
Abstract
Background and Aim: Ankle joint stiffness and its range of motion (ROM) are commonly assessed to determine the appropriate mechanical characteristics required in an effective ankle-foot orthosis (AFO) prescription. The aim of this technical note is to present the design of a manual device that enables their convenient measurement in the clinical setting and to demonstrate its reliability.
Technique: The manual device was designed with a torquemeter, a potentiometer, a steering wheel, a rotary plate, and a foot plate. The measurement of resistive torque at 0° (neutral), 5° (dorsiflexion) and 10° (dorsiflexion) ankle angular positions demonstrated the high reliability of the device with Intraclass Correlation Coefficient (ICC) (1,k) values over 0.97.
Discussion: Quantitative measurement of ankle joint stiffness and ROM by this manual device would provide objective information that could potentially assist AFO prescriptions. A future study should investigate how to incorporate the measurement obtained from the device into the prescription of an AFO.
Clinical relevance
The manual ankle joint assessment device enables an orthotist to assess ankle joint stiffness and ROM quantitatively and reliably in a clinical setting. The device could potentially assist AFO prescriptions when utilized in further studies.
Introduction
The amount of passive ankle joint stiffness and ankle range of motion (ROM) in subjects with various pathologies are commonly evaluated manually in the clinical setting. Previous methodologies have involved the use of various devices in evaluating ankle stiffness and ROM.1-3 Assessment of these parameters is particularly important for orthotists to enable them to determine the mechanical properties required in an ankle-foot orthosis (AFO) design. The mechanical characteristics of AFOs and the physiological characteristics of an anatomical ankle joint need to be matched to maximize the benefit from an orthotic intervention. 4
A specific AFO prescription must be based on the physical condition of each individual patient. A patient with a spastic ankle joint may require an AFO to prevent foot-drop, 4 whilst a patient with ankle instability may need it for better stability. 5 The stiffness of an AFO critically influences ankle joint kinematics, 6 and therefore ankle joint stiffness and ROM are usually considered when formulating an AFO prescription. However, this process relies on the knowledge and skills of an orthotist. Therefore, a clinical tool that could reliably and conveniently quantify these parameters would be useful throughout treatment regimes.
A manual device was developed for use in our previous studies to demonstrate its potential capability to evaluate spastic ankle joint stiffness.7-8 The specific aim of this technical note is to present an improved design of the manual device and to demonstrate its reliability.
Methods
Design of the device
The device was constructed with a torquemeter (TCF-50N, Nippon Tokushu Sokki, Tokyo, Japan), potentiometer (HSM30F, Sakae, Kawasaki, Japan), steering wheel, rotary plate and foot plate (Figure 1). A power supply (E-3515, Mitsuwa Denshiki Seisakusho, Kyoto, Japan) was used to supply DC +5V to the potentiometer and DC ±15V to the amplifier unit (HSC-20B, Kyowa, Tokyo, Japan) that subsequently supplied power to the torquemeter. The output signal from the torquemeter and the potentiometer was then fed into a computer through an analogue-to-digital (A/D) convertor (ADA16-8/2(CB)L, Contec, Osaka, Japan).
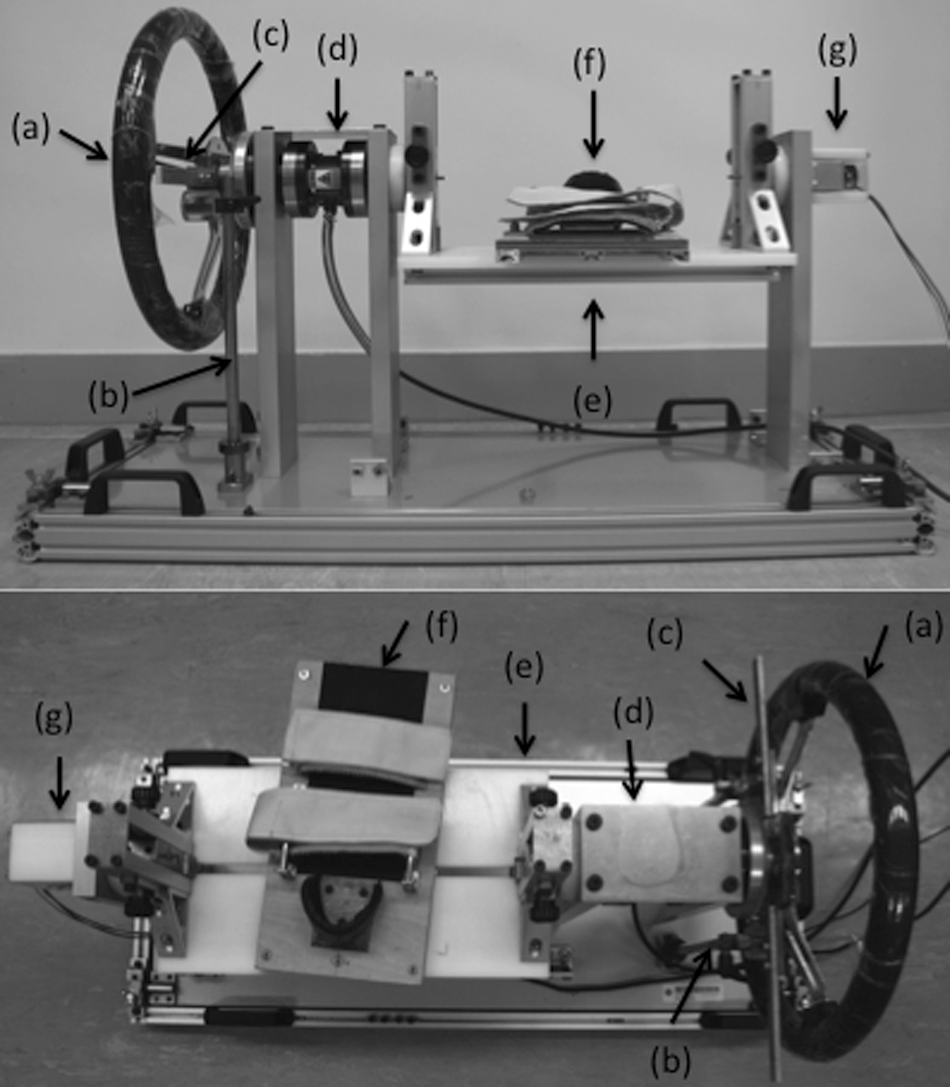
A manual ankle joint assessment device: (a) steering wheel; (b) mechanical stopper; (c) bar; (d) torquemeter; (e) rotary plate; (f) foot plate; (g) potentiometer.
The device facilitated the measurement of the angular positions and their corresponding torques simultaneously around an ankle joint in the sagittal plane by applying a manual force to the steering wheel linked to the rotary plate. The ROM of the foot plate in plantarflexion and dorsiflexion directions was adjustable with mechanical stoppers positioned under the bar attached to the steering wheel. The following improvements were made to our previous device design:7-8 (1) the foot plate was redesigned to move freely on the rotary plate with an ankle-foot complex fixed to it, which allowed more convenient and accurate positioning of the axis of the rotary plate to the estimated rotational centre of the ankle joint (Figure 1); (2) The location of the ankle strap was redesigned to be more adjustable so that it could tighten around the position immediately distal to the ankle joint to minimize the constriction of its movement (Figure 1); (3) A protractor was placed around the axis of the steering wheel, which enabled testing of ROM without a power supply (Figure 2); and (4) the device was redesigned so that it could also measure stiffness of an AFO/footwear combination whilst donned upon the patient (Figure 3). The foot plate was also redesigned for this purpose.

A protractor fixed around the axis of the steering wheel.

Measurement of stiffness of an AFO/footwear combination whilst donned upon a subject.
Calibration
Calibration of the torquemeter was conducted by applying an increasing series of known moments (0 to ±30 Nm at every 2 Nm) at 0° position using a beam and a weight, whilst that of the potentiometer was performed with an increasing series of known angles (0 to ±55° at every 5°) using a digital protractor (950-317, Mitsutoyo, Kanagawa, Japan). The torquemeter and potentiometer showed excellent linearity of R2=1.00 and R2=0.99, respectively.
Reliability testing
Ten male subjects with hemiplegia (age 54.3 (8.4) years) who suffered from a stroke for more than three years (8.7 (4.5) years) participated in this study. They were instructed to sit on a height-adjustable seat with the hip and knee joints in 90° of flexion. The ankle-foot complex of the affected side was fixed onto the foot plate. The rotational axis of the foot plate was placed at the apex of the lateral malleolus of the ankle joint. The ankle joint was subsequently rotated slowly during the assessment. The measurement was conducted three times for each subject by the same examiner, with compensation for the influence of gravity. 7 The study was approved by the Human Subjects Ethics Committee of The Hong Kong Polytechnic University, and consent was obtained from each subject.
The reliability of the measured torque at 0° (neutral), 5° (dorsiflexion) and 10° (dorsiflexion) ankle angular positions was tested by evaluating ICC (1,1) and ICC (1,3). 9 These ankle angular positions were selected as a general range of initial angles of an AFO. It has been reported that, in patients with stroke, an AFO with a dorsiflexed angle at heel strike during gait has a more positive effect on heel loading and knee stability than an AFO in plantarflexion. 10 The results of this study demonstrated high reliability of the device with ICC (1,k) values over 0.97 (Table 1).
ICC (1,1) and ICC (1,3) of the measured ankle joint resistive torque at 0° (neutral), 5° (dorsiflexion) and 10° (dorsiflexion) ankle angular positions.
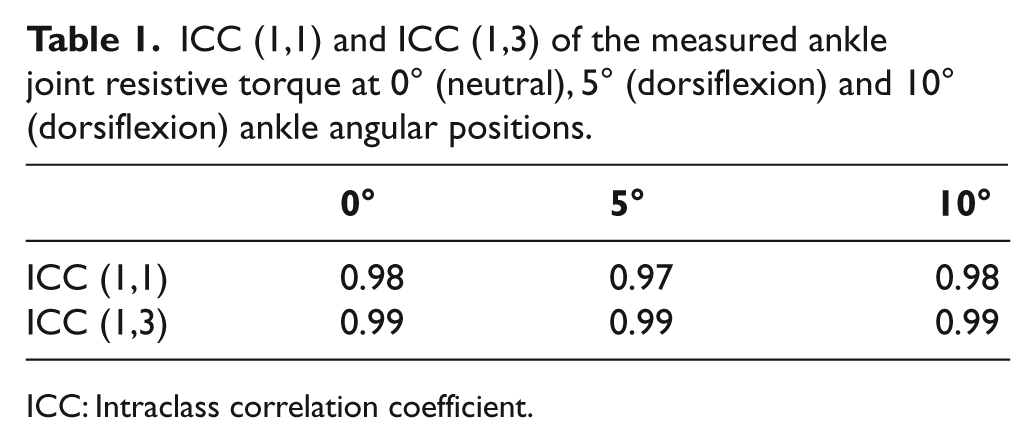
ICC: Intraclass correlation coefficient.
Discussion
Assessment of ankle joint stiffness and ROM is usually conducted subjectively based on the experience of an orthotist to determine the mechanical properties of an AFO to be prescribed. The manual ankle joint assessment device demonstrated a high reliability and would enable more objective assessment of an ankle joint.
This device would also allow the testing of a subject with an AFO in situ to quantify the stiffness of the AFO/footwear combination 11 or by directly fixing an AFO to the device using external supporting frames, a surrogate limb or C-clamps. 12 The deformation of an AFO would depend on (1) the thickness and design of the structure, (2) the elastic modulus of the material, (3) the fit and firmness of the limb within, and (4) the constraining characteristics of the shoe. These factors would also affect the motion resistance characteristics of an articulated AFO by altering the degree of co-alignment of medial and lateral joint components. Therefore, a device that can measure stiffness of an AFO/footwear combination whilst donned upon the patient in the clinical setting could be useful. 13 A manual device enables ROM and applied torque to be controlled conveniently and cautiously to prevent mechanical failure or fracture of an AFO. This is particularly relevant when testing non-articulated AFOs where sagittal plane ROM is difficult to predict. Moreover, a manual device would be more practical in the clinical setting. 8
The stiffness of an AFO should be adjusted to maintain ankle angular position to prevent foot-drop during swing phase, and should ideally also be tuned to allow smooth transitions between phases of gait and smooth forward progression during stance phase. 13 Therefore, the ROM demonstrated by an AFO/footwear combination should be designed accordingly to maximize the three rockers of gait during stance phase. 14 Sagittal plane ROM would be determined mainly by stiffness in non-articulated AFOs, and by stiffness and/or physical means (i.e. stoppers or limiters) in articulated AFOs.
This device was designed to measure stiffness in the sagittal plane as ankle movement in gait occurs mainly in this plane. Thus most researchers have focused on the sagittal plane. 13 Since gait also produces multiple-axis loads on the ankle-foot complex, the AFO/footwear combination would be subjected to moments acting in three planes, which could result in cross-coupled deformation effects. 15 Therefore, a cross-coupled moment applied in the transverse or frontal plane due to the asymmetry of ankle contour trimlines or the goodness of AFO fit to the limb would be the cause of measurement errors.
The limitations of the study were as follows: (1) a small number of subjects (n=10) was recruited for this study; (2) only one examiner participated in the reliability test. Therefore, a further study is desired for more robust reliability results [i.e. ICC (2,k) or ICC (3,k)] by recruiting a higher number of subjects and examiners. 9
Conclusion
The manual ankle joint assessment device would enable an orthotist to assess ankle joint stiffness and ROM quantitatively in a clinical setting. A further study should investigate the accuracy and repeatability of the device to measure the stiffness of an AFO/footwear combination12,13 and explore its potential capability to assist AFO prescriptions.
Footnotes
Funding
This work was funded by The Hong Kong Polytechnic University International Postgraduate Scholarships for PhD Studies.
Conflict of interest
The authors declare that there is no conflict of interest.