
Abstract
Background:
Epidemiological data for work-related traumatic limb amputations are limited worldwide, particularly incidence trends related to workplace characteristics.
Objectives:
To investigate nationwide incidence rates and trends for amputations according to industry and establishment size.
Study design:
Retrospective cohort study.
Methods:
Incidence rates were calculated using workers’ compensation claims in South Korea from 2004 to 2013. Age–sex standardization was conducted, and trends related to workplace characteristics were statistically analyzed using the chi-square test.
Results:
The overall incidence rate was 38.8 claims per 100,000 workers. Decreasing trends over time in age–sex standardized incidence were observed. Most claims occurred in manufacturing and construction industries. Incidence within the manufacturing decreased significantly (p < 0.001), but not in the construction (p = 0.130) industry. Small-sized establishments (<50 employees) accounted for 77.8% of claims. Incidence in small establishments significantly decreased between 2004 and 2013 (p < 0.001).
Conclusion:
A decreasing incidence rate for traumatic amputations in manufacturing and small establishments may imply that preventive measures have been successful in South Korea. If so, these strategies may be useful for other fast-growing Asian economies. Further research is needed to identify the causes of traumatic amputations according to industry and establishment size.
Clinical relevance
Trends in the incidence rate of work-related traumatic limb amputations related to workplace characteristics can provide useful information for policy makers to improve prevention strategies.
Background
Loss of a body part due to trauma is one of the most physically and emotionally devastating injuries. 1 Traumatic amputations result in permanent impairment and disability 2 and also cause acute- and posttraumatic stress disorder. 3 They reduce health-related quality of life, both physically and psychologically. 4 Among traumatic amputations, work-related injuries are considered particularly devastating because of the loss of income incurred during sick leave, in addition to medical expenses. 5 It has been reported that, even after medical treatment, more than half the number of amputees were unable to return to their previous employment or could only work part-time.6,7
Epidemiological studies concerning the incidence rate of work-related traumatic amputations are limited. 2 Despite the importance of obtaining data to develop effective and efficient prevention strategies,8,9 only five studies have been identified that report incidence rates concerning work-related traumatic upper and lower limb amputations, which ranged from 13.6 to 39 amputations per 100,000 workers.8–12 The most prevalent body parts lost to amputation were the fingers (80%–97%).8–12 Manufacturing (29–40 amputations per 100,000 workers), construction (13–32 amputations per 100,000 workers), and agriculture, forestry, and fishing sectors (20.8–59 amputations per 100,000 workers) showed the highest incidence rates for traumatic amputation.9,10,12 However, these reports were not nationwide studies, and all were conducted in the United States. There have been nationwide studies undertaken in Taiwan and Norway; however, these studies only included traumatic upper limb amputations,2,13 or traumatic amputations that had occurred within the manufacturing industry. 14 To date, there have been no epidemiological studies in South Korea that have reported the incidence rate of work-related traumatic limb amputations. One single hospital-based study reported the number of patients with nonspecific traumatic amputations in 1996. 15 However, of all types of amputations, they reported only the proportion of traumatic amputations between 1970 and 1994, without incidence rate.
In addition to the overall incidence rate, studies reporting trends in the incidence rate of work-related traumatic amputations are rare and ambiguous. In two studies undertaken in the United States, 9-year trends in Washington were inconclusive 8 and, in Kentucky, 10-year trends showed decreasing incidence rates. 11 Despite the need for nationwide trend data to evaluate current national policies and develop future plans, we identified only one study that reported decreasing trends in work-related traumatic amputations in the Norwegian manufacturing industry over a 10-year period. 14 Furthermore, there have been no studies reporting trends in the incidence rate of work-related traumatic amputations according to workplace characteristics such as industry and establishment size.
Therefore, this study aimed 1/ to investigate the incidence rate of work-related traumatic amputations, and 2/ to examine trends in the incidence rate of work-related traumatic limb amputations according to industry and establishment size using 10 years of workers’ compensation claims data in South Korea.
Methods
This study was approved by the Institutional Research Ethics Board at the Catholic Medical Center (IRB No. OC17ZESI0088). All records were fully anonymized prior to data analysis. Written informed consent was waived because all data were collected retrospectively.
Data source
The Korea workers’ compensation insurance covers most industrial accidents occurring since June 2000. Ninety-eight percent of all workers at private establishments with more than one employee were included. All injuries causing ⩾4 days off work can be compensated. Industrial accidents that caused these injuries must be reported to the government and a penalty is imposed in cases of failure to do so. From 1 January 2004 to 31 December 2013, 132,683,643 workers had been covered and 923,986 claims for work-related injuries and diseases had been accepted.
The data used in this study were acquired from the Korea Workers’ Compensation & Welfare Services dataset using diagnosis codes assigned by physicians using the International Classification of Diseases, 10th revision (ICD-10). The following variables were included in the dataset: claimant’s demographic information such as age, sex, nationality, and occupation; workplace information such as industry and the number of employees; and medical information such as diagnosis code, detailed injury description, and date of injury.
Study population
The study population comprised workers who claimed compensation for work-related traumatic limb amputation from 2004 to 2013. Cases with amputation-related diagnosis codes and detailed injury descriptions with amputation-related wording were identified. ICD-10 diagnosis codes related to amputation were as follows: S48.0-1, S48.9, S58.0-1, S58.9, S68.0, S68.00-1, S68.1, S68.10, S68.100-9, S68.11, S68.110-9, S68.2-4, S68.40-1, S68.8-9, S78.0-1, S78.9, S88.0-1, S88.9, S98.0-4, T05.0-6, T05.8-9, T11.6, T13.6, T14.5, and T14.7. To minimize the possibility of missing cases, we included diagnosis codes related to crushing injuries such as T14.6 and codes related to a complication of amputation or residual limbs such as T87.3-6, T92.6, and T93.6. An example of a detailed injury description is “right transphalangeal amputation of the index fingers,” as translated from Korean, and cases with detailed injury descriptions containing the words “amputation” or “disarticulation” were included.
Based on diagnosis codes and detailed injury descriptions, affected body parts were classified as follows: elbow-shoulder (shoulder disarticulation, trans-humeral amputation, and elbow disarticulation); forearm-wrist (trans-radial amputation and wrist disarticulation); hand (partial hand amputation above finger level); fingers (digit amputation of upper extremity); with thumb (first digit amputation with or without other digit of upper extremity); without thumb (second–fifth digit amputation of upper extremity); unspecified upper extremity; hip-knee (hip disarticulation, trans-femoral amputation, and knee disarticulation); lower leg-ankle (trans-tibial amputation and ankle disarticulation); foot (partial foot amputation above the level of the toes), toes; unspecified lower extremity; multiple (amputation involving more than one extremity); and unknown. Proximal upper limb amputation (above finger level) included “elbow-shoulder,” “forearm-wrist,” and hand amputation. Proximal lower limb amputation (above the level of the toes) included “hip-knee,” “lower leg-ankle,” and foot amputation. Detailed injury descriptions also provided information on which extremity had been affected (i.e. left or right side.)
Calculation and standardization of incidence rate
The incidence rate was calculated by dividing the number of claims by the number of insured workers and multiplying by 100,000. The annual number of insured workers was provided by the Annual Reports of Industrial Accidents from the Korean Ministry of Employment and Labor at the end of each year. This report also provided the number of insured workers according to industry and establishment size. For year-on-year comparability, sex- and age-standardization was performed based on the Korean economically active population by sex and age group in 2013 16 rather than on workers’ compensation insurance subscriber information, because subscriber data do not provide age and sex information. All incidence rates were analyzed across six age groups (15–19, 20–29, 30–39, 40–49, 50–59, and >60 years) and according to sex.
Statistical analyses
Claim data classification according to industry, establishment size, and affected anatomical part was conducted using EXCEL software version 2016 (Microsoft, Redmond, Washington). Tests for trends in the incidence rate according to industry, establishment size, and affected body part were conducted using a chi-square test for trend, using STATA version 12.0. We used a two-sided p value less than 0.05 in all analyses as the criterion for statistical significance.
Results
This study identified 51,450 accepted workers’ compensation claims for work-related traumatic limb amputations from 2004 through 2013. The incidence rate was 38.8 claims per 100,000 workers (95% confidence interval (CI) = 38.4–39.1). Of the amputated workers, 82.8% were men (average age: 42.9 years), and the mean age increased by 0.5 each year from 41 to 45 years. Koreans accounted for 86.4% of the total cases. The proportion of foreign workers continued to increase from 8.9% to 16.0% over the decade. According to occupation, handlers, helpers, and laborers comprised most cases (35.9%), followed by technicians and related support (17.4%) and machine operators and assemblers (16.4%) (Table 1).
Demographics of work-related traumatic limb amputations in South Korea from 2004 to 2013.
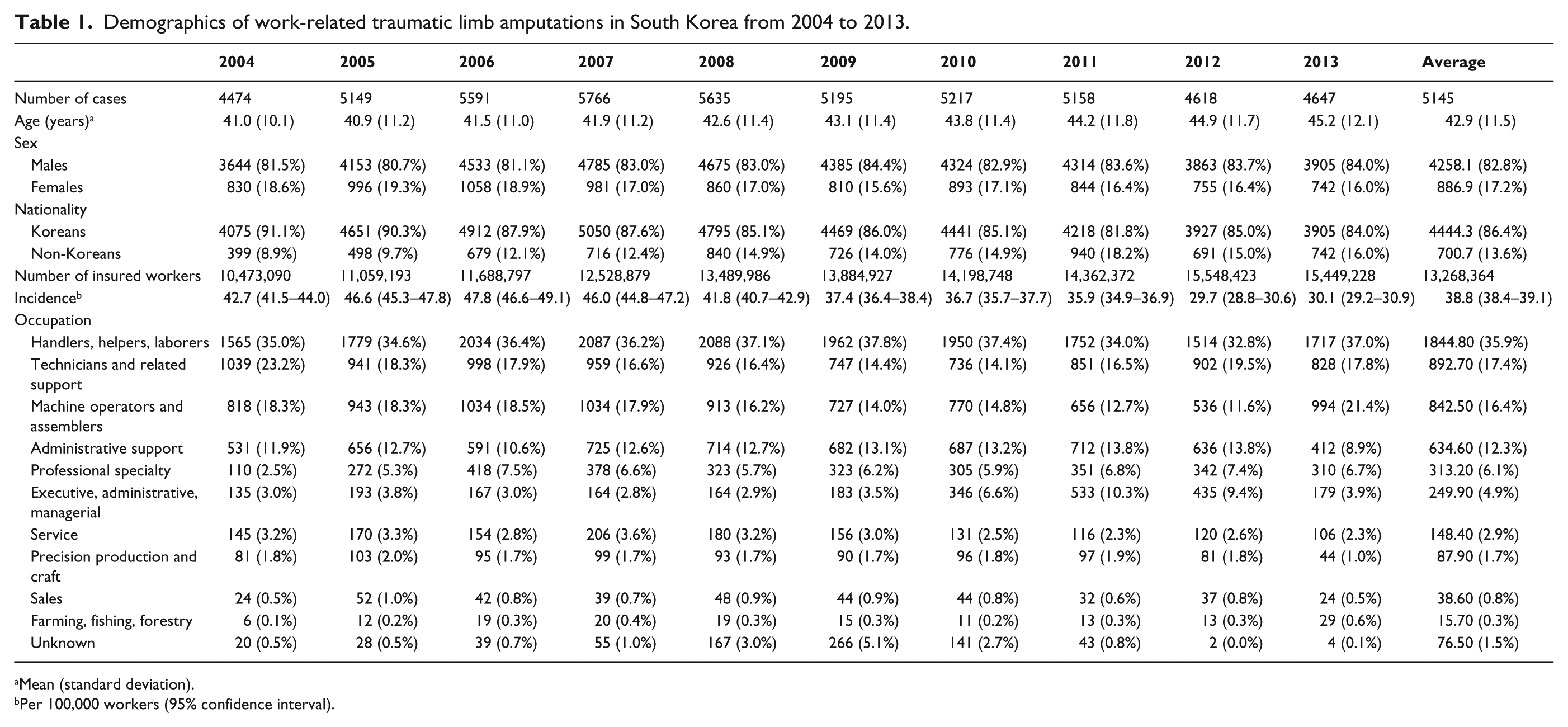
Mean (standard deviation).
Per 100,000 workers (95% confidence interval).
The number of cases of work-related traumatic amputations decreased from 5766 in 2007 to 4477 in 2013. In addition, the age–sex-standardized incidence rate showed a 26.1% decrease from the highest rate in 2007 to the lowest rate in 2013 (Figure 1).
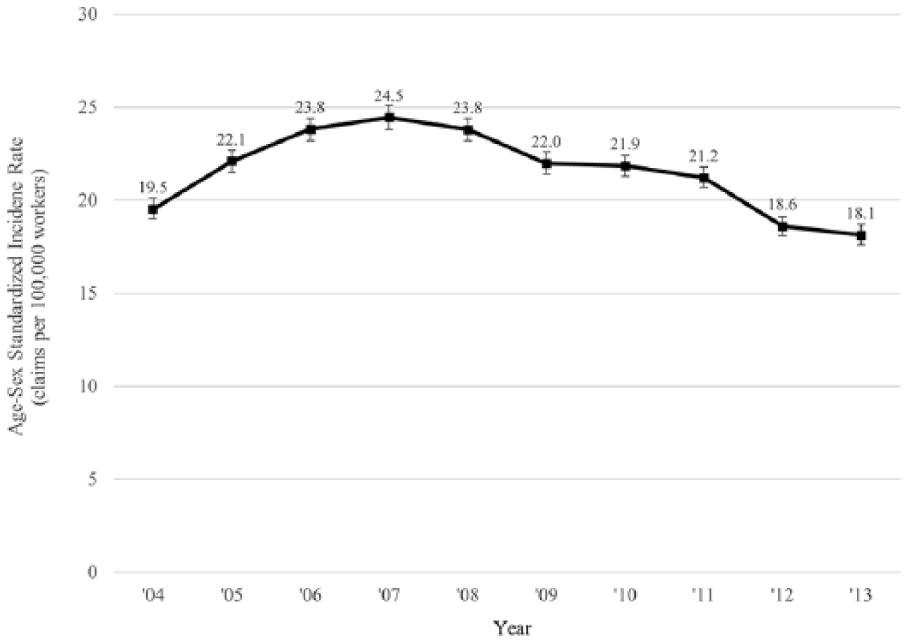
Trends in the age–sex-standardized incidence rate of work-related traumatic limb amputations in South Korea from 2004 to 2013.
We observed that 93.7% of total amputations were finger amputations (95% CI = 93.5%–93.9%). Proximal upper limb amputations above finger level comprised 2.6% (95% CI = 2.4%–2.7%). Proportion of toe amputations was 1.9% (95% CI = 1.8%–2.0%) and that of proximal lower limb amputations above toe level was 0.9% (95% CI = 0.8%–1.0%). Multiple amputations comprised only 0.9% of cases (95% CI = 0.9%–1.0%) (Table 2). Left and right sides were affected almost equally (left side, n = 25,353 claims; right side, n = 25,271 claims). The incidence rate of finger amputation significantly decreased from 44.9 claims per 100,000 workers in 2006 to 27.7 per 100,000 workers in 2013 (p for trend < 0.001). The incidence rate of toe amputation also significantly decreased (p for trend < 0.001) from 0.9 claims per 100,000 workers in 2005 to 0.6 per 100,000 workers. However, the incidence rates of proximal upper limb above finger level and lower limb amputation above the level of the toes did not demonstrate a significantly decreasing trend (p for trend of upper limb = 0.836; p for trend of lower limb = 0.589) (Figure 2).
Frequency and the incidence rate of work-related traumatic limb amputations according to the affected body part in South Korea from 2004 to 2013.
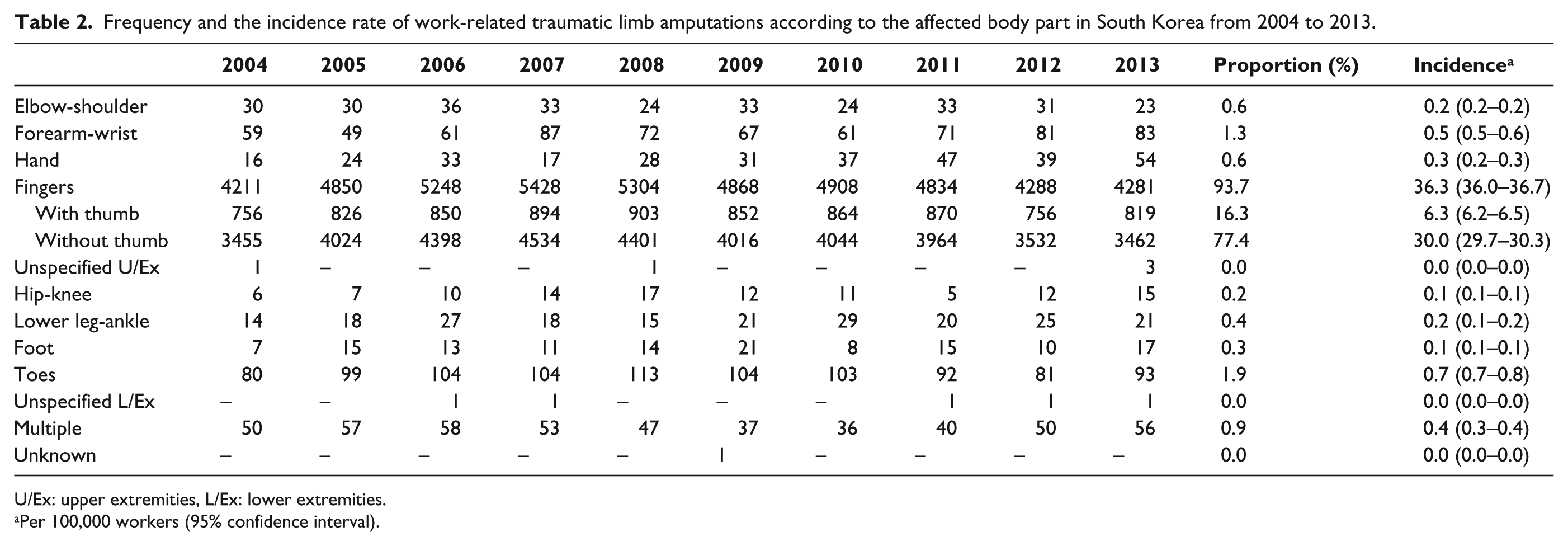
U/Ex: upper extremities, L/Ex: lower extremities.
Per 100,000 workers (95% confidence interval).
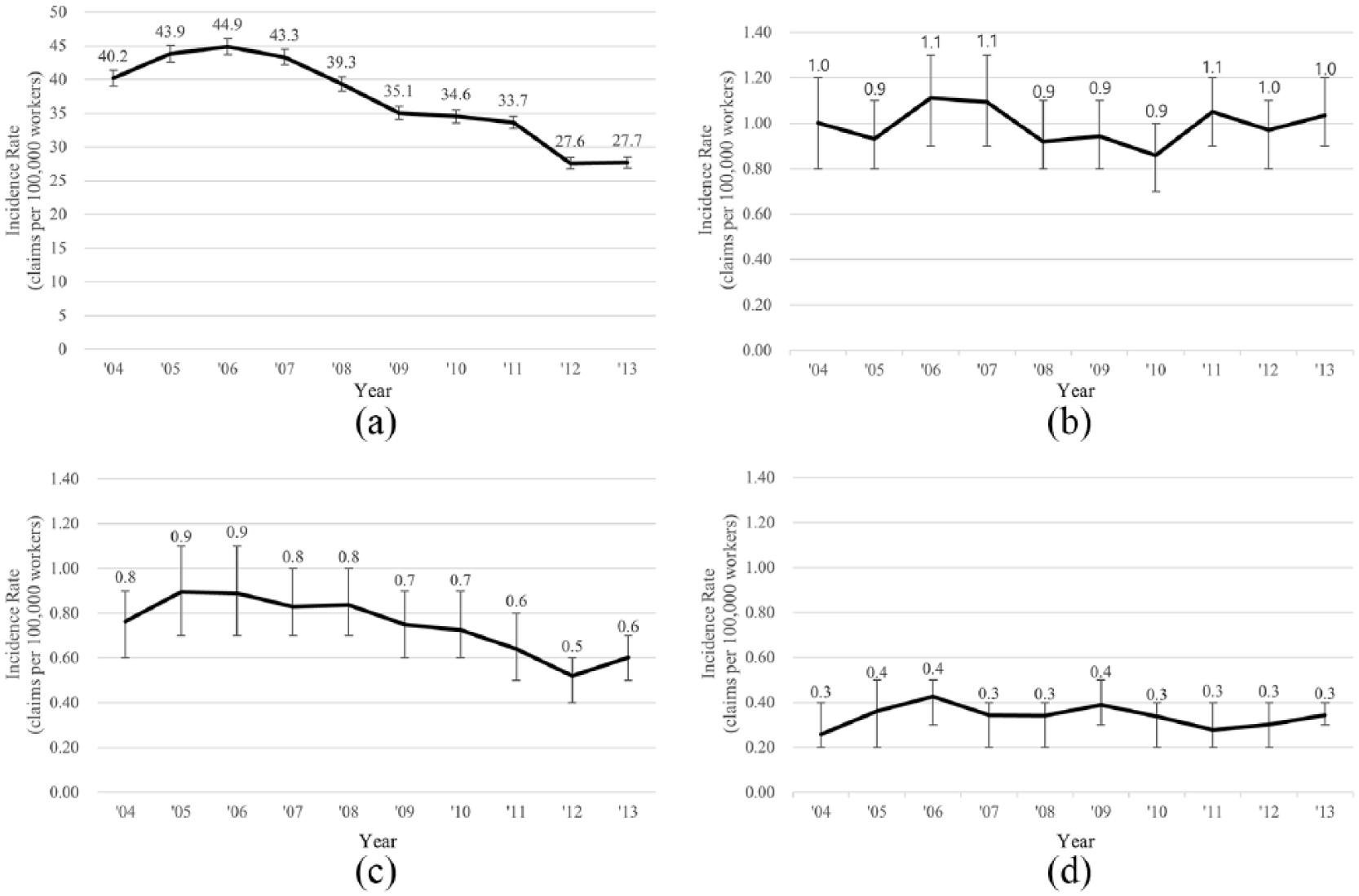
Trends in the incidence rate of work-related traumatic limb amputations according to the affected body part in South Korea from 2004 to 2013: (a) finger amputation, (b) proximal upper limb amputation (above finger level), (c) toe amputation, and (d) proximal lower limb amputation (above the level of the toes).
The three industry sectors with the highest number of work-related traumatic amputations were manufacturing (75.4%, 95% CI = 75.0%–75.8%), construction (10.7%, 95% CI = 10.4%–11.0%), and the transport, storage, and communication industry (1.5%, 95% CI = 1.4%–1.6%). Industry sectors with the highest incidence rate of traumatic amputation were manufacturing (94.4 claims per 100,000 workers, 95% CI = 93.4–95.3), mining (94.2 claims per 100,000 workers, 95% CI = 80.6–107.7), and fisheries (79.2 claims per 100,000 workers, 95% CI = 48.7–109.6). The incidence rate within the construction industry was 15.5 claims per 100,000 workers (95% CI = 15.1–15.9) and 8.7 claims per 100,000 workers (95% CI = 8.1–9.3) within the transport, storage, and communication industry (Table 3).
Frequency and the incidence rate of work-related traumatic limb amputations according to industry in South Korea from 2004 to 2013.
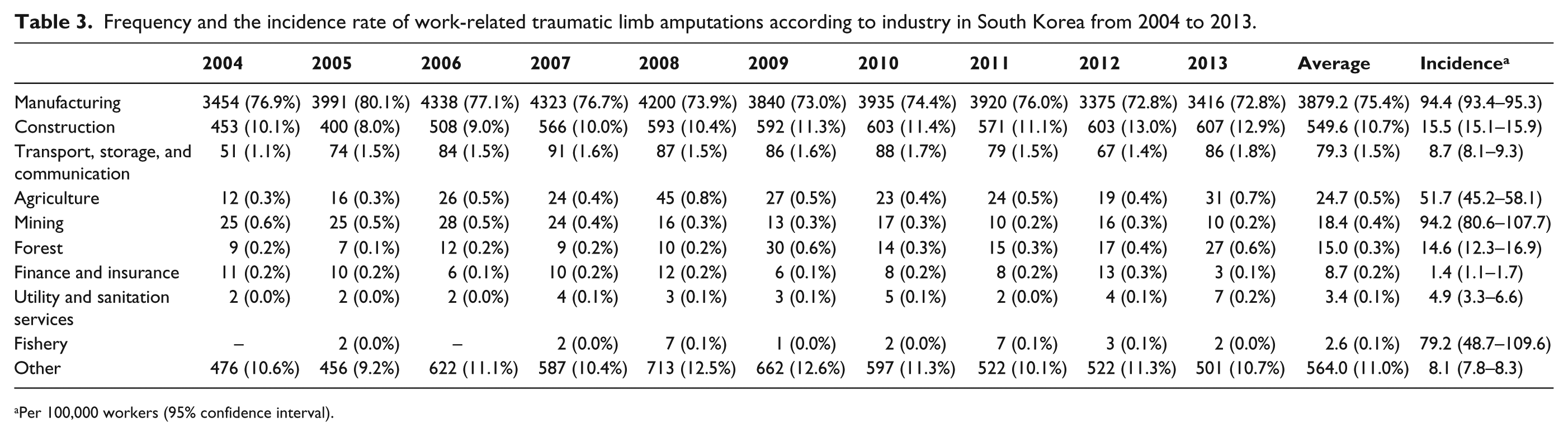
Per 100,000 workers (95% confidence interval).
The number of amputations in the manufacturing sector decreased from 2006. The incidence rate also significantly decreased (p for trend < 0.001). However, the number of amputations in the construction sector did not decrease, nor did the incidence rate (p = 0.130) (Figure 3).
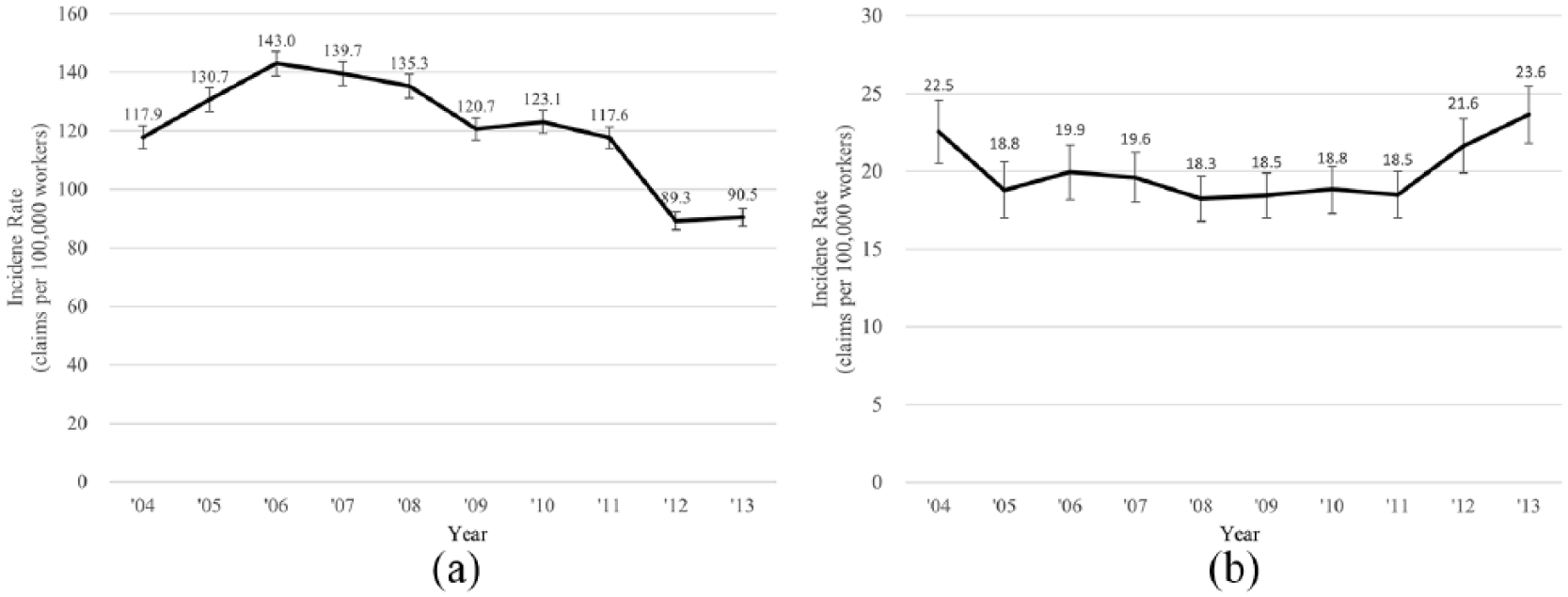
Trends in the incidence rate of work-related traumatic limb amputations according to industry in South Korea from 2004 to 2013: (a) manufacturing sector and (b) construction sector.
According to establishment size, 77.8% of the total cases occurred in workplaces with <50 employees (95% CI = 77.5%–78.2%). We noted that the smaller the size of the workplace, the higher was the incidence rate of amputation. The incidence rate in small establishments (<50 employees) was 57.5 claims per 100,000 workers (95% CI = 56.9–58.1), whereas that in larger establishments was 14.4 claims per 100,000 workers (95% CI = 14.2–14.7). Both small and large establishments demonstrated significantly decreasing trends in the incidence rate (p < 0.001). However, the incidence rate in small establishments in 2013 showed a 49.1% decrease from a high in 2005 (80.4 per 100,000; 95% CI = 77.9–82.9), while the incidence rate in larger establishments showed a 24.1% decrease from a high in 2006 (17.2 per 100,000; 95% CI = 16.2–18.3) (Figure 4).
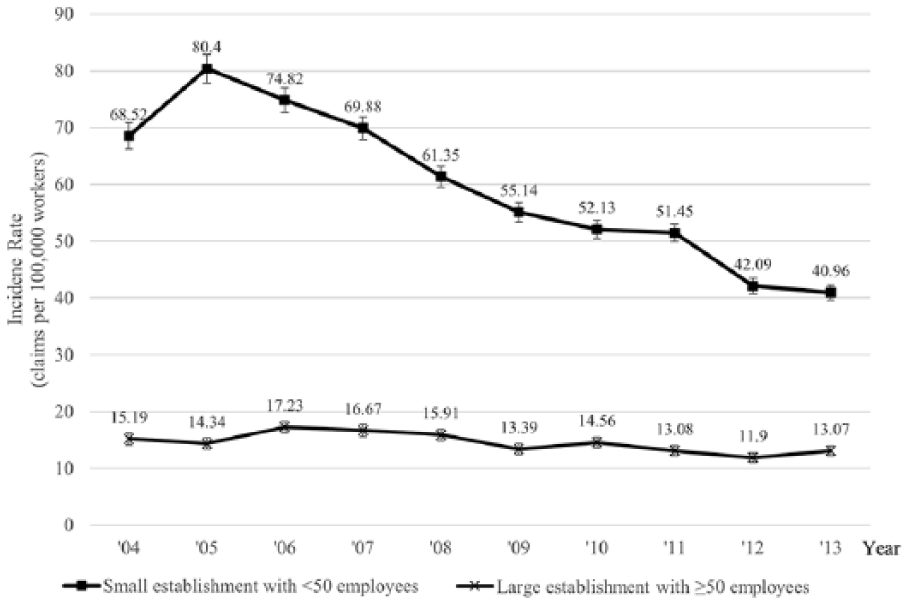
Trends in the incidence rate of work-related traumatic limb amputations according to establishment size in South Korea from 2004 to 2013.
Discussion
In this study, we observed that the incidence rate of work-related traumatic limb amputations was 38.8 claims per 100,000 workers from 2004 to 2013 in South Korea. The age–sex standardized incidence rate showed a 26.1% decrease from a high of 47.8 claims per 100,000 workers in 2006 to a low of 30.1 claims per 100,000 workers in 2013. The major workplace characteristics showing the highest incidence were manufacturing industry sector and small establishments with less than 50 employees. The most common anatomical site of amputation was the finger. The incidence rates of these amputations also showed significantly decreasing trends.
The incidence of work-related traumatic limb amputations in this study was higher than those in previous US studies undertaken in Michigan (13.6 cases per 100,000 workers in 2008, 14.4 cases per 100,000 workers in 1997),9,12 Washington (19.2 cases per 100,000 full-time workers between 1997 and 2005), 8 and in Kentucky (13.7 cases per 100,000 workers between 1994 and 2003). 11 The incidence of work-related traumatic upper limb amputations in this study was 37.3 claims per 100,000 workers, which is higher than rates reported in nationwide studies undertaken in Taiwan (12.5 cases per 100,000 workers) and Sweden (9 cases per 100,000 workers).2,13 These previous studies mentioned the possibility of underestimation due to recall bias in the questionnaire, limitation in source data analysis method, rejected claims of workers who were covered by alternative state or federal workers compensation, and a narrow survey population that does not include part-time employees.8,10,11,17 However, we analyzed nationwide workers’ compensation data including both full and part-time workers with not only diagnostic codes, but also detailed injury description data. These differences in methodologies may have minimized the risk of underestimation in this study.
The manufacturing industry and the size of small establishments are well-known risk factors for work-related traumatic amputations.14,18 In this study, the incidence rate for work-related traumatic amputations within the manufacturing industry (94.4 claims per 100,000 workers) was higher than that in other industries and also higher than that in previous reports (29–40 per 100,000 workers).9,10,12 This study also showed that the incidence rate of work-related traumatic amputations in small establishments with <50 employees (57.5 claims per 100,000 workers) was higher than that in larger establishments (14.4 claims per 100,000 workers). This difference in the incidence rate may be due to Korean legislation that specifies it is not compulsory for small establishments with <50 employees to hire safety managers. This finding was also consistent with a previous study that reported higher rates of work-related traumatic amputations in smaller establishments. 8
The incidence rate of traumatic finger amputation and traumatic amputation in the manufacturing industry and/or in a small establishment, as well as the overall age–sex standardized incidence rate, decreased significantly. The decreasing trend in the overall incidence rate is consistent with a previous Kentucky, US study, 11 and the decreasing trend in traumatic amputations within the manufacturing industry is consistent with reports from a previous study undertaken in Norway. 14 In that study, the declining trend was attributed to changes in worker compensation policies and legislative safety initiatives11,14 and the outsourcing of hazardous manufacturing processes to emerging economies, or being undertaken by immigrant workers. 14 In Korea, there were similar changes during the study period. Korea emerged as a high-income country in 2001, and this change was accompanied with the development of regulations regarding occupational safety. Regular inspection of press or lift machinery and the obligatory submission of a hazardous risk prevention plan that had been deregulated in 1997 were reintroduced. Laws protecting contingent workers were enacted between 2006 and 2007. 19 The manufacturing industry is being substituted by the service industry, and manufacturing factories have moved to emerging economies such as China and Vietnam.19,20 The proportion of insured workers within the manufacturing industry decreased from 28% in 2005 to 24% in 2013. The number of foreign workers also increased and, because of language barriers and limited fundamental labor rights, as well as their undocumented legal status, work-related injuries among foreign workers have been under-reported.14,21
This study is the first to conduct subgroup analysis of trends in the work-related traumatic amputation incidence rate, according to industry, establishment size, and affected body part. A novel finding of this study was that the incidence of traumatic amputations at the proximal upper and lower limb did not show a decreasing trend. Furthermore, the incidence rate in the construction industry, the second-most common industry involved in traumatic amputations, did not decrease. Benefits of changed legislative safety measures or the effect of outsourcing of hazardous processes appear not to have affected the incidence rate of proximal amputations or amputations within the construction industry. The cause of injury may be different between manufacturing and construction industries, 8 or between digital and proximal amputations above digit level. Therefore, further research is required to investigate the cause of injuries and to determine the reasons for these discrepancies.
Study limitations
Our study has some limitations. Self-employed workers and workers in special employment types, such as insurance salesmen, dispatch riders, and door-to-door salesmen, are not mandated to obtain workers’ compensation insurance. However, other workers in workplaces with ⩾ 1 employee are obligated to obtain insurance coverage after 2001. As of 2013, 97.5% of workers are registered for workers’ compensation insurance. 22 Therefore, the missed cases are unlikely to have had much impact on the conclusions drawn from the results.
Injuries for which <4 days off work are taken cannot be compensated and have not been included in this study. However, traumatic amputation is a major injury and usually requires ⩾4 days off work. Therefore, this limitation is not likely to have biased the results.
Furthermore, there is a risk of underreporting; amputations in foreign workers, in particular, may be hidden. The proportion of foreign workers in the Korean workforce is approximately 10% of all employees. Therefore, the underreporting by foreign workers may have a limited effect on the result of this study. Analysis of foreign workers would benefit from further research.
Despite these limitations, it was an aggregate, nationwide data of 10 years. Only 5.4% cases were excluded, and the inclusion criteria were based on medical diagnosis information and not reports from employers or employees.
Conclusion
To our knowledge, this is the largest study to date to report incidence rate trends in regard to work-related traumatic limb amputations, as well as the first study to analyze trends in the incidence rate according to workplace characteristics, such as industry and establishment size.
These findings may help further enhance preventive strategies in other emerging economies in Asia which are facing issues similar to those encountered in South Korea. Further research to identify the cause of traumatic amputations according to industry and establishment size is essential for developing preventive measures.
Footnotes
Author contribution
M.S.B., H.-I.S., J.-H.L., and I.J. contributed to conceptualization; M.S.B., H.-I.S., J.-H.L., I.J., J.-S.R., and Y.S.R. contributed to methodology; I.J., J.-S.R., and Y.S.R. conducted formal analysis; J.-H.L., I.J., S.H.L., and Y.S.R. performed data curation; I.J. prepared the original draft; M.S.B., H.-I.S., J.-H.L., I.J., and J.-S.R. reviewed and edited the manuscript; and all authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Research Center for Innovation in Medical Rehabilitation, which is funded by the Korea Workers’ Compensation and Welfare Service.