
Abstract
Background: Measurement of ankle joint dorsiflexion is an essential examination technique that needs to be performed prior to prescription of foot orthoses since the presence or absence of ankle equinus will affect the design of such devices. The purpose of this study was to investigate the effect of foot posture on sagittal plane kinematics of various foot segments during passive dorsiflexion.
Study Design: Comparative repeated measures design.
Objectives: To determine the effect of foot posture on inter segmental kinematics during passive dorsiflexion.
Methods: An optoelectronic movement analysis system was employed to collect kinematic data. A validated marker set (Oxford Foot Model) was applied to 16 subjects (12 males, 4 females) with a mean age of 35.5 years (range 20–56 years), who provided informed consent. An upward force was applied to the forefoot until maximum resistance. Sagittal movement of the hindfoot and forefoot segments along with the whole foot movement were analyzed in the pronated, neutral and supinated foot postures.
Results: While maximum foot dorsiflexion angle showed a significant difference between the three postures (p=0.000) the actual recorded difference between the neutral and supinated postures was only 2.49°. For the hindfoot and forefoot segments, mean angle range of movement for the pronated foot posture was significantly higher than the other foot postures. The forefoot to hindfoot angle demonstrated a significant (p=0.005) increase during dorsiflexion between the pronated and supinated postures. These results indicate that during passive dorsiflexion, the forefoot travels through a greater degree of movement than the hindfoot.
Conclusions: While the maximum foot dorsiflexion angle differs significantly between the pronated and supinated foot postures, hindfoot movement also varies significantly between foot postures. Furthermore, the forefoot to tibia angle travels through a greater range than the hindfoot to tibia angle, in all three foot postures. The hindfoot to forefoot angle does not remain constant during passive dorsiflexion, but increases upon application of a dorsiflexing force, indicating that the forefoot movement cannot be eliminated completely by placing the foot in any particular posture.
Keywords
Clinical relevance
The prescription of foot orthoses depends on a thorough examination of the foot that includes ankle dorsiflexion measurement, from which ankle equinus may be diagnosed. However, the techniques commonly used may not be giving us the actual ankle dorsiflexion angle but a summation of ankle and forefoot angles which means that on many occasions we may be arriving at the wrong diagnosis.
Introduction
It is indicated that prior to prescribing any foot orthoses, a thorough foot examination, including passive joint range of motion measurement, is essential. 1 The maximum dorsiflexion angle is normally measured to determine ankle equinus (which is defined as a lack of ankle joint dorsiflexion 2 ), since the assessment and presence of this condition is critical when considering orthotic management. 3 In a patient with limited mobility at the ankle, orthoses may be worn to make the individual’s walking safer and more functional and to provide dynamic stretching of the triceps surae. 4
Examination of the range of motion of the ankle joint involves the dorsiflexion of the foot through the application of force at the metatarsophalangeal joint area. The maximum ankle dorsiflexion angle is assessed either through visual estimation, 5 goniometry,6, 7 or with the use of one of the various ankle measuring devices.8-11 Among other goniometric techniques, one common type of measurement of maximum dorsiflexion involves alignment of the stable arm of the goniometer between the lateral head of the fibula and the lateral malleolus, while the moving arm is held along the lateral border of the foot up to the 5th metatarsal head. The subtalar joint is placed in neutral position and a dorsiflexing force is applied to the metatarsophalangeal joints.2, 7 While ankle and foot dorsiflexion during gait have been studied extensively, there is little information regarding passive dorsiflexion, such as manual dorsiflexion of the foot. As the resultant angle may influence treatment given to the patient, such as the prescription of foot orthoses, it is essential to know what is happening when this force is applied to the forefoot and the foot is dorsiflexed.
Where does dorsiflexion actually occur?
The degrees of freedom (DOF) of the ankle joint has been debated for some time. 12 Using eight cadaveric feet in a jig with markers attached directly to the bones, it has been shown that there is approximately five of movement between the talus and calcaneus during the first 25% of the stance phase of gait. 13 During late stance, these two bones rotate together and function as one unit. Leardini and colleagues have conducted extensive studies on ankle joint modelling using a number of dissected limbs. Their conclusions indicate that, during passive dorsiflexion, the ankle joint complex behaves as a single DOF system with large sagittal motions occurring mostly at the tibiotalar joint, with very little sagittal plane motion occurring at the subtalar joint.14, 15
These claims are further supported by Franci et al. who suggest a further modelling of the human ankle joint as a one-DOF spatial mechanism. 12 The use of computed tomography used to analyze the range of motion of the ankle confirmed that nearly all dorsiflexion and plantarflexion occurs in the talocrural joint, with increased inversion and axial rotation at this joint being prevalent only in pathologic ankles. This led researchers to conclude that dorsiflexion/plantarflexion is restricted to the talocrural joint. 16
However, besides ankle joint complex movement, Lundgren et al. have demonstrated that, during gait, the medial column may produce more movement than the ankle joint itself. In this study, which involved insertion of bone pins for more accurate kinematic analysis utilizing a 3D motion capture system, up to 17.6° of sagittal movement was obtained in the medial column, as compared to ankle joint movement which was just 15.3°. 17 In an earlier study, although the talocrural joint was found to account for most of the rotation around its axis occurring from 30° of plantar flexion to 30° of dorsiflexion, there was a substantial contribution from the joints of the arch. 18
An important aspect of clinical ankle dorsiflexion measurement is foot posture, i.e. the effect of pronation and supination. Previous trials found a significant difference between the neutral position and the pronated position 19 of up to 10° of dorsiflexion. 20 Both studies concluded that the measurement of ankle dorsiflexion should be performed with the subtalar joint at neutral position.
The procedure behind the clinical examination of ankle dorsiflexion has an important assumption that has never been scientifically assessed using accurate measurement systems. Normally, the foot is placed in neutral position and the foot is dorsiflexed by applying a force to the metatarsophalangeal joints with the assumption that the movement occurs only at the ankle joint. 2 However, the foot is composed of several segments, with movement occurring between the various joints, which may be quite extensive during gait. Hypermobility of the forefoot, for example, is a very common finding during clinical examination. This forefoot movement may, in fact, be providing false results; ankle equinus may not be diagnosed because the foot has bypassed the 0 degree mark or, according to some clinical theories, has exceeded 10 degrees of dorsiflexion. These 10 degrees may, in fact, be mostly attained by upward movement of the forefoot at the midtarsal joint, and not at the ankle joint itself since compensation to supplement limited ankle motion is to use midtarsal joint dorsiflexion in conjunction with subtalar joint pronation. 4 This would be a clear case of misdiagnosis and a patient with ankle equinus may not get the required treatment because of an apparent ‘normal’ amount of dorsiflexion. This may result in a midtarsal joint break, which is noted as a characteristic of equinus feet.
The main aims of the study were to investigate ankle dorsiflexion at the various foot postures and intrinsic foot segment motion during passive ankle joint dorsiflexion, as would happen during the clinical examination of ankle range of motion. It was hypothesized that varying foot posture during passive ankle joint examination (1) significantly affects the mean Maximum Foot dorsiflexion angle with a higher angle at pronated position; (2) affects the amount of hindfoot movement; and (3) increases the forefoot to hindfoot angle.
Methods
Sixteen healthy subjects (4 females, 12 males) with a mean age of 35.5 years (range 20–56 years) who provided informed consent were invited to participate in this study. Ethical approval was sought from, and granted by, the university ethics committee. Exclusion criteria included neurological disease, history of foot surgery and obvious foot deformity.
Height and weight, leg length and knee and ankle width were recorded for each subject to create their corresponding lower-limb kinematic model. An eight-camera optoelectronic system (Vicon, OMG, Oxford, UK) was employed to collect the kinematic data at 100 Hz. Reflective markers were placed by the primary researcher (a clinician, AG), using the Oxford Foot Model marker set (Figure 1), then cross-checked by an experienced researcher (TLC). This particular marker set, which has previously been shown to be reliable and repeatable, divides the foot into hindfoot, forefoot, hallux, and tibial segments. 21 After a standing static calibration, the markers were checked again and another static calibration was carried out with the subject sitting on a flat, patient examination couch with the knees extended, at which position data collection was subsequently carried out. This sitting calibration ensured that markers remained in the required position during the subjects’ movement from a standing to a sitting position. A supine position would have made it impossible to conduct the experiment; thus subjects remained seated so that the posterior superior iliac spine markers were visible to the rearmost cameras at all times.

Marker configuration used within data capture (Oxford Foot model).
Each subject’s knee was held parallel to the couch surface in the frontal plane. Subjects sat with arms positioned at the rear, gripping the sides of the couch in order to steady themselves and to ensure that the camera’s view was not obstructed at any time.
Each subject’s right foot was held sequentially in one of the three possible postures (i.e. maximally pronated, subtalar neutral or maximally supinated). The sequence of these foot postures was determined randomly by the other researcher to avoid any bias that would affect the results. Consistent placement of the foot at neutral position is notoriously difficult, however this is the recommended position for this procedure and it is used in clinical practice, often by practitioners with little experience. A single clinician with 25 years’ experience, who normally makes an assessment of subtalar joint neutral position at least five times per day, determined subtalar joint position. 19 An intratester reliability coefficient of 0.88 for clinicians who perform this technique at least once monthly, has been demonstrated. 22 Subtalar position was determined by the talo-navicular congruency method: for neutral position, the head of the talus was palpated and felt equally both medially and laterally, and the curves above and below the malleoli were used to verify neutral position placement. When placed in the pronated position, only the medial head of the talus was palpable, while in the supinated position only the lateral head was palpable. The forefoot was loaded to initial resistance by the application of force at the metatarsophalangeal joint area, then it was dorsiflexed to the end of motion of the ankle joint until there was no further dorsiflexion movement available, ensuring that the subtalar joint did not move out of the determined posture during the process. It was held in that position for three seconds before being released. Ten repetitions for each posture were done, for a total of 30 trials per subject.
Each subject’s data were normalized and then averaged for each condition. Since the investigator’s hand holding the foot at neutral position could interfere with the camera views, the first five correct trial results out of 10 were recorded for each posture for each participant. Thus a total of 15 trials were analyzed for each participant. From the five correct trials for each foot posture, the means of the required angles were calculated. Appropriate repeated measures ANOVA was carried out using SPSS 17.0, with the level of significance set at p=<0.005 throughout all statistical analysis.
Results and statistical analysis
Maximum foot dorsiflexion angle
The mean maximum foot dorsiflexion angles in the pronated, neutral and supinated postures are shown in Table 1 and illustrated in Figure 2.
Scores for mean maximum foot dorsiflexion angle and mean hindfoot to forefoot range of movement in the pronated, neutral and supinated positions.
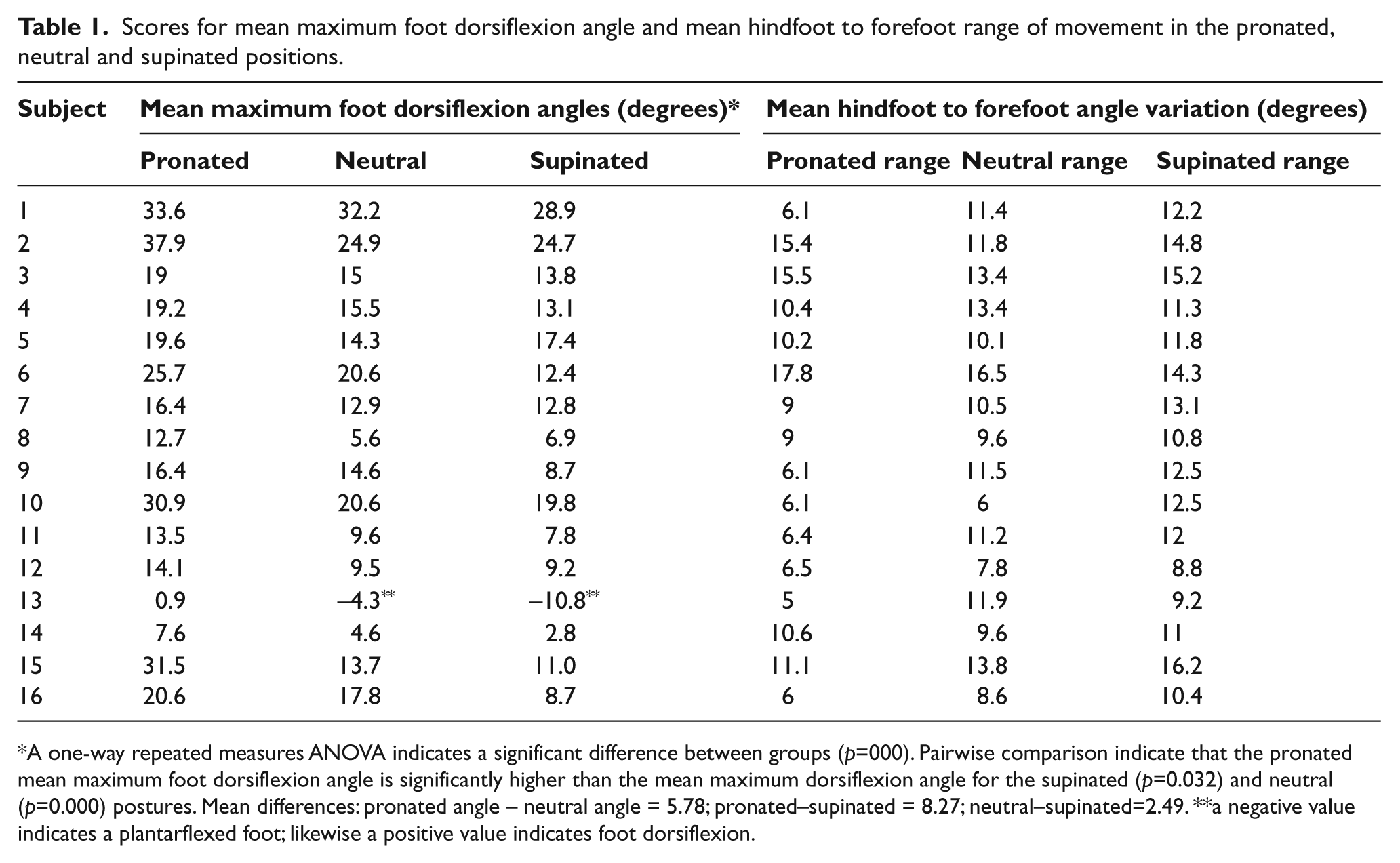
A one-way repeated measures ANOVA indicates a significant difference between groups (p=000). Pairwise comparison indicate that the pronated mean maximum foot dorsiflexion angle is significantly higher than the mean maximum dorsiflexion angle for the supinated (p=0.032) and neutral (p=0.000) postures. Mean differences: pronated angle – neutral angle = 5.78; pronated–supinated = 8.27; neutral–supinated=2.49. **a negative value indicates a plantarflexed foot; likewise a positive value indicates foot dorsiflexion.
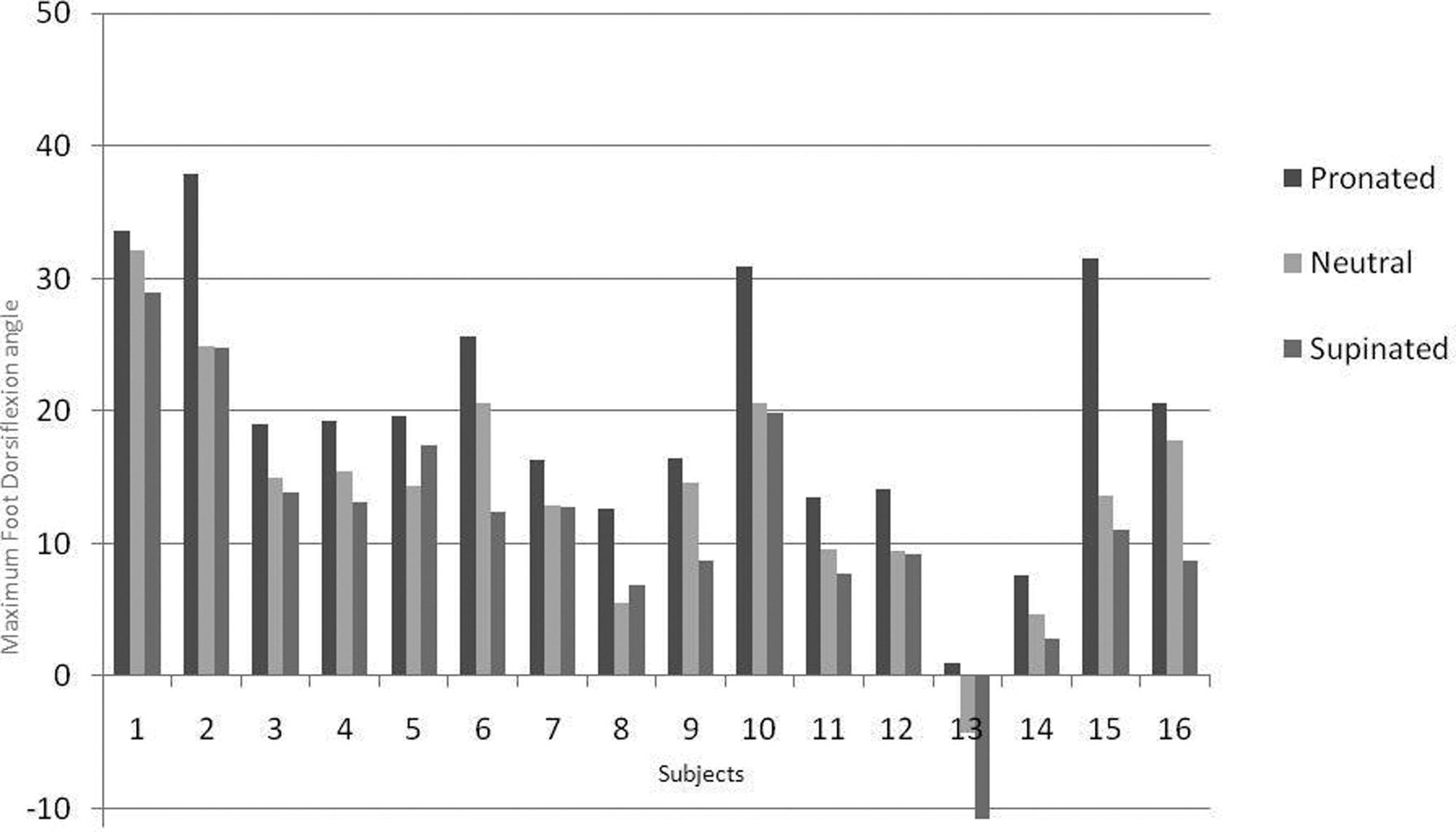
Maximum Foot Posture Angle in three postures under investigation.
A one-way repeated measures ANOVA was conducted to compare the mean maximum foot dorsiflexion angle between the three foot postures, which indicated a significant difference between groups (p=0.000). The mean maximum foot dorsiflexion angle is significantly different in both the pronated to neutral postures and pronated to supinated postures (p=0.000). Likewise, there is also a significant difference in maximum foot dorsiflexion between the neutral and supinated postures (p=0.032).
The difference between the mean maximum foot dorsiflexion angle between pronated and neutral is 5.78°; between pronated and supinated is 8.27°, while between supinated and neutral it is only 2.49°.
As shown in Figure 2, the mean maximum pronated foot dorsiflexion angle is higher for all participants. The general trend indicates that the maximum angle is reached in the pronated posture, reduced in the neutral posture, further reduced in the supinated posture. This is true in 14 out of the 16 participants: 87.5% of subjects.
Hindfoot and forefoot movement
A two-way ANOVA was used to compare the mean angle range of movement of the hindfoot and forefoot at each of the foot postures.
The mean angle ranges of movement differ significantly between the three foot postures for both hindfoot and forefoot (p=0.008). The mean angle range of movement for the pronated foot posture is significantly higher than the other foot postures both for the forefoot and hindfoot segments as shown in Table 2.
Descriptive statistics (angle range of movement for forefoot and hindfoot).
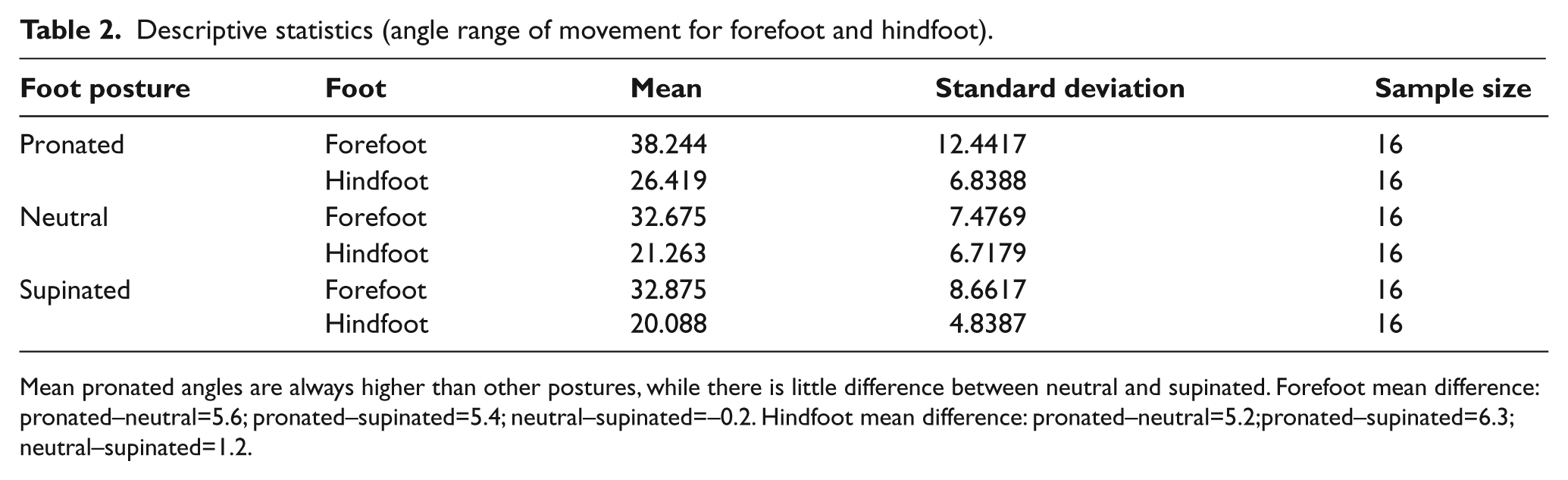
Mean pronated angles are always higher than other postures, while there is little difference between neutral and supinated. Forefoot mean difference: pronated–neutral=5.6; pronated–supinated=5.4; neutral–supinated=–0.2. Hindfoot mean difference: pronated–neutral=5.2;pronated–supinated=6.3; neutral–supinated=1.2.
Although the trajectories for the forefoot and hindfoot are fairly parallel (i.e. what is happening in the forefoot is also happening in the hindfoot), forefoot scores are significantly higher (Figure 3). Thus the forefoot range of motion is greater than the hindfoot range of motion throughout the three foot postures: there is always more forefoot range of motion than the hindfoot in all foot postures. Pronated to neutral posture (p=0.027) and pronated to supinated posture difference (p=0.014) are both significant. On the other hand, there is no significant difference between the neutral and supinated postures (p=0.969).
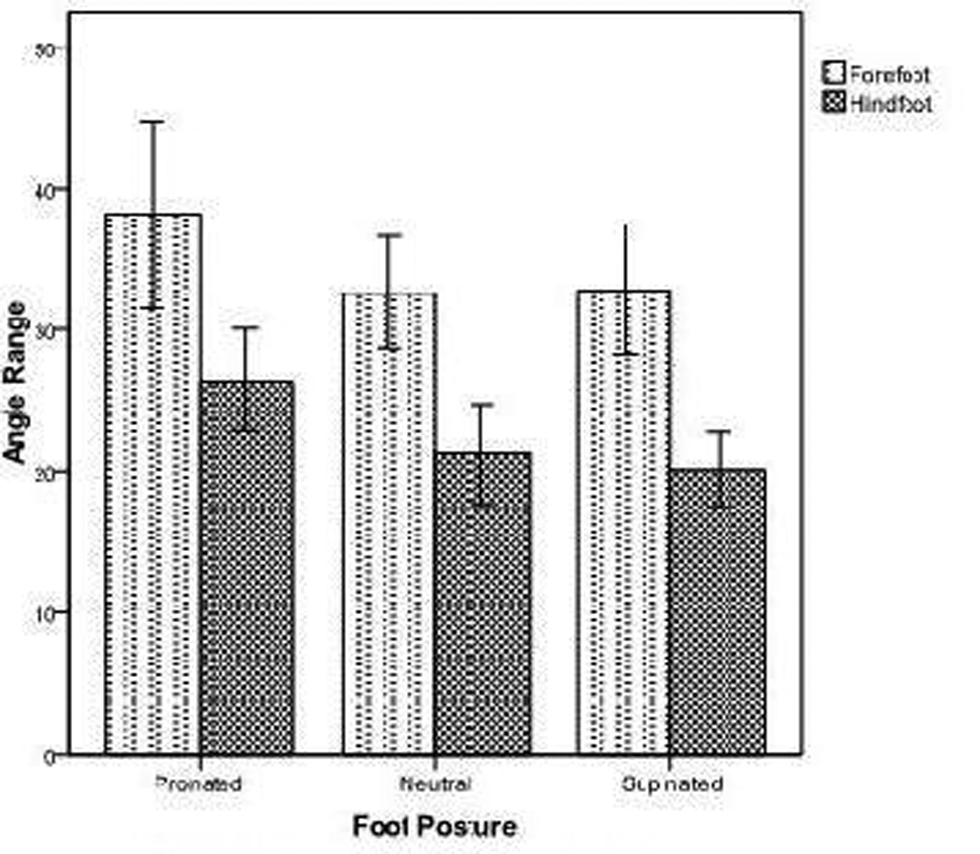
Foot Posture vs. Angle Range.
Forefoot to hindfoot angle
According to the way that the Oxford Foot Model estimates the forefoot to hindfoot angle, if there is only hindfoot movement with no forefoot movement relative to the hindfoot, this angle would remain constant during the dorsiflexing procedure. However, with the application of force during dorsiflexion, the angle increased, then remained at the same position during the period of time when the foot was held at a dorsiflexed position. This then decreased again as the foot was released.
A one-way repeated measures ANOVA indicated a significant difference for the forefoot to hindfoot angle variation (p=0.007). Pairwise comparisons demonstrated a non-significant difference between pronated and neutral (p=0.139) and neutral and supinated (p=0.147) but a significant difference between pronated and supinated postures (p=0.005).
Discussion
Although ankle joint dorsiflexion assessment is carried out routinely, little is known about what actually happens to the various foot segments, or indeed the foot itself, when a dorsiflexing force is applied to the forefoot. Thus this research was carried out to investigate sagittal plane kinematics of passive ankle joint dorsiflexion, such as would occur during the measurement of the maximum ankle dorsiflexion angle. As the foot is multi-segmental, it is important to determine whether there is pure ankle joint movement or whether there is forefoot movement as well during this process. Root theory advocates the use of subtalar joint neutral position and to lock forefoot movement at the midtarsal joint. Issues regarding both the neutral position 22 and the midtarsal joint locking mechanism have been amply discussed elsewhere.
This procedure has thus never been investigated using a structured and accurate method such as the Oxford Foot Model. Whereas in most protocols used within traditional 3D motion capture systems, the foot is treated as a single rigid lever, this model can measure segmental motion within the foot.
Two previous studies, using measurements obtained from projections of 35mm slides 19 and video 20 that investigated the effect of foot posture on maximum ankle dorsiflexion, both concluded that the pronated foot posture produces significantly more dorsiflexion than the other postures. Although these studies also concluded that ideally ankle angle assessment should be carried out at subtalar joint neutral, Woodburn advocated reverting to a ‘slightly supinated position’ when there is uncertainty in establishing a neutral position, 20 a conclusion confirmed by the results of this trial. Furthermore, the study by Woodburn established a difference of 3.5° between the neutral and supinated posture, 20 which is also supported by this trial since the difference amounted to 2.49°.
Not only is the effect of foot posture on maximum foot dorsiflexion important because of issues of unreliability in placing the subtalar joint at neutral position, 22 but movement within the foot itself had to be investigated to verify whether, after placing the subtalar joint at neutral and ‘locking’ the midtarsal joint, the only movement left during manual dorsiflexion of the foot is indeed pure ankle joint movement. 2
The results obtained confirm the conclusion by the two previous studies; i.e. that in the pronated position, there is significantly more dorsiflexion of the foot in all subjects. This would appear to point out that, if one is measuring ankle dorsiflexion, the pronated position needs to be avoided because it would give larger, possibly false, results, which are significantly different to both the neutral and supinated positions.
There is a statistically significant difference between maximum foot dorsiflexion angle between all three postures. These differences between the pronated and neutral postures and pronated and supinated postures are quite significant, both statistically (p=0.000) and clinically (5.78° and 8.27° respectively).
Although there is a statistically significant difference between the neutral and supinated posture, the clinical significance is debateable since this amounts to just 2.49°. It is unlikely that this difference will be detected using normal clinical methods which are not as accurate as an eight-camera optoelectronic system. Even so, the clinical relevance of such a difference is questionable and unlikely to affect clinical decisions.
Unlike the previous two studies, it appears that the neutral position does not provide consistent results; neutral angle range lies between the pronated and supinated postures in 87.5% of subjects. This could perhaps be due to problems with consistent placement of the subtalar joint at neutral. If consistency in placement by an experienced clinician under controlled experimental conditions was an issue, the implications for uncontrolled clinical examination must be borne in mind.
Another important consideration is that the forefoot appears to move through a greater range than the hindfoot in all three foot postures (Figure 2); i.e. sagittal forefoot movement cannot be eliminated by putting the foot in any particular posture. Thus it is clear that, when applied to clinical measurement of ankle dorsiflexion, both ankle and forefoot movement is being measured irrespective of the position the foot is put in. Thus the term ‘foot dorsiflexion’ would be more applicable to ‘ankle dorsiflexion’ in this case. This may be of significant importance as sometimes there can actually be more movement at the forefoot than at the ankle, as also pointed out by Woodburn who concluded that ‘with a pronated subtalar joint we may miss a diagnosis of true limitation’. 20 On the other hand, our results show that there is little clinical difference between the neutral and maximally supinated postures, which is not in agreement with the statement that ‘with a supinated subtalar joint we falsely diagnose ankle equinus’. 20
Using a different, yet clinically relevant methodology to previously published papers, the current study has obtained different results for hindfoot movement. Surprisingly, hindfoot movement is not constant as reported elsewhere and appears to vary with posture as well. As the amount of movement at the ankle joint should not be affected by changing foot posture, this can only happen at the subtalar joint; namely the sagittal plane component of movement of this articulation. This is in total disagreement with other studies which had concluded that there is no sagittal plane movement at this joint in a non-weightbearing situation.14, 15
There were some limitations to this study, including the small sample size, which consequently points to a need for another similar study on a larger scale. The exclusion of subjects with specific foot conditions, and patient populations, imply that the results of this study cannot be inferred to actual patients, but only to healthy subjects. Children would also have possibly produced a different outcome due to their increased foot flexibility. Subject 13 had an obvious limitation of dorsiflexion and perhaps should have been excluded from the study in order to obtain a more homogenous result.
Conclusions
The amount of sagittal foot movement, including the range of forefoot and hindfoot movement, varies depending on foot posture. Foot dorsiflexion was maximum at the pronated posture in all participants; it was least in the supinated posture in 87.5% of subjects. Changing posture does not totally eliminate forefoot movement.
When dorsiflexing the foot using a manual force on the plantar metatarsophalangeal joint area, the forefoot moved through a greater angle than the hindfoot in all the investigated foot postures. This was also confirmed by the forefoot to hindfoot angle, which increased with the application of force during dorsiflexion. This implies that the mid-tarsal joint locking mechanism does not function at neutral position, that pure ankle dorsiflexion cannot be obtained in this manner and thus any apparatus, such as the traditional goniometric method, that measures foot dorsiflexion across the forefoot and hindfoot may actually be measuring the summation of the movement of both foot segments.
Thus foot posture is an important element that must be borne in mind when conducting foot dorsiflexion measurements.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.