
Abstract
Background:
The aim of this case study was to verify the efficacy and safety of anti-gravity treadmill training for prosthetic rehabilitation following below-knee amputation.
Case description and methods:
The patient underwent left below-knee amputation as a result of diabetic foot gangrene. Since his physical strength and vitality had declined during the perioperative period, anti-gravity treadmill training was introduced for his outpatient prosthetic rehabilitation.
Findings and outcomes:
Stable prosthetic gait exercise could be carried out under guidance on the anti-gravity treadmill, quickly resulting in improved gait. Furthermore, the patient’s self-efficacy and exercise tolerance were elevated after the period of anti-gravity treadmill training. At the final evaluation following 6 weeks of rehabilitation with the anti-gravity treadmill, he had acquired prosthetic gait with the assistance of a T-cane.
Conclusion:
The anti-gravity treadmill was found to be a useful instrument for prosthetic rehabilitation following below-knee amputation.
Clinical relevance
Anti-gravity treadmill training has the potential to support the prosthetic rehabilitation of below-knee amputees, especially for patients whose physical strength and vitality are decreased.
Background
Recently, the main causes of amputation of the lower limbs have changed from traffic accidents and tumors to peripheral arterial disease, and the incidence of lower extremity amputation has increased. 1 Most patients with peripheral arterial disease have difficulties in walking and do not have the habit of taking regular exercise because of symptoms including pain and paralysis. 2 Therefore, the physical strength and vitality of patients tend to decrease during the perioperative period, and most patients cannot participate positively in prosthetic rehabilitation; it is therefore difficult for them to attain appropriate prosthetic gait.
The anti-gravity treadmill, consisting of a treadmill enclosed within an airtight chamber, applies air pressure to a patient’s lower body to alter body weight support and can decrease the load on lower extremities and cardiovascular function. 3 Furthermore, on the current commercially available anti-gravity treadmill (AlterG™, Fremont, CA, USA), the risk of falling is negligible because in addition to the presence of a handgrip, patients wear shorts specially designed for the treadmill which are attached to the treadmill air chamber. Therefore, our hypothesis was that the anti-gravity treadmill could be a useful instrument for prosthetic rehabilitation of below-knee amputees, especially for those patients with reduced physical strength and vitality. However, so far, there have been no reported investigations of the efficacy of anti-gravity treadmills for prosthetic rehabilitation.
The purpose of this case study was therefore to verify the safety and effectiveness of anti-gravity treadmill training for prosthetic rehabilitation of a below-knee amputee.
Case description and methods
A 66-year-old male subject (weight = 81 kg, height = 168 cm) underwent left below-knee amputation because of diabetic foot gangrene. Following amputation, necrosis of the stump of the left lower leg occurred and additional debridement of the stump was performed. Treatment of the wound and servicing of the removable rigid dressing were started the day following the debridement. However, it took 5 weeks for the wound to heal and to attach the lower extremity pressure-cast prosthesis (ICECAST Anatomy; Össur, Reykjavik, Iceland). 4 Although resistance muscular strength training and endurance training were continued in the interim, his physical strength and vitality decreased. After attaching the lower extremity prosthesis, standing-position training, balance training, and walk training with a parallel bar were performed, but the patient could not acquire the necessary prosthetic gait ability because he was exhausted by the rehabilitation and required crutches and assistance in walking at the time of discharge. Since his decreased physical strength and vitality were considered to be inhibitors of his gait exercise, anti-gravity treadmill training was introduced for his outpatient prosthetic rehabilitation.
The outpatient rehabilitation was conducted for 20–40 min three times a week, beginning with stretch exercises followed by the anti-gravity treadmill (AlterG M320; AlterG™) training (Figure 1). Regarding the treadmill setting, body weight support, walking speed, and exercise time were adjusted with the ratings of perceived exertion using Borg’s scale of 10–13 points for walking and cardiopulmonary effort. Borg’s 5 scale is an index to measure the rating of perceived exertion: 10 points indicates “fairly light” and 13 points indicates “somewhat hard.” The incline of the treadmill was not changed. During anti-gravity treadmill training, guidance in the correct prosthetic gait was also carried out. After treadmill training, resistance muscle strengthening exercises (especially for the diseased limb) and free walk training on the floor were briefly performed. During the study period, body weight support, treadmill speed, and exercise time on the treadmill were adjusted according to the Borg ratings of perceived exertion.

Patient training on the anti-gravity treadmill.
The General Self-Efficacy Scale was used to assess optimistic self-efficacy to cope with a variety of difficult demands at each important step in the study period. 6
At 1 week (initial examination) and 6 weeks after (final examination) the introduction of treadmill training, the performance of walking on the floor including a 6-min walking distance was evaluated.
At the initial and final examination of the study, pulmonary gas exchange was also measured breath-by-breath with a mobile aero monitor (AE-100i; MINATO Medical Science, Tokyo, Japan) during the anti-gravity treadmill training at 40% of body weight support and a speed of 1.25 m/s for 8 min. The oxygen consumption rate (VO2) was recorded throughout the tests.
Ethical consideration and informed consent
The subject and his wife were informed about the parameters of the study and consented to a series of investigations. A signed statement of consent was obtained from the couple for permission to use the photographs and laboratory data. The Hiroshima University Ethics Committee suggested to obtain a signed statement of consent for a case study.
Findings and outcomes
During the study period, no falling occurred, there were no apparent problems with using the lower extremity prosthesis, and the prosthetic gait exercises were accomplished stably and successfully.
The General Self-Efficacy Scale was 27 before the first operation and 26 at discharge, where it remained until the introduction of the anti-gravity treadmill training. However, it rose to 33 just after the introduction of anti-gravity treadmill training and remained at 33 through to the final evaluation.
Table 1 shows the progress of the anti-gravity treadmill training. At the beginning, the patient exercised with 30%–40% of body weight support and at a speed of 0.56–0.83 m/s for 10 min. However, at the final evaluation, he could exercise with only 0%–15% of body weight support and at a speed of 0.97–1.11 m/s for 30–40 min.
Exercise intensity on the anti-gravity treadmill.
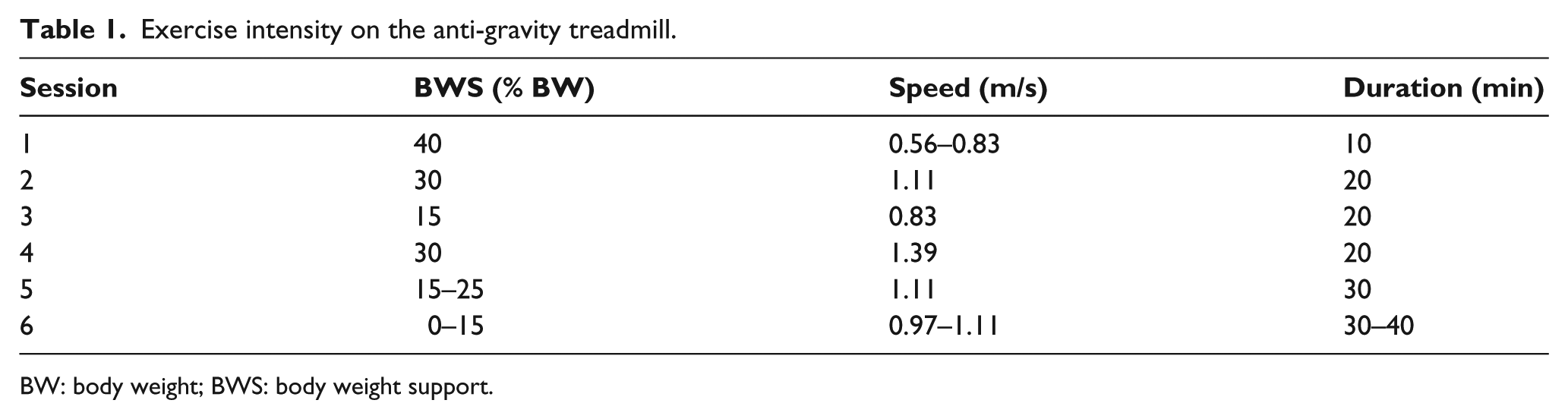
BW: body weight; BWS: body weight support.
Before the introduction of the anti-gravity treadmill training, he required crutches and assistance when walking. However, at the final evaluation, he had fully acquired the ability for prosthetic gait with the aid of a T-cane and no longer required assistance (Figure 2). At the initial examination of the study, the 6-min walking distance with crutches and assistance was 230 m (mean velocity 0.64 m/s). However, at the final evaluation of the study, the walking distance with a T-cane was 331 m (mean velocity of 0.92 m/s). The points on Borg’s scale after the 6-min walking at the initial examination were 13: the same as at the final examination, although the walking distance at the final examination was longer than that at the initial evaluation.

Gait 1 week (initial) and 6 weeks (final) after introduction to anti-gravity treadmill training: (a) initial—the patient tried to walk with crutches but gait was unstable and he required the assistance of his wife; and (b) final—gait was stable and the patient could walk with a T-cane without assistance.
The oxygen consumption rate reached a plateau about 3 min after the start of the anti-gravity treadmill training. After reaching this plateau, the VO2 at the final evaluation was lower than that at the initial examination for the same treadmill conditions (Figure 3).
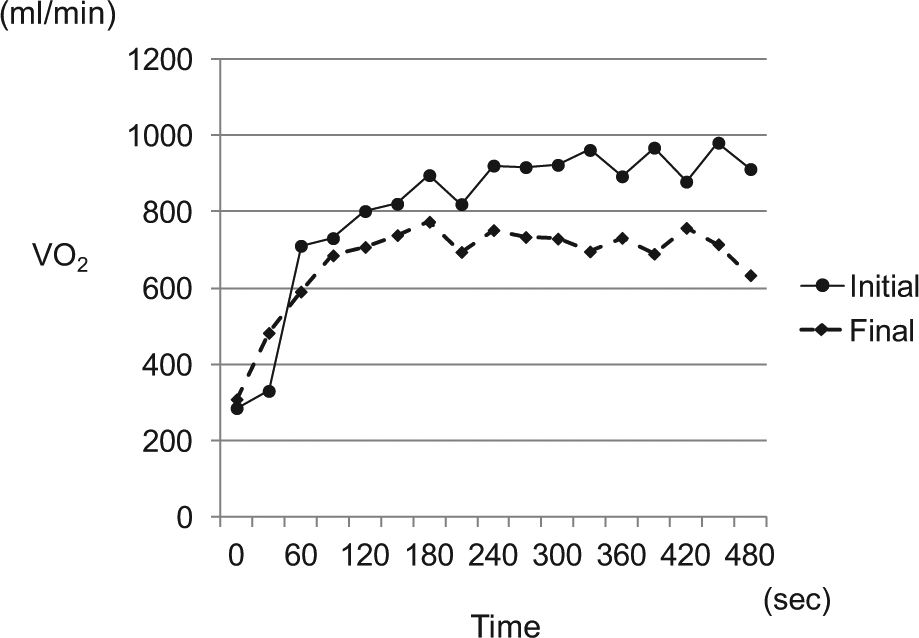
Oxygen consumption rate (VO2) during anti-gravity treadmill training.
Discussion
In space, the lack of gravity can cause bone loss and muscle atrophy; contrarily, on Earth, gravity can cause musculoskeletal disease. 7 From these points of view, the anti-gravity treadmill, which can provide body weight support by as much as 80%, has been developed. Patil et al. 8 measured the knee forces of patients who had undergone total knee arthroplasty on an anti-gravity treadmill and reported that it enabled them to control and decrease forces on the knee. Regarding cardiopulmonary function, Hoffman and Donaghe 9 showed that VO2 and heart rate for the same treadmill speed are reduced with increase in body weight support.
After the anti-gravity treadmill was developed, a number of clinical and basic studies have been performed to assess its effectiveness for patients with lower extremity arthritis and other disorders that interfere with the ability to walk, and some favorable data have been published.10,11 However, to date, there appear to have been no reports of its efficacy for the lower limb amputees.
Concerning below-knee amputees, standing-position training, balance training, and walk training are the generally recommended methods for prosthetic rehabilitation. After achieving prosthetic gait ability using parallel bars, prosthetic gait is typically practiced away from the parallel bar. However, since prosthetic gait requires more physical strength than normal walking, some aged patients cannot acquire practical prosthetic gait. 12
In this study, the eyesight of the patient was poor and he underwent hemodialysis because of diabetic complications, so he was not in the habit of taking regular exercise. Furthermore, the physical and mental activities of the patient were decreased because he could not walk for long distances during the perioperative period. Therefore, the patient could not acquire practical prosthetic gait ability until discharge because he felt exhausted during rehabilitation, and it was considered difficult to elevate his physical and mental activities to develop prosthetic gait. Therefore, the anti-gravity treadmill training was introduced as a way of reducing the load on the lower extremity and cardiopulmonary function, with little risk of falling.
Adjustments can be made to the anti-gravity treadmill for percent body weight support, walking speed, and effort required by changing the incline of the treadmill. However, Finch et al. 13 reported that the percentage of total double-limb support time was decreased by introducing the support of 50% of body weight, and Mercer et al. 14 showed that the muscle activity of the lower extremity was decreased by body weight reduction. These findings imply that the prosthesis should bear a certain minimum load to ensure successful prosthetic rehabilitation. Therefore, in this study, treadmill training commenced at 40% of body weight support. Initial treadmill speed was 0.56–0.83 m/s and exercise time was 10 min, values were estimated based on Borg’s scale for walking and cardiopulmonary effort. The incline of the treadmill was not changed, in order to reduce extra burden on the prosthetic gait. Providing gait guidance was straightforward because of the transparency of the supporting air chamber. On the treadmill, the kick-off of the legs was easy, however, careful guidance for the forward swing of the legs was important to obtain stable gait. Since patients cannot see their legs on the current commercially available anti-gravity treadmill, some minor changes, such as mounting a lower leg monitor, were considered necessary. In this study, the treadmill reaction forces, velocity, and duration of the exercise were gradually increased because prosthetic gait ability and physical strength steadily improved.
As mentioned earlier, the mental activity of the patient was reduced because of the long period experiencing difficulty in walking because of his diabetic complications. Although his self-efficacy was temporarily elevated at the introduction of prosthetic rehabilitation, it remained low until the introduction of anti-gravity treadmill training. Since he could walk comfortably, faster, and longer on the anti-gravity treadmill, his self-efficacy was markedly improved just after he began the treadmill training. This unexpected benefit was not anticipated before the introduction of treadmill training. Since his self-efficacy was markedly elevated, he quickly developed a positive attitude to participating in the training and his gait was quickly and smoothly stabilized.
Cardiopulmonary function measured as oxygen consumption rate at the final evaluation was lower than that at the initial examination, demonstrating improvement in motion efficiency following anti-gravity treadmill training. In the 6-min walking distance test, the Borg rating of perceived exertion at the initial examination was the same as that at the final examination. 15 However, since the walking distance at the final evaluation was longer than that initially, this result, too, might suggest an improvement in motion efficiency after anti-gravity treadmill training.
In this study, the walking training on the floor was briefly performed after the treadmill training. With the stabilization of gait on the treadmill, the gait on the floor was also stabilized and walking speed was elevated as well. Together with the elevation of his physical strength and vitality, the patient was finally able to walk with a T-cane.
Conclusion
A case of below-knee amputation caused by diabetic gangrene was reported, where prosthetic rehabilitation using an anti-gravity treadmill was shown to be successful and efficient. Stable walking exercises could be performed with little risk of falling. After training, the self-efficacy and exercise tolerance were clearly elevated and the patient progressed quickly and efficiently to acquire the ability of prosthetic gait with the aid of a T-cane. The anti-gravity treadmill is therefore recommended as a useful instrument for prosthetic rehabilitation for below-knee amputees.
Footnotes
Author contribution
All authors contributed equally in the preparation of this article.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This study received no specific grant from any funding agency in the public or commercial sectors.