disease and amputation. In Finnish population, male smoking is higher (37%) compared to women (20%) and the gender difference in smoking is largest in the oldest age group (Rahkonen et al. 1992). The most prominent difference was seen in the rate of traumatic amputations, where the authors found almost fourfold difference between the genders. In Finland, the age-adjusted incidence of serious injuries per 105 was 1659 among men and 1216 among women in 1995 (Kannus et al. 2001). The highest difference has been in the incidences of road traffic accidents (male vs. female incidence 183 vs. 101 per 105), and in injuries induced by machines and devices (male vs. female incidence 214 vs. 37 per 105) (Kannus et al. 2001). The difference in traumatic amputation incidence correlates well with these differences in serious injury incidences.
Survival after amputation was highly related to the amputation level and age. In unadjusted data, survival of females was lower than that of males, but this difference is totally explicable by the higher mean age of women. After adjusting, the survival of females was even a little even higher that in males, but in no group was there a significant difference. Mean survival after trans-femoral amputation was only 4 months in patients over 65 years of age. This is probably a reflection of the fact that trans-femoral amputation patients are high-risk patients with very poor preoperative health rather than trans-femoral amputation being a more risky procedure than trans-tibial amputation. Pell and Stonebridge (1999) studied the factors affecting survival after major amputation in 2759 patients. Their findings were similar to ours: Age and amputation level were significantly associated with mortality, whereas sex did not predict mortality. Luther (1994) studied survival after major amputation and vascular reconstruction in patients with critical limb ischaemia. In his study, the 1- and 5-year survival rates after amputation were 55% and 20%; the figures from our study are about the same. In Luther's study, 1- and 5-year survival of critical limb ischaemia (CLI) patients after vascular reconstruction was significantly better, 83% and 45% respectively, reflecting the poorer preoperative condition of amputation patients compared to reconstruction patients. In a study of 1560 non-selective CLI patients, Bertele et al. (1999) found 1-year mortality 81%, which is significantly better compared to the present study's patients, whereas Lepäntalo and Mätzke (1996) reported only 46% 1-year survival in patients with unreconstructed CLI. It seems to be that among patients with CLI, there is a group of patients with very poor survival: Elderly patients with widespread CLI that cannot be reconstructed.
Survival after major amputation was significantly poorer among diabetics compared to non-diabetic vascular amputation patients despite the fact that diabetics were significantly younger on average that non-diabetic. Diabetes has been found to increase significantly mortality due to coronary heart disease and stroke in normal population (Laakso et al. 1995; Tuomilehto et al. 1996; Mulnier et al. 2006; Raymond et al. 1995; Whiteley et al. 2005). Among the elderly Finnish population, survival of non-diabetics is better compared to diabetics in both genders. The cumulative 1(4)-year survival in elderly (>70 years) Finnish men with and without diabetes has been 85% (58%) and 90% (69%) respectively and in women 96% (74%) and 100% (92%) (Hiltunen et al. 1998). Compared to these figures, 1(4)-year survival of amputation patients, with and without diabetes, is significantly reduced, being 59% (31%) and 51% (11%) in men and 48% (26%) and 46% (19%) in women in the present study. When performing comparisons between the groups, it has to be remembered that mean age between the groups is not equal. For example, non-diabetic women were significantly older than diabetic women, non-diabetic men and diabetic men.
The rate of vascular surgical procedures among amputees was excactly the same in both genders. This suggests that vascular surgical activity is the same in both genders even if male patients are younger than female. Reconstruction activity before the major vascular or diabetic amputation was lower in females compared to males. This can be due to a higher revascularization activity in male diabetics or a higher failure rate after the revascularization in males. Before a minor amputation, in turn, the revascularization rate was higher in females; this possibly suggesting that reconstructions survive and only minor amputations have to be made.
The present study was based totally on large registries, which involves certain limitations in respect of results. Most vulnerable are hospital discharge registries, the biggest concern being if all the amputations have been registered. However, it can be assumed that systemic error is the same in both genders. Also, in the validation studies, the validity of hospital discharge registers and the cause of death register has been found to be reasonably good (Mähönen et al. 1997). The most important information from the cause of death registry here was the date of death, which is not as vulnerable to error as for example the causes of death. The comprehensiveness of the local vascular registry has been checked annually using the anaesthesia register and missing procedures have been sought from case histories.