
Abstract
For many people assistive products are important to perform daily activities and to participate in society. In the process of selecting the proper assistive product for a person, it is important to describe in a uniform and transparent way his/her present functioning and wishes with respect to functioning. To indicate how the ICF (the International Classification of Functioning, Disability and Health) can be used during the supply process, we have taken as a framework a general guideline describing this process. The guideline distinguishes seven steps in the supply process and for each step an inventory is made of the actions of the client, the actions of the care professional, the instruments used, the decisions made, the data generated, relevant classifications (including the ICF) to code these data, and the results for the client. It is the aim of this discussion paper to describe the role of the ICF in the prescription and supply of assistive products and to discuss the specific data in this process that can be classified using the ICF. Although the ICF is not perfect, it is a useful tool to code important data in the process of supplying assistive products.
Assistive products – used worldwide by millions of people – are used to maintain or enhance functioning, rather than to cure a disease. 1 As functioning can be classified with the International Classification of Functioning, Disability and Health (ICF), it can be expected that the use of ICF terminology in the supply process of assistive products will result in a better match between the characteristics of the person and the characteristics of the assistive product.
Introduction
For many people, assistive products are important to perform daily activities and to participate in society. In the process of selecting the proper assistive product for a person, it is important to describe in a uniform and transparent way their present functioning and wishes with respect to functioning. To indicate how the ICF (the International Classification of Functioning, Disability and Health 2 ) can be used during the supply process, we have taken as a framework a general guideline 3 describing this process. The guideline distinguishes seven steps in the supply process and for each step an inventory is made of the actions of the client, the actions of the care professional, the instruments used, the decisions made, the data generated, relevant classifications (including the ICF) to code these data, and the results for the client. It is the aim of this discussion paper to describe the role of the ICF in the prescription and supply of assistive products and to discuss the specific data in this process that can be classified using the ICF. Although the ICF is not perfect, it is a useful tool to code important data in the process of supplying assistive products.
Assistive products
There are many products that can help people with disability to enhance their quality of life. Examples are hearing aids, wheelchairs, Braille equipment, communication devices, software, urine collection systems, oxygen apparatus and mobile hoists. Some of these assistive products reduce impairments or compensate for impairments, such as aspirators or stimulators for pain relief. Other products help people to perform an activity (like canes and adapted computers) or to take over an activity (such as elevators) and to participate in society (e.g. adapted cars). Generally speaking, assistive products help people with disability to function better in daily life and to participate in society. 4
There are many models and instruments for the selection and advisory process of assistive products in the rehabilitation field. In 2009, Bernd et al. reviewed the scientific literature; they found seven models and 15 instruments. 5 Of the seven models, three are specific for assistive products and suitable for the selection process: the Matching Person and Technology Model (MPT), 6 the framework for Modeling the Selection of Assistive Technology Devices, 7 and the Human Activity Assistive Technology (HAAT) Model. 8
Use of the ICF
The use of the ICF as a framework for the selection of assistive products is debated in the literature. 5 Many authors stress the importance of the ICF, but there are also authors who are of the opinion that the ICF is not a suitable framework because it fails to meet the needs of the consumers, 9 or because there is a lack of causal and temporal components. 10
The aim of this paper is to discuss how the ICF can be partially used to classify relevant data in the process of supplying assistive products. As a framework for this discussion a general guideline for the supply process of assistive products, developed in the Netherlands, is used.
General guideline
Stimulated by both a change in financing the provision of assistive products in the Dutch healthcare system as well as a shift from care guided by the medical diagnosis to care guided by the (problems in) functioning of the client (as classified with the ICF), a basic guideline was developed to help clients and caregivers to make the right choices in the selection process of assistive products. The guideline was published in February 2010. 2
The basic guideline follows the steps described earlier
11
for the provision of assistive products; the process starts with a person realizing that they have a problem and ends when, during the evaluation, it becomes clear that the person has a properly working assistive product (Figure 1). The steps are described in Table 1.
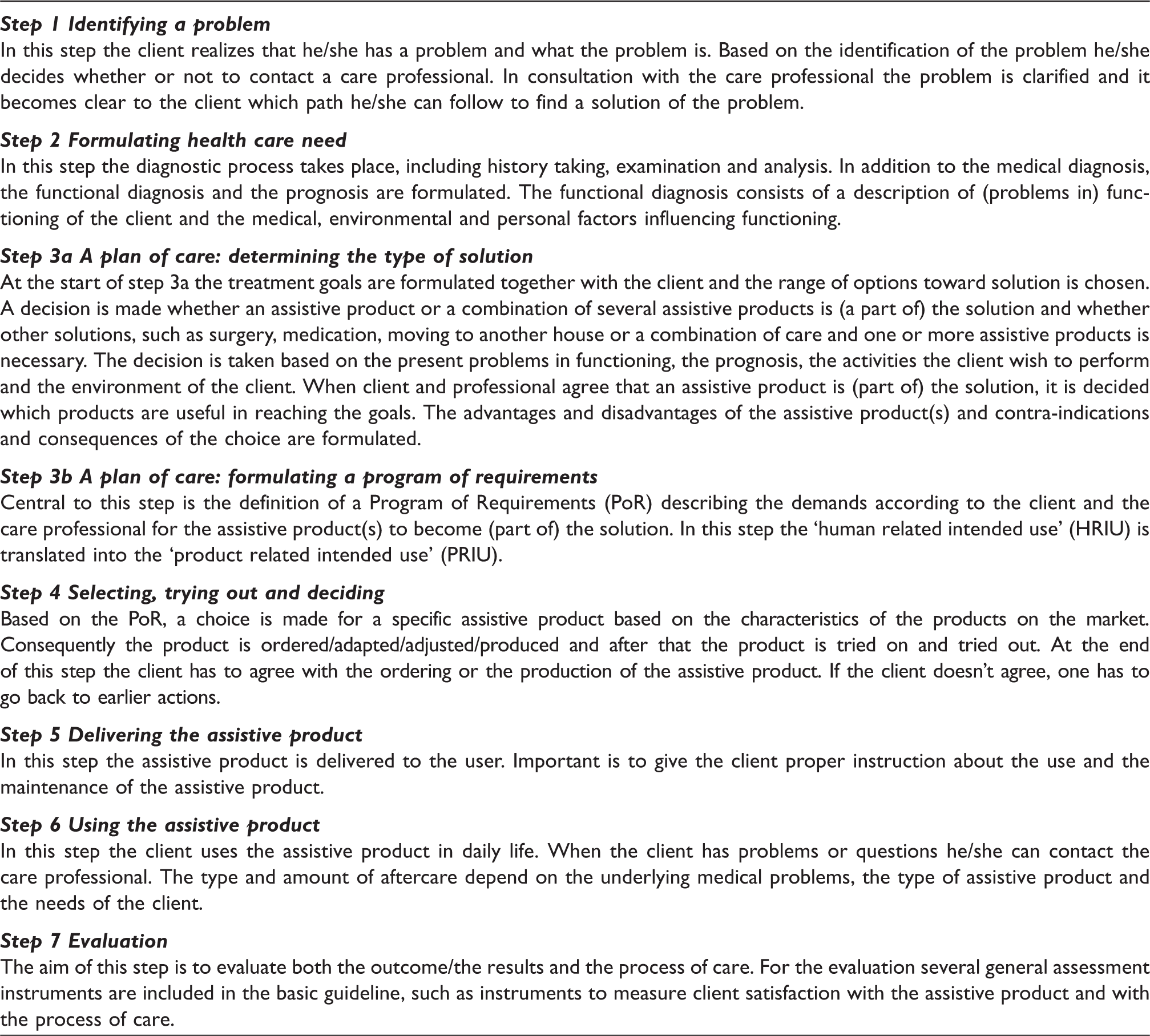
The steps taken in the provision of assistive products. The steps of the general guideline describing the process of supplying assistive products.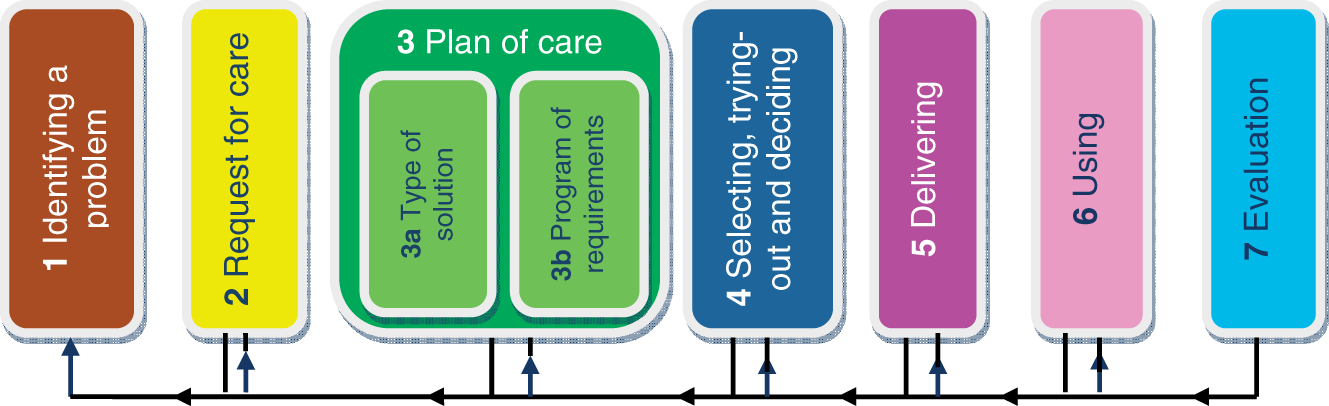
For each step the following items are described:
actions of the client system (the client system consists of the client themselves and, if relevant, other people, such as parents, a partner, and a legal representative); actions of the care professional (such as a health professional (e.g. physician or an occupational therapist), or a producer or supplier of assistive products); sources (such as legislation) and/or assessment or evaluation instruments used; decisions of the client system and/or care professional; data which are generated during the actions and which can be included in the healthcare record; the results for the client system.
Coding assistive products
The ISO 9999 and the Cliq classification.
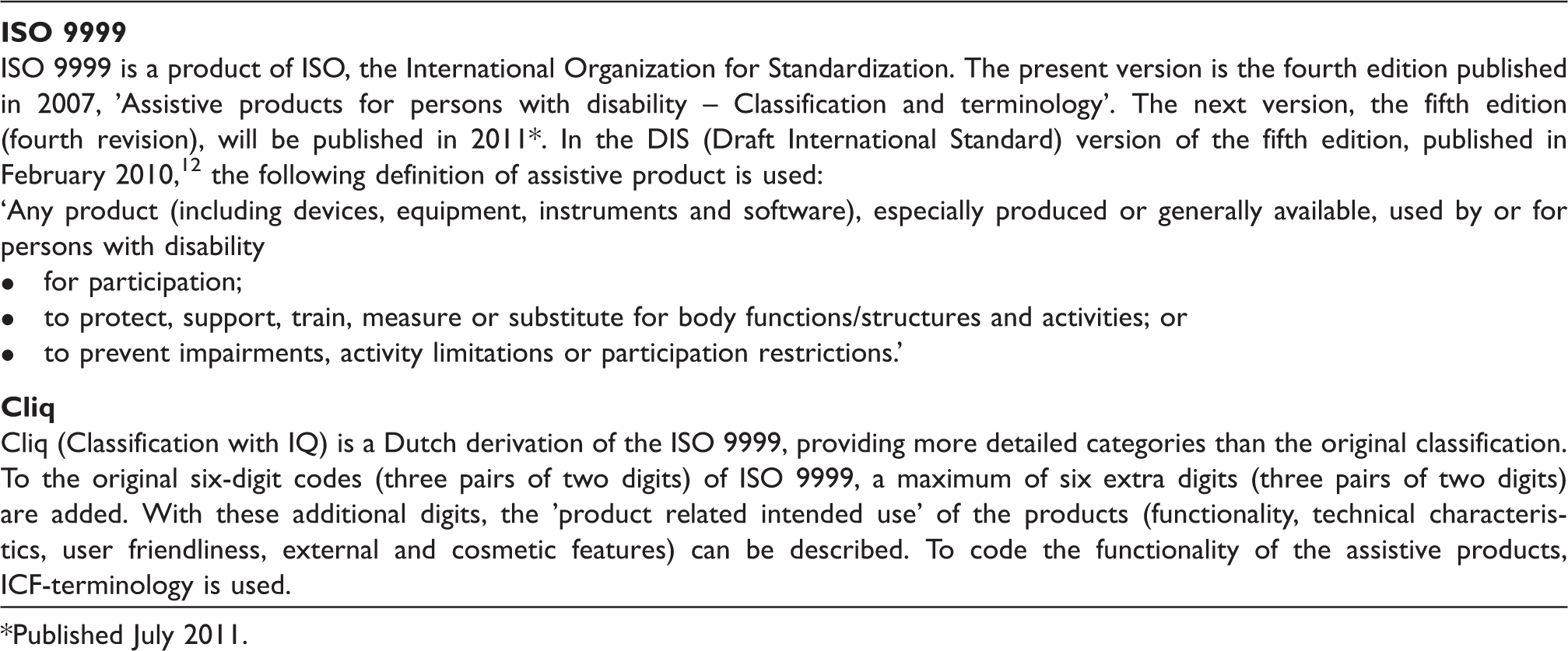
Published July 2011.
Use of ICF and Cliq within the framework of the basic guideline
In this section, the most relevant data generated during the seven steps of the supply process (Figure 1 and Table 1) are described in more detail.
Request for help (step 1)
At the start of the process a multitude of reasons to contact a care professional is possible: problems on the level of body functions and structure (impairment in attention, pain, shortness of breath), activities (such as limitations in walking or communicating), participation (problems in work or in following education) or environmental factors (such as finding a proper assistive product or support of employer). These problems can be classified with the ICF.
Data gathered during history taking (step 2)
In history taking the care professional makes an entry of current (problems in) functioning (complaints) as indicated by the client, their wishes with respect to functioning, the client’s expectations with respect to functioning and the personal circumstances (such as living status, housing, work). All these data can be coded with the ICF.
Findings of care professional (step 2)
Based on a (physical) examination and several tests, a care professional can code their findings with respect to the present functioning of the client with the ICF.
Functional diagnosis (step 2)
In addition to the medical diagnosis, a care professional formulates a functional diagnosis at the end of the diagnostic process: their professional opinion about the functioning of the client and the (positive or negative) influence of medical, environmental and personal factors. With the exception of the medical and personal factors, the functional diagnosis can be coded with the ICF. The medical diagnosis and the medical factors can be classified with a ‘medical’ classification, like the ICD-10, 13 the ICPC 14 or the DSM-IV. 15
General treatment goals (step 3a)
Goals for the treatment as a whole, including the use of assistive products, can be coded using the ICF. General goals are, for example, participation in work, independence in self-care or improving quality of life.
The human-related intended use (HRIU) (step 3a)
HRIU is the ‘intended use of the assistive product from the perspective of the user’; it indicates what the product should make possible or what the product has to do in the eyes of the user. In other words, HRIU is what a client wants, can and may do with the assistive product. ‘Wants’ is about the wishes of the client (I want to read the newspaper using this assistive product, I want to go to the toilet by myself). ‘Can’ is about the possibilities of the client (taking into account the clients’ problems) and ‘may’ indicates what is sensible from the perspective of the care professional. The HRIU can be coded with the ICF.
The product-related intended use (PRIU) (step 3b)
‘Product-related intended use' is a legal term that indicates ‘what the user can and may expect of the assistive product’. It encompasses the following characteristics of the product:
functionality: activities (indirectly participation) for which the assistive product can be used (such as standing and work) and functions and structures supported by the product (such as respiration and range of motion of a joint); technical characteristics; user friendliness; external and cosmetic features (like color); other characteristics.
The PRIU can be coded with the Cliq-classification (Table 2).
Experiences during use (step 6)
The experiences of the client in using the assistive products, including problems in using the assistive products, can be coded with the ICF.
Outcomes/results (step 7)
The results, in terms of changes in functioning of the client, and the goals reached can be classified using the ICF.
To summarize the results, the most important data in the selection and advisory process of assistive products – the functional diagnosis (formulated in step 2), the treatment goals (step 4), the HRIU (step 3) and the results (step 7) – can be coded using the ICF as presented in Figure 2. The PRIU and the characteristics of products on the market cannot be coded with the ICF but can be coded using the ISO 9999 or Cliq.
The most important generated data classified with the ICF and with Cliq (a more detailed version of ISO 9999; see Table 1).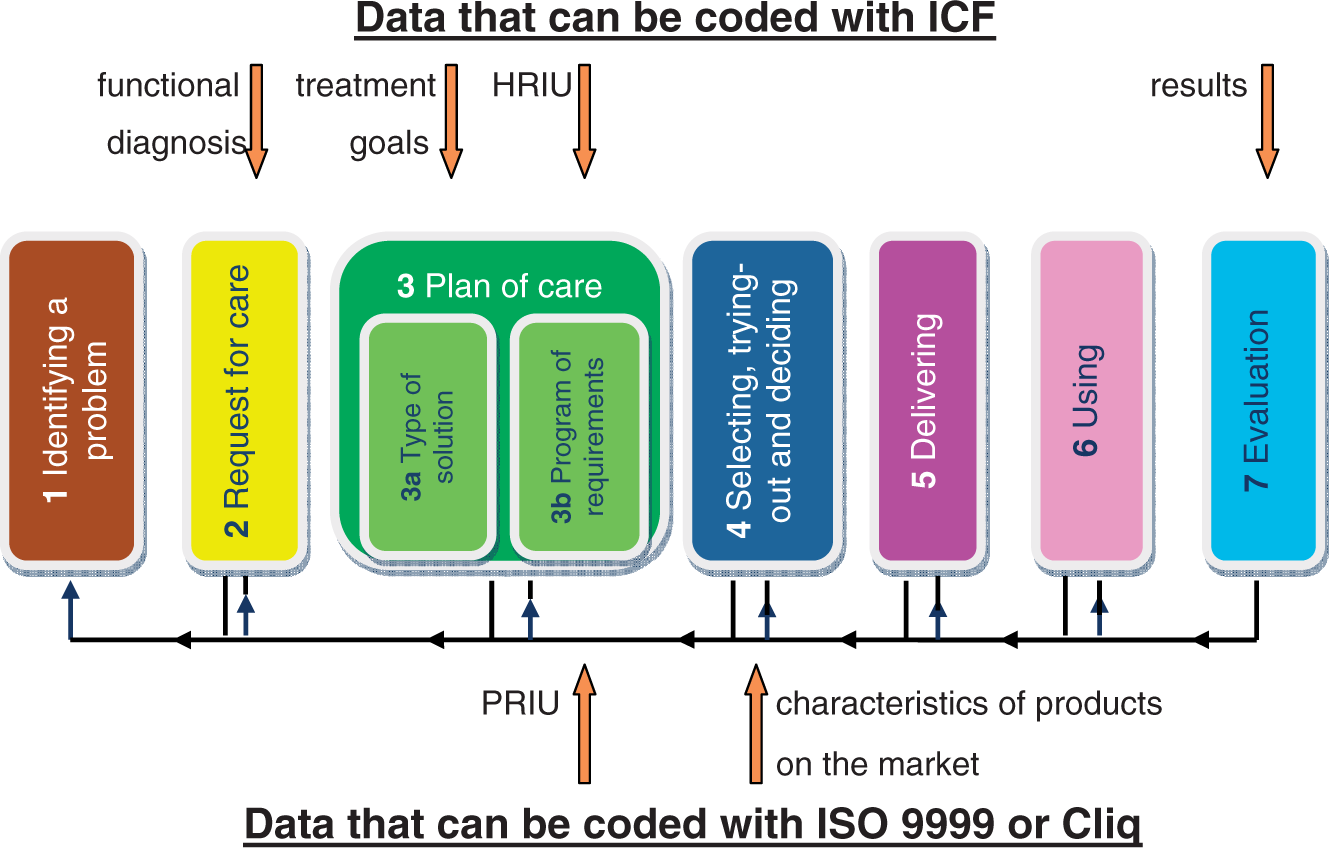
Discussion
As the functioning of the client is the starting point of the provision of assistive products, and clients must be provided with assistive products that help them in their daily functioning, the ICF is an important classification as it can be used to describe both the (problems in) functioning as well as the environmental factors influencing functioning.
To discuss the use of the ICF in the process of providing assistive products, we take the four challenges in using the ICF to quantify assistive technology interventions and outcomes formulated by Smith et al.
9
as our starting point:
The subjective nature of coding while using the ICF, especially the qualifiers to code the severity of the problem.
We agree with Smith et al.
9
that the present qualifier for severity just gives an indication; assessment instruments are needed to decide whether a problem is minor or severe.
Many ICF-codes are not specific enough to describe the function of assistive products.
We agree that this is true for many of the classes of ICF. A solution might be to make a clinical derivative of the ICF including more detailed classes.
The ICF does not consider qualifiers of performance such as safety or task/activity completion time.
There are several attempts to formulate new qualifiers, safety might be such a new qualifier. The time it takes to complete an activity can be integrated in the assessment instruments to code severity.
Problems in matching many of the assistive products with the ICF as it is unclear what the main function of these products is.
As an example for this fourth challenge Smith et al.
9
use a universal cuff: should this be matched to the impairments in functions (such as muscle power), to impairments in structure related to movement or to limitations in activities or restrictions in participation in self-care or employment? In fact this is not a problem of the ICF, but a problem in the ISO 9999. To meet this challenge a document with a mapping of all the subdivisions of the ISO 9999 to the ICF can be found on the website of the Dutch WHO Collaborating Centre.
16
Moreover, attempts are made to harmonize Chapter 1 of the list of environmental factors of the ICF and the ISO 9999.
17
Although we see the current problems of the ICF – such as lack of detail, a combined list of activities and participation, no list of personal factors (which are very important in selecting assistive products) – we think that the ICF is a useful tool on three levels:
on the most abstract level the basic ICF terms (like participation and disability) can be used in, for example, policy documents (such as documents on the reimbursement of assistive products for people with disability); on a more detailed level the titles of the ICF classes can be used to describe characteristics of (groups of) clients, such as in clinical guidelines; to aggregate data of groups of clients ICF-codes can be used, such as in electronic healthcare records and in epidemiological research.
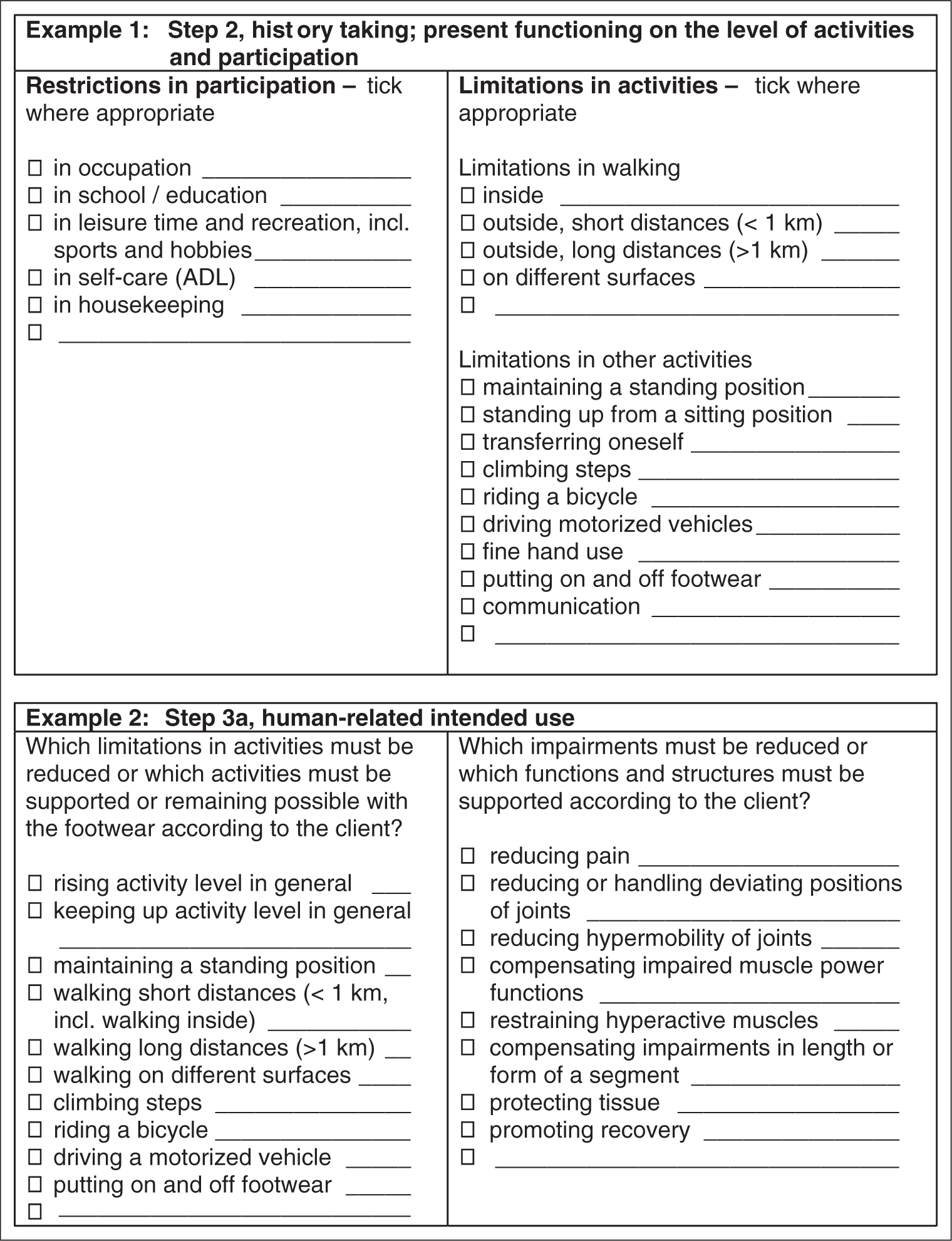
With the use of the basic guideline, more specific protocols are developed in 2011, such as a protocol for people with walking problems and a protocol for persons with hearing problems. Already available is a protocol for orthopedic shoe technicians to provide proper footwear to persons referred to them by a physician (persons with more complicated problems). 18 The protocol was published in June 2010. 19
Two examples of data to be classified with the ICF from the Dutch protocol for shoe technicians. 19
The basic guideline has been developed to make the process of supplying assistive products more transparent and to increase the chance that the selected assistive product really helps the individual to function better in daily life and to prevent mismatches as much as possible. However, a period of trying out is necessary as there are so many (objective and subjective) factors which determine whether or not a good match is reached between the characteristics of the client and the characteristics of the assistive product.
Conclusion
Although the ICF is not perfect – it lacks detail and there is no list of personal factors – it can be used to code important data in the process of providing assistive products to clients who have problems in functioning in daily life. These data are the functional diagnosis, the treatment goals, the HRIU, and the results/outcome of the process (changes in functioning due to the use of the assistive product provided). By using the ICF to describe the wishes and possibilities of the clients (HRIU), a better match is possible with the characteristics of the assistive product. Awaiting harmonization of Chapter 1 of the list of environmental factors of the ICF and the ISO 9999, it is advised to use the ISO 9999 or the Cliq classification to describe the characteristics of assistive products.
Footnotes
Funding
The development of the general guideline was funded by the Dutch Ministry of Health, Welfare and Sport.