
Abstract
Background: Currently there is a paucity of research providing recommendations on the type of orthotic or material used in its construction for different patient requirements.
Objectives: To gain a greater understanding of the characteristics of orthotic materials and how they affect gait so to enhance the clinical decision-making process.
Study Design: Repeated measures.
Methods: Plantar pressures and kinematics were evaluated for 10 participants while walking on a treadmill under various conditions which included, shoes only and shoes with four different flat insoles and custom devices created in each of two densities of two materials.
Results: For the flat insoles, medium density ethyl vinyl acetate was found to produce greater peak pressures than at least one of the other material conditions and low and medium density polyurethane were most effective at increasing average contact area and at reducing pressure time integral. For the custom devices, while no significant differences were evident, when compared to the shoe only condition, medium density polyurethane increased average contact area by a greater percentage than the other materials.
Conclusions: Results for medium density polyurethane suggest a possible difference in loading characteristics, indicating a potential material suitability for patients with a compromised ability to deal with pressure.
Findings from the present study provide information for a clinician to draw an evidence-based orthotic prescription based on material properties.
Background
Orthoses are routinely prescribed to people with diabetes to offload pressure in areas of the foot that may cause ulceration. However, there is little scientific evidence on the use of custom foot orthoses in diabetes to improve gait and reduce further deformity. Systematic reviews that have examined the effectiveness of orthoses in preventing ulceration in people with diabetes1-4 have cautiously supported their use, with the authors considering the limited evidence from which they had made their conclusion. Subsequently these reviews have pointed out a major limitation of research in this area; although orthoses are shown to be of benefit in preventing ulceration, current research does not allow for recommendations regarding the type of orthoses to be prescribed. Furthermore, research to date does not provide a conclusive answer to what the most suitable materials to use in constructing orthoses for different patient requirements are. 5
In-shoe pressure measurements, namely peak pressure, peak force and pressure time integral 6 are the most common outcome measures used in research to determine the effectiveness of orthoses.7-10 The widespread use of in- shoe pressure measurements in research studies involving orthotic effectiveness is based on the established link between high foot pressure and ulceration which has previously been shown in an early retrospective study by Stokes et al. 11 and a more recent prospective study by Veves et al. 12 The cause of increased foot pressure in people with diabetes has received much discussion with potential contributors including neuropathy13,14 and limited joint mobility at the ankle and foot.15-17 Of the limited research available which used in-shoe plantar pressure measurements to compare orthoses materials some have focused on the effect of wear on the materials9,18,19 while others have compared the immediate effect of different orthoses materials on plantar pressures while walking.20,21 Both of these studies compared flat insoles with Birke et al. 20 comparing Poron® insoles of different hardness values and Tong and Ng 21 comparing two types of Poron® and two combinations of Poron® and Plastazote®. While this previous research examining Poron was warranted as it is a common prescription choice, other materials which are commonly prescribed, such as ethyl vinyl acetate and polyurethane, 22 have not been examined.
The comparison of plantar pressures when using flat versus custom orthoses have been conducted by a number of researchers.7,10,20,23-26 While direct comparison between these studies is not possible, due to the wide variety in both participants and interventions used, results from all but one of these studies 23 has supported the use of custom orthoses over flat. Only one of these studies 24 used the same material in the construction of both their flat insoles and custom devices, allowing identification of possible differences in the performance of the materials when used flat and when custom moulded to a participant’s foot. Previous research which has examined the effect of orthoses on lower limb kinematics has shown that changes in kinematics are evident when wearing orthoses compared to a shoe only condition. 27
With the range of material available for the manufacture of custom foot orthoses growing year on year, the aim of this study was to gain a greater understanding of the characteristics of the materials used and how they affect gait with a view to informing the clinical decision-making process in the provision of foot orthoses for people with diabetes. To extend the current knowledge and understanding in this area, it was hypothesized that insole material (ethyl vinyl acetate and polyurethane) and construction (flat and custom) would have an effect on lower limb kinematics and plantar pressures.
Methods
Participants
Ten healthy participants (four males and six females) with an average age of 30.9 (± 12.4) years, weight of 69.3 (± 12.2) kg and height of 172.0 (± 9.4) cm were recruited for the study. While the authors acknowledge the limitations associated with using a small sample size, previous research has reported that sufficient statistical power can be achieved when using a sample size of 10. 28 While the authors acknowledge that differences in gait are evident between gender, the focus of this study was on comparing the orthotic materials and not the participants and therefore we do not consider gender to be an issue in this manuscript.
Ethical approval was received from the university ethics committee and all participants signed the approved consent form before participating in the tests. All participants were free from any musculoskeletal injury at the time of testing and had no known history of foot pathologies or structural abnormalities.
Procedure
This laboratory-based study compared the effects of material choice (used in the manufacture of orthoses) on lower limb kinematics and plantar pressures. Materials chosen to be tested were: low density polyurethane (PU) (Shore A hardness 20–25), medium density PU (Shore A hardness 55 ± 3), low density ethyl vinyl acetate (EVA) (Shore A hardness 25) and medium density EVA (Shore A hardness 50). The materials used were selected based on a previous survey, which found that these are the materials used within orthoses that are commonly prescribed to people with diabetes. 22
The study consisted of two testing sessions with the first requiring participants to walk on a treadmill while wearing standardised plimsoll shoes (a minimalistic athletic shoe with a canvas upper and rubber sole) under five conditions: (1) shoe only, and shoe with; (2) 3-mm flat insole of low density PU; (3) 3-mm flat insole of medium density PU; (4) 3-mm flat insole of low density EVA; and (5) 3-mm flat insole of medium density EVA. As the focus of this study was on comparing the orthotic materials we chose this ‘minimalistic’ footwear as we wanted to limit the effect of the footwear on gait. Following this baseline assessment, participants had foam box impressions of their feet taken by the same experienced clinician. These impressions were used to create custom devices for each participant in each of the two densities (low and medium) of the two materials (PU and EVA) for the second testing session. These devices were created using CAD/CAM technology with a standard mode of manufacture. A standard prescription form (Salts Techstep, UK) was used with a 4° medial extrinsic rearfoot posting and forefoot balanced to rearfoot vertical on a shell customised to the participant. This type of prescription is common and traditional within the podiatric profession across various countries (modified Root prescription technique). No attempt was made to evaluate the participants using clinical biomechanical paradigms as it was the function of the device, not the participant, that was of interest. A 4° rearfoot posting was used as this was thought to be a very common prescription characteristic across various common orthotic interventions. Prescribed devices were full length with 3 mm thickness under the forefoot, toes and heel, and a top cover of 1-mm medium density EVA.
The testing procedure for the first session was replicated with the five conditions for this second session being: (1) shoe only, and shoe with; (2) custom device of low density PU; (3) custom device of medium density PU; (4) custom device of low density EVA; and (5) custom device of medium density EVA. The order of testing condition for both sessions for each participant was randomly determined using a computer-generated random number list (MS Excel 2007, Microsoft, USA). Forty-two reflective spherical markers (14 mm diameter) were placed on anatomical landmarks on the participant, using double-sided tape on their bases, for use with the Plug-in-Gait and Oxford Foot Models. 29 The shoes used in the present study were modified to allow the reflective markers to be placed on the participants’ feet. Shoe modification involved removing sections of the shoes canvas upper to allow the placement of markers on anatomical landmarks. A minimum amount of material was removed to allow the placement and unobstructed movement of markers during gait while aiming to maintain the structural stability of the shoe. As the reflective markers which were placed on the feet had to be removed and reapplied when footwear conditions were changed, markings were made on the skin where the markers were to be placed to aid correct reapplication. An eight-camera motion analysis system (Vicon, OMG, Oxford, UK) was used to record the motion of the individual markers and in-shoe pressures sensors (F-Scan, Tekscan, Boston, USA) with a resolution of 3.9 sensels per cm2 measured plantar pressure distribution. The F-Scan sensors were trimmed to fit the plimsoll shoes and one pair of sensors was used per shoe size.
Prior to data collection, calibration of equipment was conducted according to manufacturer’s guidelines. For the motion analysis system a dynamic calibration was performed and residuals of less than 2 mm from each camera were deemed acceptable. A static standing trial was recorded for each condition and was used to estimate joint centres and other virtual points from the marker locations. Data were collected while the participants walked on the treadmill at a self-selected speed (3.4 ± 0.5 km/h−1). Eight trials of 10 s duration were recorded for each condition. Both motion analysis and in-shoe pressure system employed a sampling frequency of 100 Hz and were synchronised for data collection using a custom-made synchronization box (Tekscan Inc., USA). The heel contact and toe off events during a gait cycle were identified using in-shoe pressure sensors and applied to the motion analysis trials.
Data processing and analysis
Plantar pressure analysis was conducted by dividing the contact area of the foot into six anatomically and functionally relevant regions which are shown in Figure 1. The six regions were hallux, first metatarsal, lateral metatarsals, midfoot, medial heel and lateral heel. Stance duration, peak pressure, peak force, pressure time integral and average contact area for each of the six regions was recorded using the proprietary software (F-Scan Research 6.51, Tekscan Boston, USA). Three-dimensional marker data were filtered with a Woltring filter (MSE=20) which is the method recommended by the manufacturer for optimum results. For lower limb kinematics the range of motion of the following were recorded; femur/tibia flexion, adduction and rotation, forefoot/hindfoot dorsiflexion, adduction and supination, hindfoot/tibia dorsiflexion and inversion and hallux/forefoot dorsiflexion. Additionally the change in angle of these variables (except hallux/forefoot dorsiflexion) early in the loading response 30 (from heel strike to 6% of the gait cycle) was calculated. The first three trials collected for each condition which were deemed acceptable based on the correct data acquisition of both the Vicon and F-Scan systems were used for analysis. Eight trials were collected for each condition to ensure that sufficient data were collected in case of data corruption of trials. The three trials, with six to eight steps per trial (with the first and last steps removed from the analysis), were analyzed and results for these three trials were then averaged to create a representative trial. For statistical analysis a repeated measures ANOVA (p ≤ 0.05) was used to access differences between conditions. Post hoc pair-wise comparisons with Bonferroni adjustments were conducted for multiple comparisons.
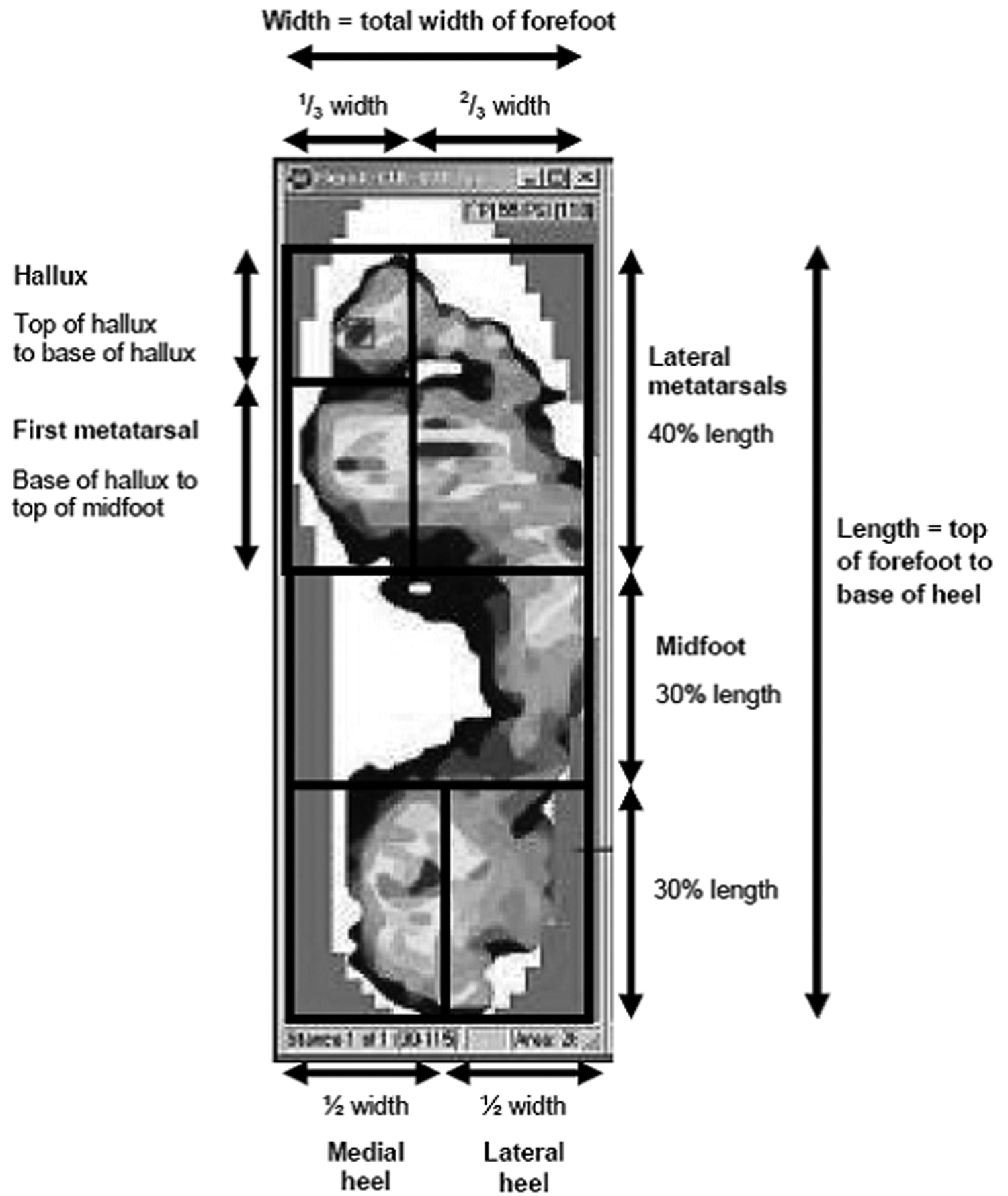
Definition for division of foot into six sections.
Results
First session – flat material
Mean values for stance duration and F-Scan in-shoe measurements are provided in Table 1 with lower limb kinematic data presented in Table 2. The stance phase duration was significantly less for medium density EVA than low density EVA (0.70 ± 0.03 s vs. 0.71 ± 0.03 s). The shoe only condition produced significantly greater peak pressures than the other conditions at the first and lateral metatarsal regions only. The addition of medium density PU resulted in reduced peak pressure at the first metatarsal region, and all conditions except medium density EVA, resulted in reduced peak pressure at the lateral metatarsal region. Where significant differences were evident between the conditions, medium density EVA always produced greater peak pressures than at least one of the other material conditions. Where significant differences were evident for peak force, medium density EVA was found to produce greater peak forces at the lateral metatarsal region than all the other materials and more than low density EVA and PU at the medial heel. In general, the low and medium density PU were the most effective at increasing average contact area and at reducing pressure time integral. Significant differences for range of motion were evident for femur/tibia adduction with low density EVA significantly greater than medium density EVA and forefoot/hindfoot supination with the shoe only condition significantly less than medium density EVA. When going from heel strike to 6% of the gait cycle the change in angle for femur/tibia flexion was significantly greater for medium density EVA than the shoe only condition.
Comparison of F-Scan in-shoe pressure measurements between conditions for flat material session (mean ± standard deviation).
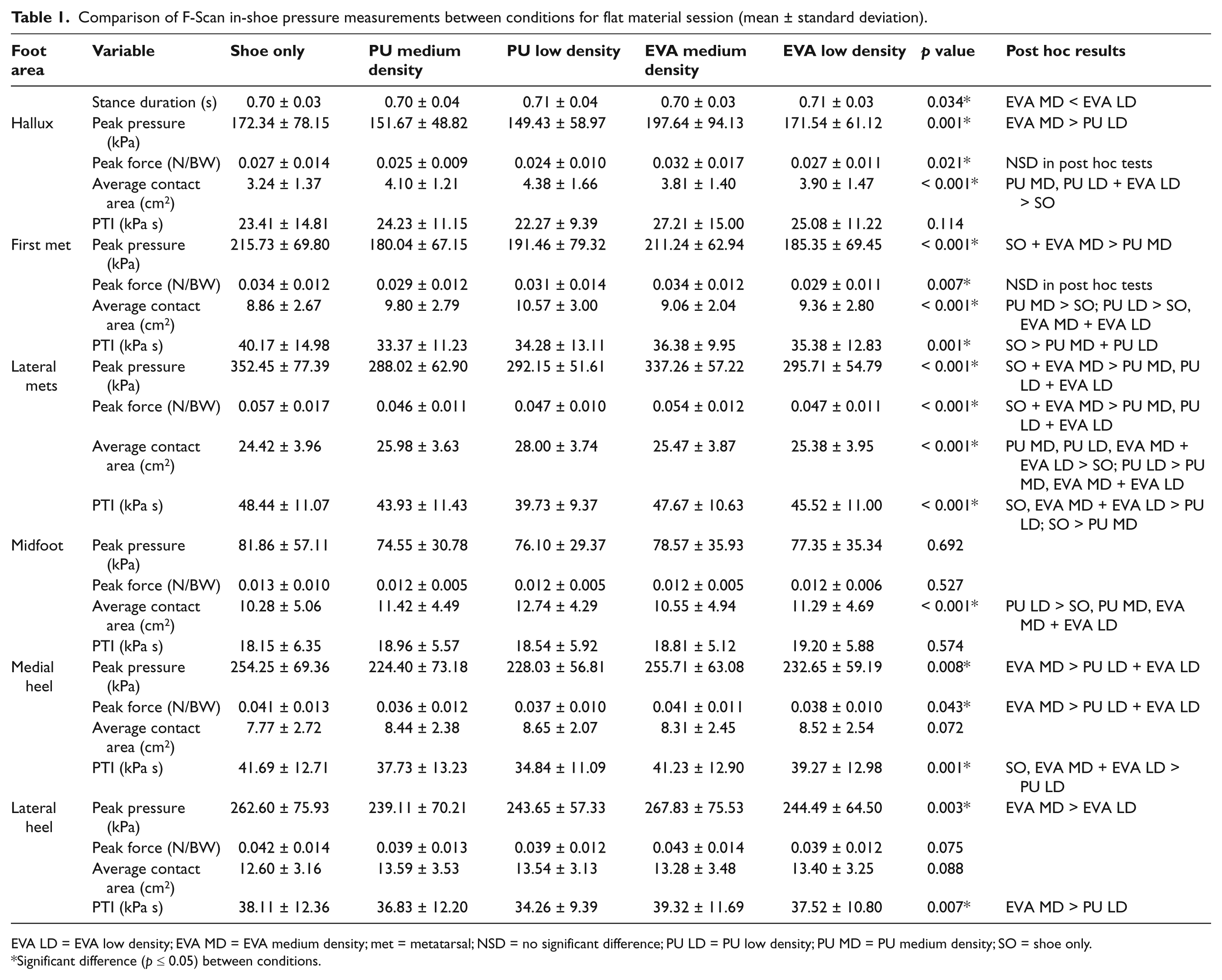
EVA LD = EVA low density; EVA MD = EVA medium density; met = metatarsal; NSD = no significant difference; PU LD = PU low density; PU MD = PU medium density; SO = shoe only.
Significant difference (p ≤ 0.05) between conditions.
Comparison of kinematic variables between conditions for flat material session (mean ± standard deviation).
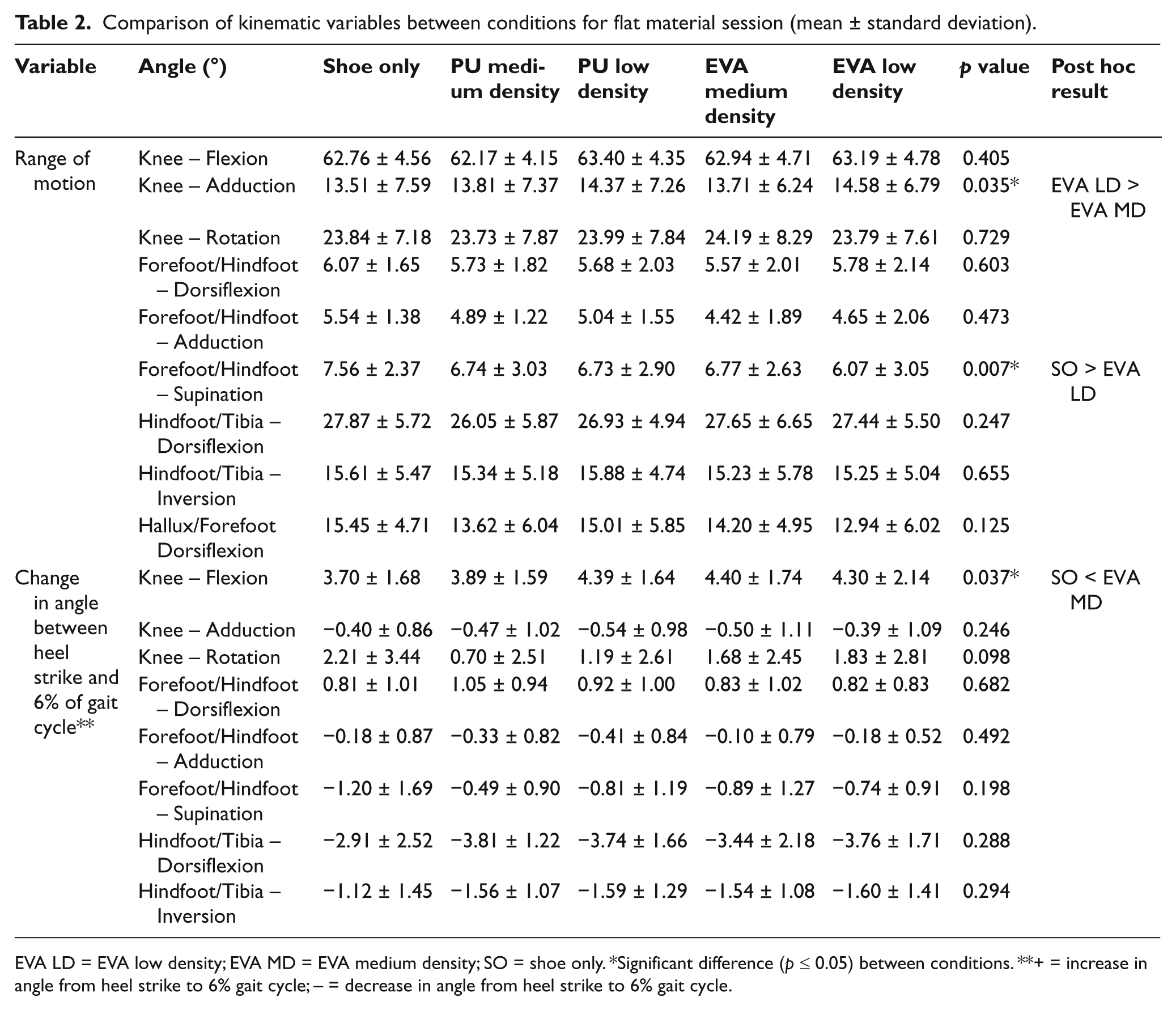
EVA LD = EVA low density; EVA MD = EVA medium density; SO = shoe only. *Significant difference (p ≤ 0.05) between conditions. **+ = increase in angle from heel strike to 6% gait cycle; – = decrease in angle from heel strike to 6% gait cycle.
Second session – custom device
Mean values for stance duration and F-Scan in-shoe measurements are provided in Table 3 with lower limb kinematic data presented in Table 4. Medium density EVA and PU were found to significantly increase peak pressure at the hallux when compared to the shoe only condition. Both low density materials (PU and EVA) were found to significantly reduce peak pressure at the first and lateral metatarsals when compared to the shoe only condition. All the materials were effective at significantly reducing peak pressure at the medial and lateral heel when compared to the shoe only condition. Medium density PU and EVA increased peak force at the hallux and midfoot when compared to the shoe only condition. All the materials were effective at significantly reducing peak force at the medial and lateral heel. When compared to the shoe only condition, contact area was significantly increased by all materials at the hallux and midfoot. All materials reduced pressure time integral at the lateral metatarsals and the medial and lateral heel. Significant differences for range of motion were evident for forefoot/hindfoot supination with the shoe only condition significantly greater than both PU conditions. When going from heel strike to 6% of the gait cycle the change in angle for femur/tibia flexion was significantly greater for low density PU than low density EVA.
Comparison of F-Scan in shoe pressure measurements between conditions for custom device session (mean ± standard deviation).
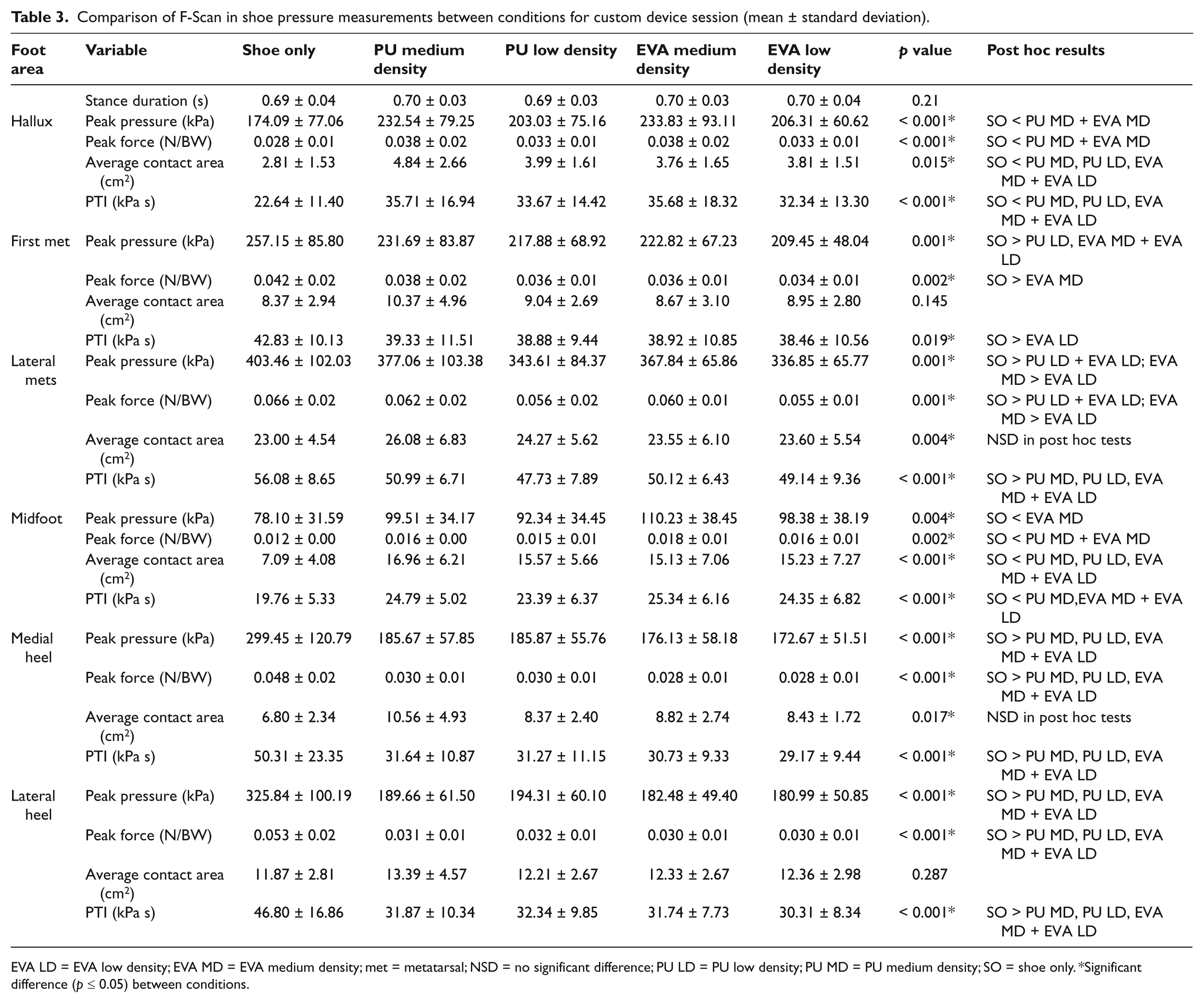
EVA LD = EVA low density; EVA MD = EVA medium density; met = metatarsal; NSD = no significant difference; PU LD = PU low density; PU MD = PU medium density; SO = shoe only. *Significant difference (p ≤ 0.05) between conditions.
Comparison of kinematic variables between conditions for custom device session (mean ± standard deviation).
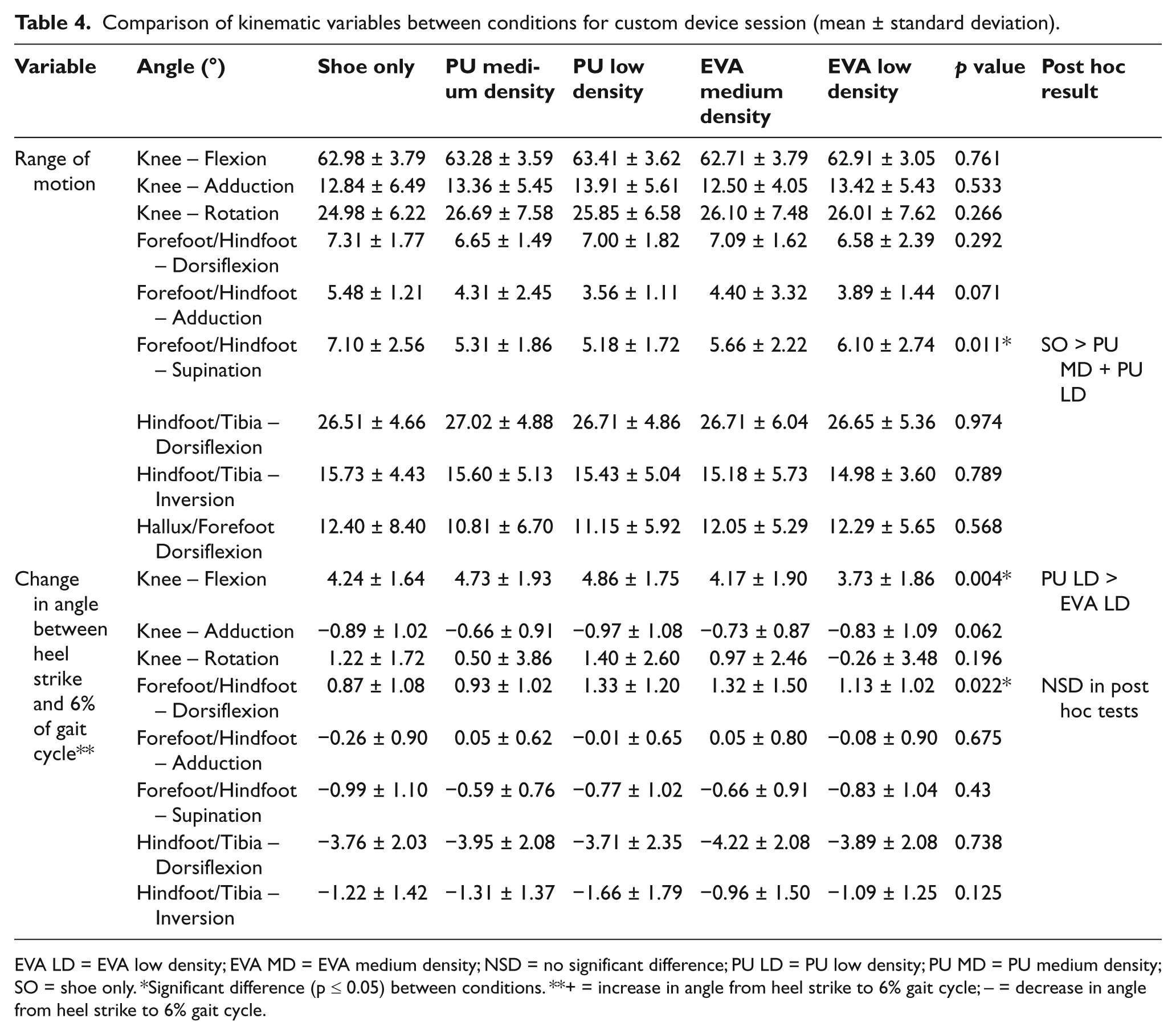
EVA LD = EVA low density; EVA MD = EVA medium density; NSD = no significant difference; PU LD = PU low density; PU MD = PU medium density; SO = shoe only. *Significant difference (p ≤ 0.05) between conditions. **+ = increase in angle from heel strike to 6% gait cycle; – = decrease in angle from heel strike to 6% gait cycle.
Discussion
As hypothesized, various insole materials and different construction were found to have an effect on plantar pressure, however, in contrast to our hypothesis, there was little effect on lower limb kinematics.
Kinematics
Lower limb kinematics were assessed to examine the effect of the materials on ankle and foot joint mobility. Few significant differences were evident between conditions. Since these differences were small (0.7°–1.49°), they were not considered relevant. 31 Similarly, for the custom devices, some small differences (1.13°–1.92°) in lower limb kinematics were evident between conditions. These small differences may be attributed to extrinsic factors such as marker placement procedures and related skin movement and intrinsic factors such as variability in functional anatomy between the participants. These factors might have had an influence in the changes in actual joint angles and may not contribute to significant modifications in clinical intervention.
Plantar pressure
Results for the flat insoles showed that medium density EVA always produced greater peak pressures than at least one of the other material conditions and that both PU insoles were most effective at increasing contact area and reducing pressure time integral, indicating the possibility that PU is superior to EVA when pressure reduction is a requirement. When the percentage change in peak pressure of the custom devices were compared to the shoe only condition, findings were similar to previous research 24 whose custom devices were also found to increase peak pressure at the hallux. While it is difficult to identify specific reasons for this increase, the changes could be attributed to the relationship between the participants’ plantar surface contour and the construction of the custom devices.
While no significant differences were evident between the materials for average contact area further analysis showed that when compared to the shoe only condition medium density PU increased the average contact area by a greater percentage than the three other materials in all six areas of the foot; hallux (30–38% greater), first metatarsal (16–20%), lateral metatarsals (8–11%), midfoot (20–26%), lateral heel (9–10%) and medial heel (26–32%). This suggests a possible difference in the loading characteristics of the material with medium density PU appearing to conform more with pressure therefore spreading the load over a greater area. This does not affect other measurements such as peak pressure in the zone, but does indicate a contouring around the anatomical structure that is applying the pressure such as the first metatarsal head or the hallux. This could have a clinical significance in the ability of the material to ‘off load’ areas of the foot by distributing the force over a greater area and therefore changing the shape of the point of contact. Clinicians may consider this useful when choosing a material that needs to be supportive, corrective and have good pressure attenuation characteristics for patients with compromised ability to deal with pressure.
Additionally, while the average contact area for the medial and lateral heel in the custom devices was not significantly different to the shoe only condition, the F-Scan sensors were cut to fit the shoe without the devices and therefore the sensors did not cover all of the heel contour on the custom devices and subsequently could not measure the entire contact area of the heel contour.
The effect of the manufacturing process on the production of custom devices also needs to be considered, manufacturing techniques may cause material deformation which may influence the material performance characteristics. 32
Flat insoles versus custom devices
As significant differences were evident when the results for the shoe only condition from both the flat insoles and custom device sessions were tested, subsequent comparisons between the two sessions were not completed.
While the present study examined the effect on plantar pressure and joint mobility of different materials used in orthoses prescribed for people with diabetes, normal population participants were recruited as research to date has not examined orthotic materials in this way before with this study providing baseline data on the performance of the tested materials for the normal population.
Conclusion
Results for the flat insoles suggest the use of PU for patients where a reduction in peak pressures is required. With regard to the custom devices, the results for average contact area for medium density PU suggest a possible difference in the loading characteristics of the material, indicating that it may be a suitable material for patients with a compromised ability to deal with pressure.
Footnotes
Funding
This work was supported by Salts Techstep under sKTP project (No: sKTP012).