
Abstract
Abstract
Purpose
Paediatric foot surgery is often performed to restore anatomical shape or range of movement (ROM). The purpose of this study was to determine how foot morphology and ROM are associated with foot function in children aged five to 16 years of age.
Methods
Participants included 89 patients with foot disorders and 58 healthy controls. In addition to measuring children's foot alignment and ankle ROM, children and parents completed the Oxford Ankle and Foot Questionnaire (OxAFQ).
Results
Mean age was 10.3 years for patients and 10.6 years for controls; 53 of 89 patients had clubfoot. All foot measurements and scores on the OxAFQ significantly differed (p < 0.001) between patients and controls. Patients and their parents significantly differed on the physical (p = 0.03) and emotional (p = 0.02) domains of the OxAFQ, with parents’ ratings being lower than their children. Moderate correlations (r = 0.54 to 0.059; p < 0.001) were found between physical domain (reported by parents on the OxAFQ) and dorsiflexion-knee flexed, and foot- arc-of-movement. Moderate correlations were found between physical domain (reported by children on OxAFQ) and foot-arc-of-movement (r = 0.56; p < 0.001). Patients in the surgical group showed moderate correlations (r = 0.57;, p < 0.001) between physical domain (reported by children on OxAFQ) and plantar flexion, and foot arc-of-movement. The control group and the patients in non-surgical subgroup showed no significant correlations.
Conclusion
Plantar flexion, arc of ankle ROM and hindfoot alignment impact foot function in children with foot deformities. Parents report significantly lower scores on the OxAFQ when judging foot functioning.
Level of evidence
Level II. Prognostic Studies
Introduction
Foot and ankle problems are common in children 1 and are the most common reason for children to present to an orthopaedic surgeon. 2 Foot pathology in children may be due to congenital deformities, clinical syndromes, neuromuscular conditions or trauma.3–6 The foot is the most distal segment in the lower extremity, acting as a base of support upon which the body maintains balance, allowing the individual to interact with the environment and to perform activities. The foot adapts to the ground surface, aids in shock absorption and acts as a rigid lever that propels the body forward during push off. 7 In the past, evaluation of the foot and treatment of malalignment has depended on a theoretically conceived ‘ideal foot’, but more recently it has been recognized that the ‘ideal foot’ is an invalid theoretical concept that should be replaced by a reference-based deviation from usual observation. 8
Treatment for foot disorders aims to prevent, correct or accommodate deformity, manage symptoms and improve physical function and quality of life. Therapeutic options for children with foot problems include medication, physiotherapy, casting, orthotics and/or surgery. Surgical treatment options include soft-tissue procedures, osteotomies and/or arthrodesis, depending on the problems to be addressed and the age of the patient. Although achieving dorsiflexion is often an important goal of surgical treatment, it is unclear how and to what extent foot function is influenced by foot morphology and range of movement (ROM).
When parents and children/adolescents with illnesses are asked about their functioning and quality of life, self and parental reports are not always congruent. Parents tend to underestimate their child's functioning or quality of life, especially when the quality of life is dependent on the interaction between the parent and child/adolescent.4,9–11 Little is known about whether parents of children/adolescents with foot abnormalities have similar perspectives on the functioning of the foot. Given the young age of these children, parents tend to speak on behalf of their children, thus it would be important to understand whether their perspectives converge in order to provide best care.
Objectives
The purpose of this study was to determine how foot morphology and ROM are associated with foot function, as measured by the Oxford Ankle and Foot Questionnaire (OxAFQ),3–5 in children aged five to 16 years. It was hypothesized that: 1) dorsiflexion and plantar flexion correlate with foot function; 2) deviations in hindfoot alignment negatively impact foot function; and 3) patients (defined as those with a foot disorder) and their parents would express different perspectives on foot function.
Patients and methods
Participants
To detect a 0.30 (moderate) Pearson correlation between measures of foot morphology and OxAFQ at a 0.05 level of significance, with a power of 0.80, 85 participants were needed. Assuming a mean difference between patients and controls of 8 for the OxAFQ domains with power 0.8 and a type I error probability of 0.05, 4 we required 56 patients and 56 healthy controls. Therefore, we recruited 147 participants: 89 patients with foot disorders and 58 healthy controls.
All participants were between five and 16 years of age. Two groups of participants were recruited for this study: patients with foot disorders and healthy controls. Patients with foot disorders were recruited sequentially from the Orthopaedic Clinic at the Hospital for Sick Children, Toronto, Canada. Healthy controls were children with no complaints or prior history of a foot disorder. Healthy controls comprised of children who came to the hospital accompanying patients or children of hospital staff or volunteers.
Patients with a foot disorder and a community ambulatory status were included in the study; however, they were excluded if they had a concomitant disorder affecting other segments of the lower limb and/or underlying neuromuscular or metabolic conditions.
Questionnaire
The OxAFQ assesses child or parent reported health status for children with foot and ankle problems aged between five and 16 years.3–5 The 15 questions are divided across three subscales (i.e. physical domain assessing general activity limitations; school & play assesses participation restrictions; emotional domain assessing to what extent a child is bothered about their foot or ankle because of the appearance or the way people treat them) and one single item (i.e. if the child can or cannot wear footwear). Children (OxAFQ-C) and parents (OxAFQ-P) each completed the questionnaire. Items were scored from 4 (never) to 0 (always) indicating how frequently the issue affects the child. Item scores were added together in each of the three domains with no total test score. The summed score in each domain was transformed to a decimal, where 0 represents the poorest score and 1 the best.
Procedure
Participants completed a clinical evaluation, and each child and one of their parents completed the OxAFQ. The following demographic data were also collected: age, sex, clinical diagnosis, previous treatment, ethnicity, siblings and education of parents. Participants were asked if they had any foot pain over the week immediately previous to their clinic visit. All clinical assessments were performed by a fellowship-trained paediatric orthopaedic surgeon, blinded to the questionnaire scores.
Clinical evaluation
Although it is common to differentiate hindfoot (talus and calcaneus), midfoot (remaining tarsal bones) and forefoot (metatarsals and toes), we distinguished ‘hindfoot’ (tarsus) from the ‘forefoot’ with separate measures for joint movement and weight-bearing deformity. 12 While foot and ankle movement have been evaluated in different ways in the past, we used the Ad Hoc Committee of Terminology of the Japanese Society for Surgery of the Foot and Ankle to describe movement of the ankle and foot.13–16 Joint movements are expressed in three planes: transverse (horizontal), sagittal and frontal (coronal). The neutral zero starting position is the position standing with the long axis of both feet parallel each other. Sagittal movement of the foot/ankle is described as dorsiflexion/plantar flexion. 15 In the coronal plane, ‘valgus’ describes that the hindfoot is angulated outward relatively to the sagittal body axis, while ‘varus’ describes that the hindfoot is angulated inward. 10 ‘Cavus’ is used to describe a high arch. 17 ‘Flatfoot’ is used to describe a weight-bearing foot with a low or absent longitudinal arch. 12 The long axis of the heel (heel bisector) should intersect the second metatarsal head: if the forefoot is deviated inward relatively to the hindfoot, this deformity is described as ‘adductus’; if the forefoot is deviated outward relatively to the hindfoot, this deformity is described as ‘abductus’. 18
Foot morphology and ROM were assessed by using a goniometer to measure: hindfoot alignment (varus/valgus), forefoot alignment (adduction/abduction) and ROM of the foot and ankle (dorsiflexion with the knee flexed and extended, and plantar flexion). Each foot was also described in terms of hindfoot alignment (varus, neutral, valgus), foot arch (cavus, neutral, flat) and forefoot alignment (adductus, neutral, abductus). Hindfoot deviation was measured with a goniometer in degrees of valgus or varus, considering zero degrees of deviation as the heel in neutral position, perpendicular to the floor, in the standing position. Dorsiflexion and plantar flexion were measured with the knee extended and with 90° of knee flexion, maintaining the foot supinated and keeping one arm of the goniometer parallel to the fifth metatarsal, while the other arm was put on the midline of the fibula, with the fibular head as a reference point. For the purpose of this study, we were also interested in considering the arc-of-movement in our analysis and defined it as the combined dorsiflexion and plantar flexion ROM. A foot was considered to be ‘normally shaped’ if hindfoot valgus was < 10° and there was no forefoot abductus or adductus. Any degree of hindfoot varus was considered abnormal.
Statistical analysis
Pearson's correlation coefficient (r) was used to quantify the relationship between OxAFQ and measurements of foot morphology and ROM. The t-test was used to detect differences in OxAFQ between patients and controls and paired t-test was used to detect differences between patients and their parents. In all, 87 patients and their parents were compared on the OxAFQ, scores, one patient was not included in the comparison because their parent did not complete the questionnaire and thus could not be included in a paired t-test. In patients with bilateral foot disorders, only the worst foot measurements were considered for the purpose of statistical analysis. We further performed subgroup analysis for patients who received surgery (patient surgical group) and patients who did not receive surgery (patient non-surgical group). We also performed subgroup analysis comparing clubfoot with idiopathic toe-walkers and clubfoot with others (tarsal coalition, idiopathic flatfoot and others).
Results
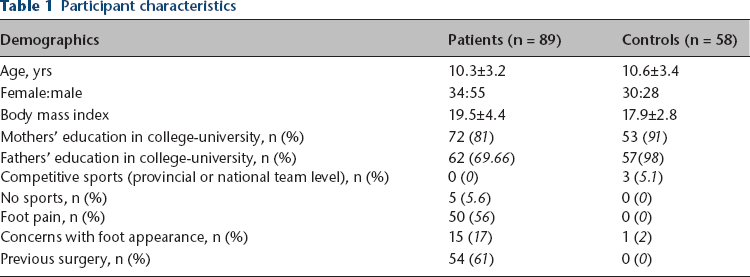
We recruited 147 participants for this study: 89 patients with foot disorders and 58 healthy controls. The mean age was 10.3±3.2 years for patients and 10.6±3.4 years for controls; 62% of patients and 48% of controls were male; 61% of patients had a previous foot surgery (Table 1). In the patient group, 17% of participants had concerns about their foot appearance, compared with 2% of participants in the control group. In patients, 56% had foot pain compared with 0% of controls.
Participant characteristics
Of the 89 patients, 36 had normally shaped feet, 19 had planovalgus abducted feet, ten had cavovarus adducted feet and 27 had feet with deformities that did not fit these two patterns. A number of aetiologies were noted in the patient group, with clubfoot being the most common (Table 2). There were 19 idiopathic toe-walkers, six of whom had treatment with serial casting, with one of these patients further having a bilateral percutaneous tendon Achilles lengthening. There were six patients with tarsal coalitions: calcaneonavicular in three patients (one patient had resection and two had no surgery at the time of the study) and talocalcaneal in the remaining three (one patient had excision, one had excision and surgery and the remaining patient did not have any treatment at the time of this study). There were three patients with idiopathic flatfoot and none of them had surgery. Although these participants had a flat arch and hindfoot valgus greater than 5°, their inclusion in the patient group was not based on a specific threshold of hindfoot valgus, but due to the fact that they have presented to our hospital with a symptomatic planovalgus foot: one patient had problems with shoe-wear and two patients had pain. When examining foot measurements, patients and controls significantly differed across all foot measurements. When the patient group was further subdivided to examine those in the surgical and non-surgical group, significant differences were seen between groups on foot arc-of-movement (29.04 sd 14.87, surgical group; 36.34 sd 12.39, non-surgical group; p = 0.01) and plantar flexion (21.20 sd 11.49, surgical group; 30.29 sd 8.22, non-surgical group; p = 0.00003). When the patient group was subdivided into clubfoot and idiopathic toe-walkers, significant differences were seen between groups on hindfoot deviation (6.34 sd 5.54, clubfoot group; 3.21 sd 1.47; idiopathic toe-walker group; p = 0.004) and plantar flexion (21.60 sd 11.38, clubfoot group; 32.11 sd 8.87, idiopathic toe-walker group; p = 0.002). No significant differences were seen between patients in the clubfoot group and patients in the other group (tarsal coalition idiopathic flatfoot, others) (Table 2).
Aetiology of the foot problems in patients
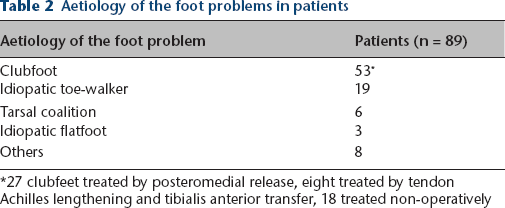
27 clubfeet treated by posteromedial release, eight treated by tendon Achilles lengthening and tibialis anterior transfer, 18 treated non-operatively
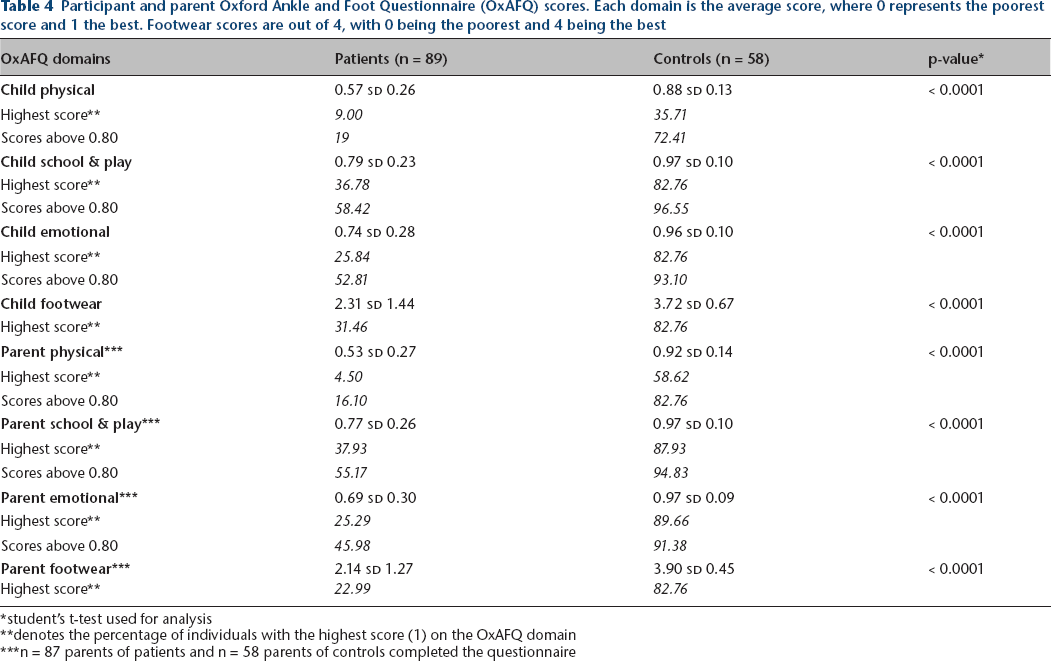
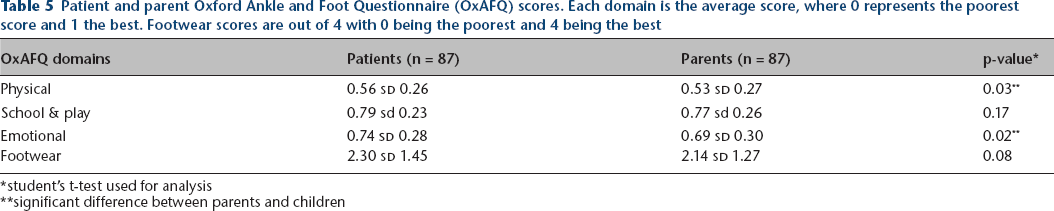
Patients and controls scored significantly differently on all foot measurements; 44% of patients had normal foot measurements (Table 3). Patients and controls scored significantly differently (p < 0.0001) on all domains (i.e. physical, emotional, school & play) and on the item footwear of the OxAFQ (Table 4). Scores of 1 (highest possible score) on the OxAFQ were more likely in controls and their parents. About 35.71% to 87.93% of controls and their parents’ ratings were the highest score. In the group of patients and their parents, highest scores ranged between 4.5% and 37.93% of participants. Parents of patients compared with parents of controls scored significantly different (p < 0.0001) in all domains (i.e. physical, emotional, school & play) and on the item footwear of the OxAFQ (Table 4). Patients and their parents significantly differed on the physical domain (p = 0.03) and the emotional domain of the OxAFQ, with parents’ ratings reflecting lower scores and poorer outcomes (Table 5).
Foot measurements

student's t-test used for analysis
Participant and parent Oxford Ankle and Foot Questionnaire (OxAFQ) scores. Each domain is the average score, where 0 represents the poorest score and 1 the best. Footwear scores are out of 4, with 0 being the poorest and 4 being the best
student's t-test used for analysis
denotes the percentage of individuals with the highest score (1) on the OxAFQ domain
n = 87 parents of patients and n = 58 parents of controls completed the questionnaire
Patient and parent Oxford Ankle and Foot Questionnaire (OxAFQ) scores. Each domain is the average score, where 0 represents the poorest score and 1 the best. Footwear scores are out of 4 with 0 being the poorest and 4 being the best
student's t-test used for analysis
significant difference between parents and children
When examining correlations between function, as determined by the OxAFQ and foot characteristics (i.e. plantar flexion, dorsiflexion, foot ROM arc, hindfoot deviation), moderate correlations were found between child report on the OxAFQ physical domain and foot ROM arc (r = 0.56; p < 0.001) Strong correlations were found between parent report on the OxAFQ physical domain and foot dorsiflexion with the knee flexed (r = 0.54; p < 0.001) and also between the OxAFQ physical domain and foot ROM arc (r = 0.59; p < 0.001). There was also a strong correlation between OxAFQ parent report on footwear and foot ROM arc (r = 0.53; p < 0.001). Most of the OxAFQ domains reported by children and parents showed weak to moderate correlations with foot measurements with the exception of the child's and parent's report on the school & play domain with hindfoot deviation, which was not significant (Table 6).
Correlations between function (as determined by Oxford Ankle and Foot Questionnaire (OxAFQ)) and foot characteristics for patients and controls
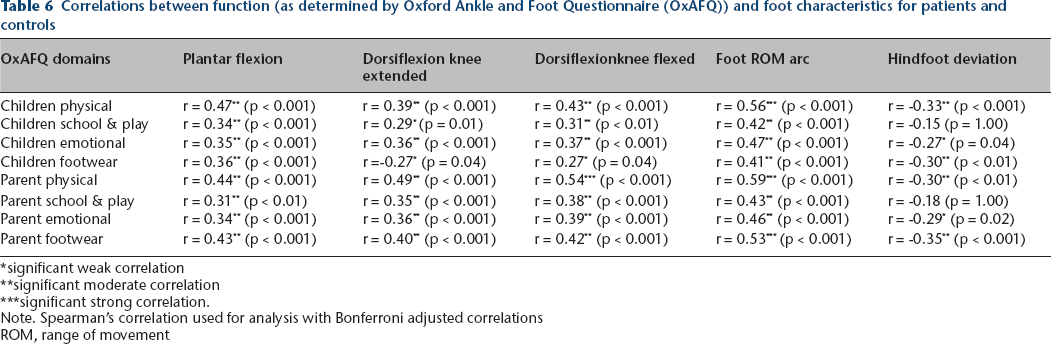
significant weak correlation
significant moderate correlation
significant strong correlation.
Note. Spearman's correlation used for analysis with Bonferroni adjusted correlations
ROM, range of movement
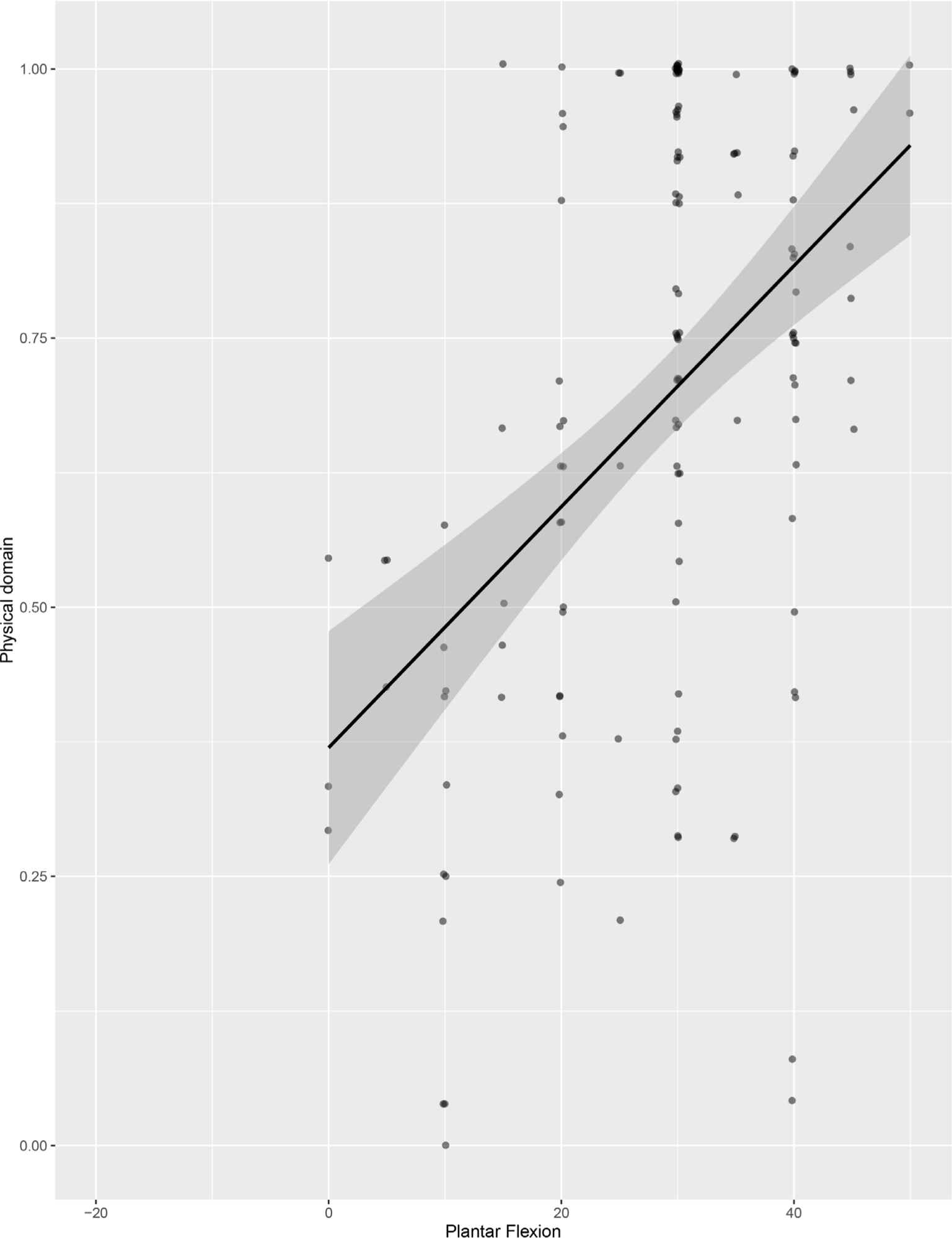
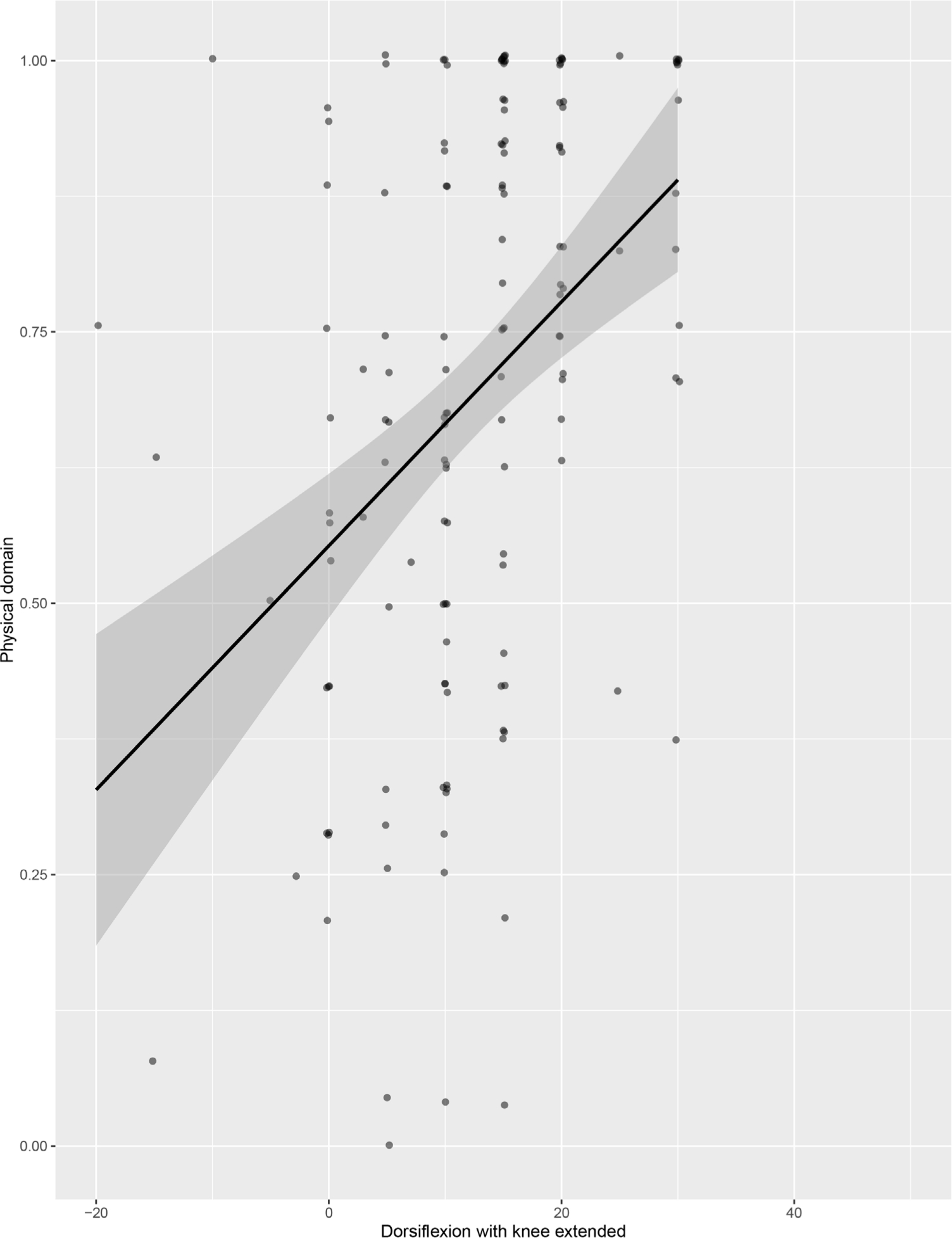
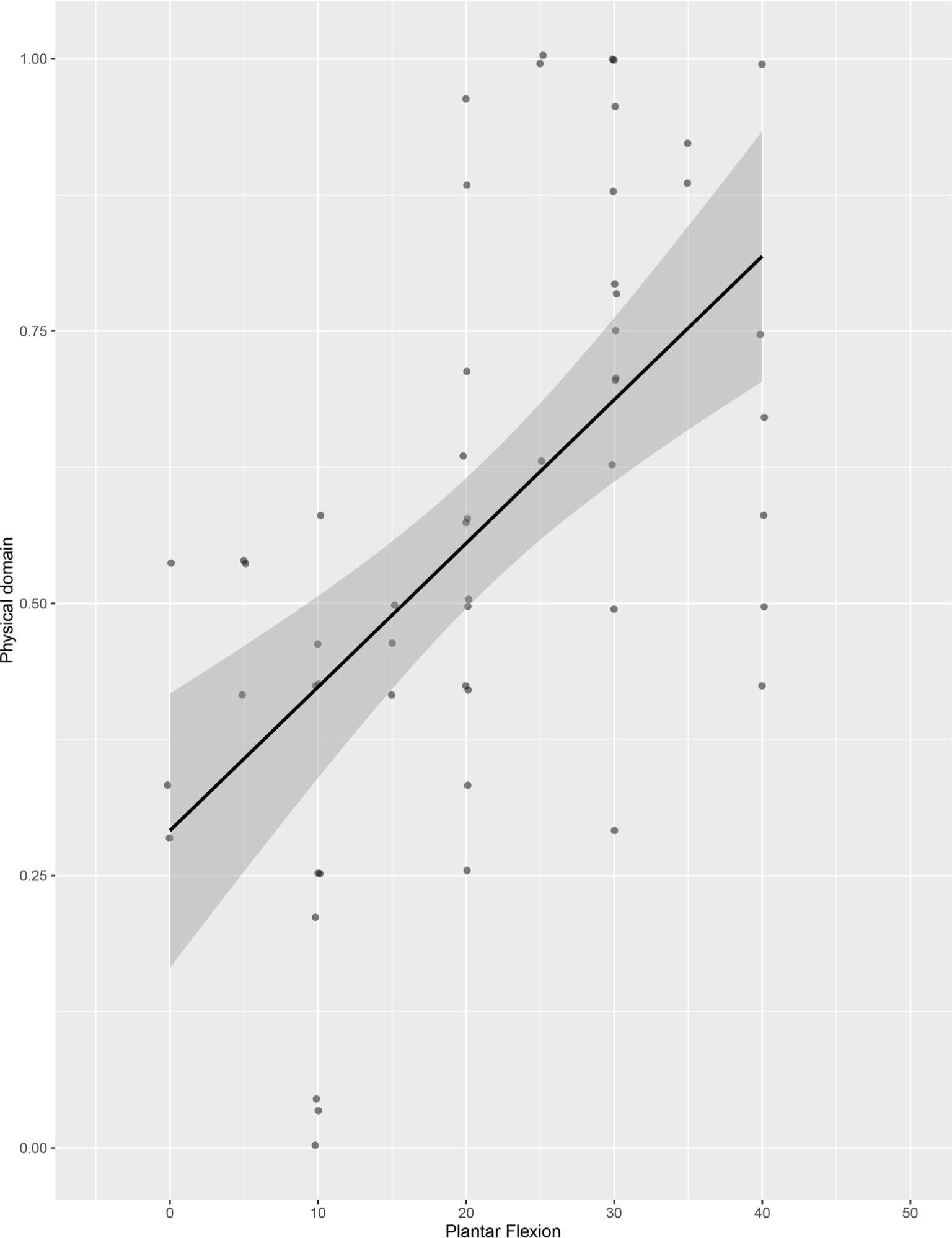
When examining the physical domain on the OxAFQ as reported by children, positive moderate correlations were seen with: greater plantar flexion (r = 0.47; p < 0.001) (Fig. 1), dorsiflexion when having the knee extended (r = 0.39; p < 0.001) (Fig. 2) and dorsiflexion when having the knee flexed (r = 0.43; p < 0.001) (Fig. 3). The OxAFQ's physical domain reported by children showed a negative moderate correlation with hindfoot deviation (r = -0.33; p < 0.001) (Fig. 4). Further examination of the relationship between reported physical domain on the OxAFQ and hindfoot deviation revealed a significant negative moderate correlation between physical domain scores and increased valgus (r = -0.35; p < 0.0001) only (Fig. 5). Figure 6 provides an example of foot structure and measurements and ratings on the OxAFQ by both patient and parent.
Correlation between plantar flexion and physical domain of Oxford Ankle and Foot Questionnaire (r = 0.47; p < 0.001; includes patients and controls, excludes parent report).
Correlation between dorsiflexion-knee extended and physical domain of Oxford Ankle and Foot Questionnaire (r = 0.39; p < 0.001; includes patients and controls; excludes parent report).
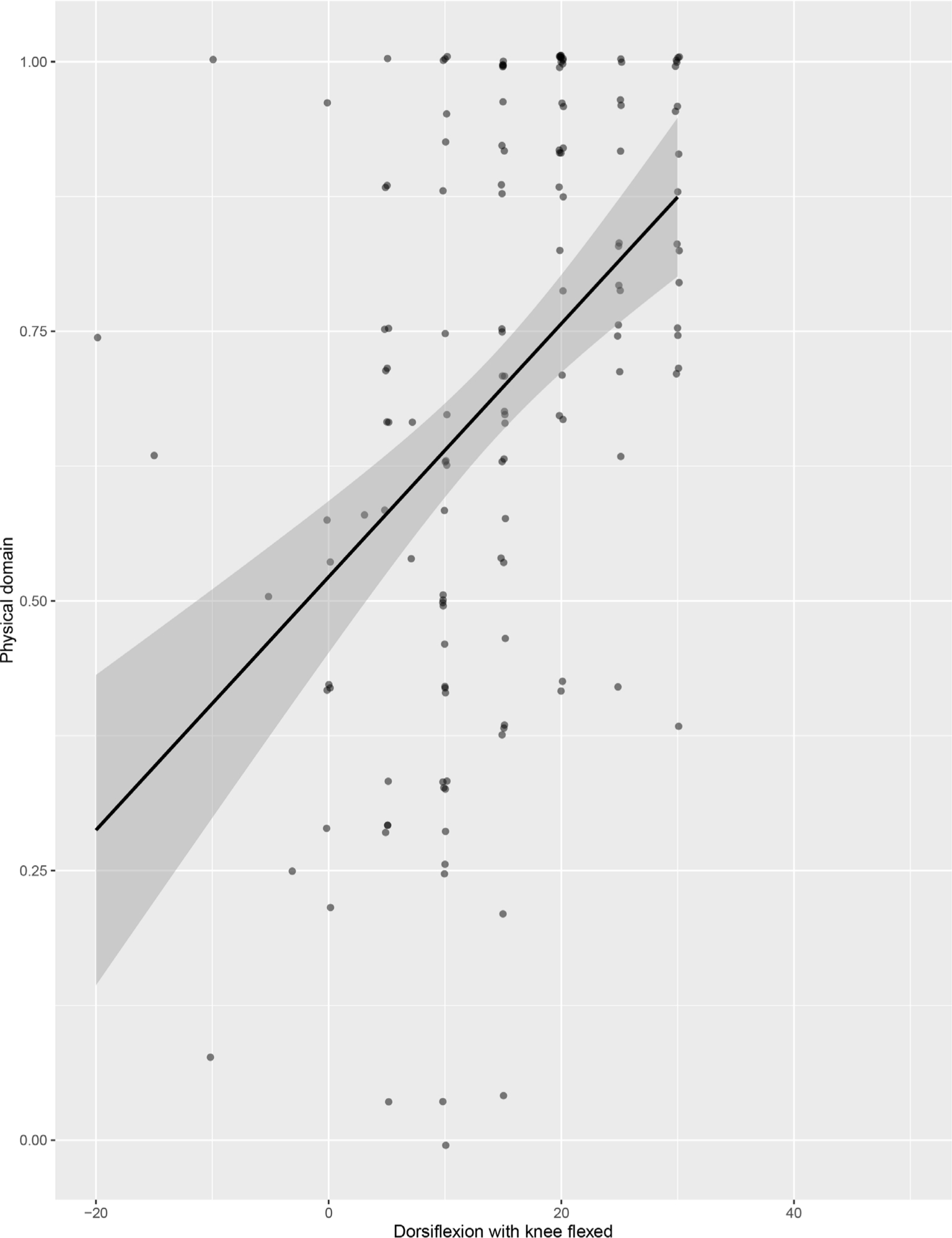
Correlation between dorsiflexion-knee flexed and physical domain of Oxford Ankle and Foot Questionnaire (r = 0.43; p < 0.001; includes patients and controls; excludes parent report).

Correlation between hindfoot deviation and physical domain of Oxford Ankle and Foot Questionnaire (r = -0.33; p < 0.001; includes patients and controls; excludes parent report).
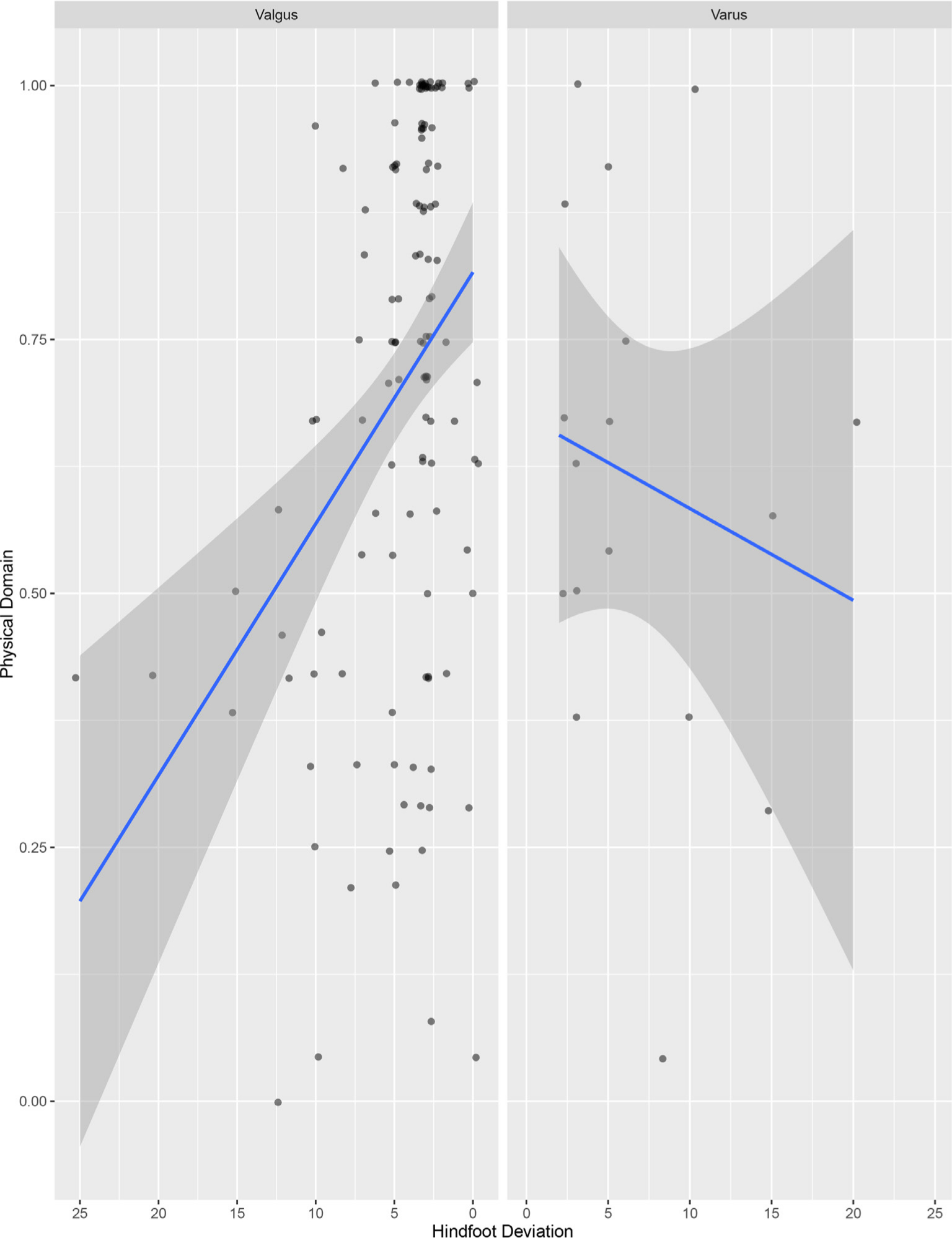
Comparing hindfoot deviation and physical domain (Oxford Ankle and Foot Questionnaire), separated by valgus and varus (valgus r = -0.35; p < 0.0001; varus r = -0.19; p = 0.47; includes patients and controls; excludes parent report).

Examples of foot structure and rating on the Oxford Ankle and Foot Questionnaire (OxAFQ) by both patient and parent. Examples of foot structure and rating on the OxAFQ by both patient and parent. This 15-year-old male patient had bilateral clubfeet and underwent two posteromedial releases on the left foot and one posteromedial release on the right foot. On the left foot, he had 25° hindfoot deviation, 0° dorsiflexion knee-flexed and knee-extended and 20° plantar flexion. A higher score on the OxAFQ domain represents better functioning (0 to 1.00) Footwear is reported as a single item. Items are scored from 4 (never) to 0 (always) indicating how frequently the issue effects the child. Patient rating on the OxAFQ included: physical domain = 0.42; school & play domain = 1.00; emotional domain = 0.69; footwear = 2.00. Parent rating on the OxAFQ included: physical domain = 0.50; school & play domain = 0.88; emotional domain = 0.38; footwear = 1.00.
Correlations between function, as determined by the OxAFQ and foot characteristics (i.e. plantar flexion, dorsiflexion, foot arc-of-movement, hindfoot deviation) were completed individually for the control group, as well as for patients, with these being further analyzed according to the type of treatment received: patient surgical group and patient non-surgical group. In terms of the control and the patient non-surgical groups, no significant correlations were found in either of these groups. In terms of the patient surgical group, positive moderate correlations were found between physical domain of the OxAFQ as reported by children and plantar flexion (r = 0.57; p = 0.0002) and foot arc-of-movement (r = 0.57; p = 0.0003) (Figs 7 and 8, respectively); as well as positive moderate correlations between the emotional domain of the OxAFQ as reported by children and plantar flexion (r = 0.48; p = 0.01) and foot arc-of-movement (r = 0.45; p = 0.02); and lastly positive moderate correlations were found between the physical domain of the OxAFQ as reported by parents and plantar flexion (r = 0.47; p = 0.02), and foot arc-of-movement (r = 0.45; p = 0.02). In terms of the patient clubfoot group, positive moderate correlations were found between physical domain of the OxAFQ as reported by children and plantar flexion (r = 0.54; p = 0.001) and foot arc-of-movement (r = 0.53; p = 0.002); as well as positive moderate correlations between the emotional domain of the OxAFQ as reported by children and foot arc-of-movement (r = 0.53; p = 0.04). In terms of the patient group of idiopathic toe-walkers, significant moderate to strong correlations were found across all domains of the OxAFQ as reported by parents and foot arc-of-movement: physical domain and foot arc-of-movement (r = 0.71; p = 0.02), school & play domain and foot arc-of-movement (r = 0.72; p = 0.02), emotion domain and foot arc-of-movement (r = 0.59; p = 0.02) and foot domain and foot arc-of-movement (r = 0.71; p = 0.02).
Correlation between plantar flexion and physical domain of Oxford Ankle and Foot Questionnaire for patients in surgical subgroup (r = 0.57; p = 0.0002; for patient surgical subgroup only).
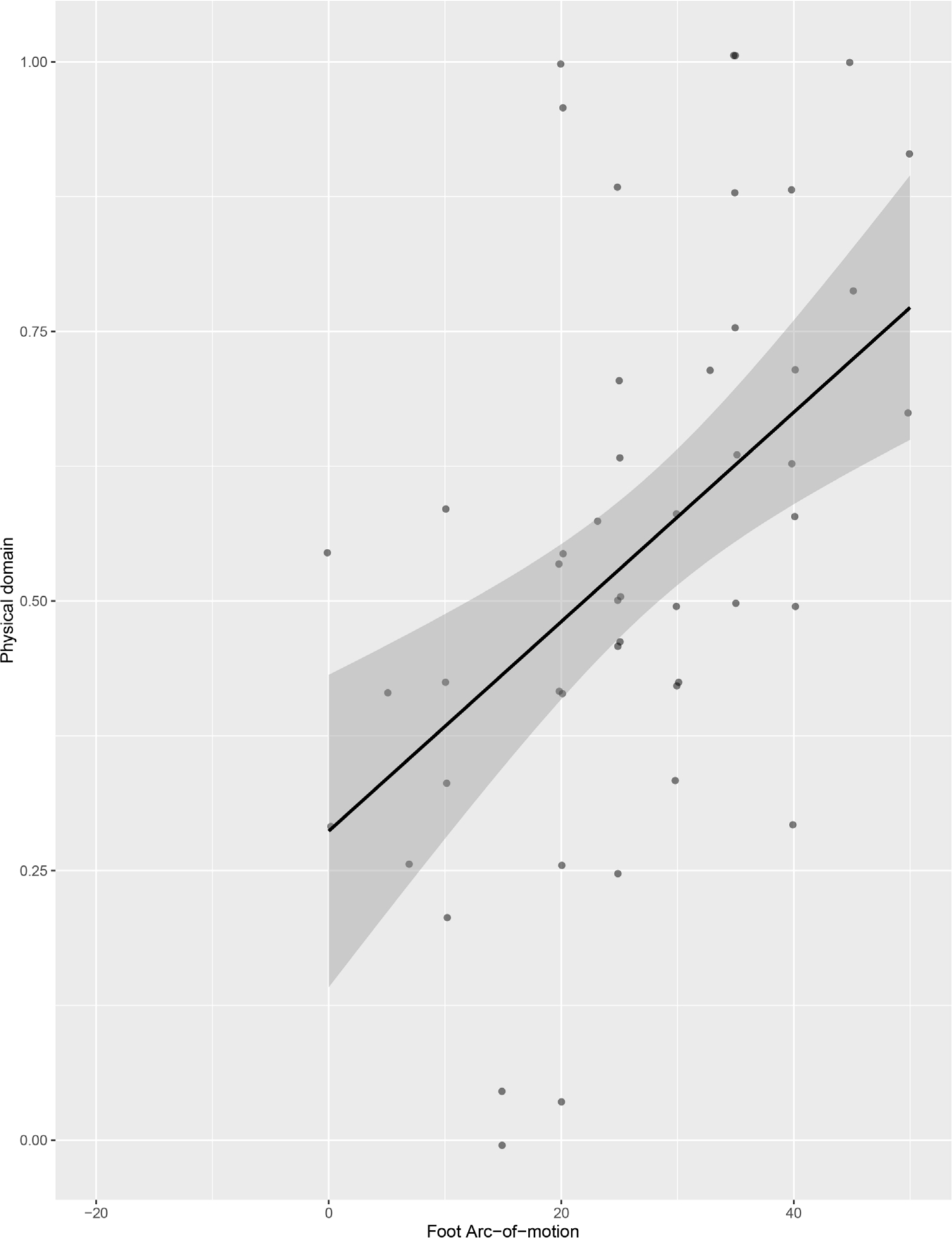
Correlation between foot arc-of-movement and physical domain of Oxford Ankle and Foot Questionnaire for patients in surgical subgroup (r = 0.57; p = 0.0003; for patient surgical subgroup only).
Discussion
Our study has demonstrated that shape and movement show substantial variability in their relationship to function. Plantar flexion and foot arc-of-movement moderately correlated with physical foot function as reported by children and by their parents on the OxAFQ physical domain. Despite the focus of surgeons on achieving dorsiflexion in treatment of foot problems, our study highlights that lack of plantar flexion had similar or stronger association with function.
According to the International Classification of Functioning, Disability and Health, formally endorsed by the World Health Organization in 2001, functioning is a continuum, relevant to the lives of all people to different degrees at different times in their lives. Decrease in functioning may result from decrease in intrinsic capacity, problems with body structures or functions or features of the person's physical, human-built or social environment that lead to problems in performance and decreased capacity. 19 The challenge for surgeons is understanding which structures impair function, which structures are amenable to surgical correction and which structures, if corrected, are likely to lead to improved function.
The relation between foot morphology and function in children is critical to surgeons in planning operative treatment. While surgery can change shape or movement, clearly the primary aim is to relieve symptoms and/or improve function. As expected, no single aspect of foot morphology was highly correlated with function. Irrespective of foot morphology, pain, for example, caused decreased function. The findings of this study are useful to surgeons examining the importance of plantar flexion and dorsiflexion in foot function. While it cannot be determined from this study, perhaps greater attention should be directed to strategies to enhance or preserve plantar flexion and/or ensure that treatments such as surgery do not sacrifice plantar flexion to achieve increased dorsiflexion. Despite our hypothesis, children and parents reported virtually identical scores for the school & play and footwear domains of OxAFQ. This finding is helpful to surgeons who can, in both research and clinical care, rely on parents to accurately reflect on their child's functioning at school. However, children and their parents significantly differed on the physical domain and on the emotional domain of the OxAFQ, with parents’ ratings reflecting lower scores and poorer outcomes. Parents may be more sensitive to their child's functioning and quality of life because they are able to observe their child directly and examine the impact the foot morphology has on their life.
Our study had several strengths. First, the wide variety of foot problems and different foot deformities contributes to the generalizability of the findings of this study. Second, the normal controls, without any foot problems, allowed us to more strongly contrast the relationship of foot deformity to the OxAFQ.
However, this study had several potential limitations. First, hindfoot position is difficult to quantify. To address this, all measurements were performed by a single observer in a consistent fashion who was blind to the questionnaire scores. 20 Although the single observer may concern some researchers, it has been shown that intrarater reliability of hindfoot alignment is good to excellent, and better than interrater reliability. 21 Second, we did not evaluate muscle strength or perform gait analysis. Although it has been demonstrated that foot muscle strength can improve pain and improve function in patients with flatfoot, our primary focus was on ROM and deformity, and our primary outcome, consistent with the aims of surgery, was on function. 22 Fourth, while moderate correlations were found between foot morphology and function, the scatterplots revealed wide variation in the relationships. Fifth, association does not mean cause and effect.
In a cross-sectional study including 245 healthy children, aged seven to 14 years, a wide range of ankle movement was found: passive dorsiflexion with the knee extended was 10° to 43°, passive dorsiflexion with knee flexed was 23° to 57° and maximum plantar flexion was 36° to 70°. 23 One could expect that a healthy child with a minimum of 10° of dorsiflexion and 36° of plantar flexion will have a normal function, but we could not find further data in the literature correlating ROM with function. Although we are not able to define a target ankle movement to achieve the best function, the results of our study highlight the potential importance of plantar flexion in function.
Conclusion
The present study improves our understanding on how morphology and ROM of the foot affect children's functioning. Future research should evaluate how interventions to change foot morphology, or ROM, translate in terms of function as perceived by children and families.
Footnotes
ML: Analysis and interpretation of the data, Drafting and critical revision of manuscript.
GAT: Design, analysis and interpretation of the data, Drafting and critical revision of manuscript.
JD: Data acquisition, drafting and critical revision of manuscript.
UGN: Design, drafting and critical revision of manuscript.
BMF: Design, drafting and critical revision of manuscript.
JGW: Design, analysis and interpretation of the data, Drafting and critical revision of manuscript.