
Abstract
Background: The International Classification of Functioning, Disability and Health (ICF) covers all aspects and levels of human functioning.
Objectives: The aim of the study was to find out whether the ICF can be used in everyday prosthetics and orthotics (P&O) clinical practice for description of human functioning, and whether it can demonstrate the influence of a prosthesis or an orthosis on a person's functioning.
Study Design: Prospective clinical study.
Methods: A short list of ICF codes was compiled from Annex 9 and used for one month for all patients seen at the author's P&O outpatient clinics.
Results: One hundred patients (59 men, average age 58 years) with different medical problems were included in the study. From 6 to 27 (14 on average) ICF categories from all four components of ICF were used in these patients. The most frequently used category for body functions was mobility of joint functions, for body structures it was structure of the skin and for activities and participation it was walking. Public and private buildings were the only barriers identified.
Conclusions: It can be concluded that the ICF can be used in everyday P&O clinical practice. An ICF list of categories provides quick additional information. To be able to demonstrate the influence of P&O devices on person's functioning, at least for activities and participation, one has to use qualifiers.
For clinicians it is important to know that it is possible to use the ICF in clinical practice and that it can demonstrate the impact of P&O devices on a person's functioning.
Background
At a prosthetics and orthotics (P&O) outpatient clinic, the clinician can see patients with very different diagnoses who have different functional problems, such as people following lower and/or upper limb amputation, other lower/or upper limb impairments, impairments of spine, disabilities due to different neurological or rheumatologic diseases, and others. The patients need different devices, which are not disease or injury specific, but depend on problems with functioning. In Slovenia, as in several other European countries, prostheses and orthoses have to be prescribed by a medical doctor. Thefirst phase of this process is to identify patients’ problems, which are then the basis for goal settings, therapy prescription including prosthesis and orthosisand evaluation of our work.
Presently, there is no uniform way to describe problems of those in need of prostheses and orthoses. Most frequently, we just describe the problems and medical findings in a way we have learned during our training. Sometimes we use outcome measures. At the end of the 20th century, there were around 50 different outcome measures in use across Europe just for people following lower limb amputation. 1 In a literature review, Condie 2 found that 25 different outcome measures are used as primary ones and several more as comparators. There are at least seven outcome measures for adults following upper limb amputation andan additional nine for children. 3 However, the author of this study did not find any outcome measures specific for people with impairments of the spine or specific to people using orthoses. Almost all these outcome measures were developed before the publication of the International Classification of Functioning, Disability and Health (ICF) 4 and most of them do not cover the full spectrum of human functioning.5,6
The main goal of prostheses and orthoses is to improve individual functioning. Prostheses replace an amputated part of the body and try to restore the lost body function and decrease the problems with activities and participation.7–14 Orthoses also influence body functions, such as increased or decreased mobility, pain, decreased muscle strength and so on. 15 The result is improved functioning. The current outcome measures are useful but are not comprehensive and do not fully encapsulate human functioning and activity limitations. 16 Resnik 17 identified 40 generic or condition-specific self-reported measures that have questions from oneor more of the nine activities and participation chapters of the ICF. Only five of them contain participation items linked to all nine chapters of the activity and participation component of the ICF. These five had not been used in people following amputation. Two others (Frenchay Activities index18–20 and Reintegration into Normal Living Index21,22) have been used but, according to Noonan, are not ICF-based. 23
The ICF covers all aspects and levels of human functioning and was developed as a common language. 4 The ICF organizes information in two parts and each has two components. Part one deals with Functioning and Disability (components Body comprises classification for Body functions and classification for Body structures, second component is Activities and Participation), part two covers Contextual Factors with classification of Environmental factors. It is organized in alphanumerical system in which the letter b is used for Body Functions, s for Body Structures, d for Activities and Participation, and e for Environmental Factors. These letters are followed by a numeric code describing category. The first number represents the chapter number (first level), the next two define category on second level and an additional one digit can be added for the third and fourth level. In chapters ICF categories are nested’ so that broader categories are defined to include more subcategories. The ICF categories are only complete with the presence of a qualifier. 4 For Activities and Participation two qualifiers have to be used. The first one for Performance is what an individual does in their current environment, and includes the environmental factors. The second one, Capacity, describes an individual's ability to execute a task or an action in a uniform or standard environment without assistive technologies and/or adaptations. 4
There is still no agreement on how to use ICF in clinical practice. The World Health Organization (WHO) suggested using an ICF checklist or WHO-DAS II questionnaire, which are both pathology non-specific, whereas others are developing pathology specific ICF core sets. 16 There are no published studies on ICF use in P&O clinical practice. Kohler et al. 16 wrote about core set development for people following amputation and two studies linked outcome measures to ICF.5,6 Raggi et al. 24 found the WHO-DAS II, an ICF-based disability instrument to be sensitive to the influence of assistive technology on person's functioning, but none of the included subjects had a prosthesis or orthosis.
Hence, the aim of the present study was to determine whether the ICF can be used in everyday P&O clinical practice for the description of human functioning, and whether it can demonstrate the influence of prostheses and/or orthoses on a person's functioning. Additionally, we wanted to find out if functioning depends on an individual's age and number of P&O devices used.
Methods
A shortlist of ICF categories with appropriate codes was prepared by author from Annex 9 (Suggested ICF data requirements for ideal and minimal health information systems or surveys) 4 based on clinical experience (see supplementary material appendix 1). Six nests (vision, hearing, speech, fertility, breathing, cognition) and three categories (sexual activity, sleep, energy/vitality) from the Annex 9 were not included in the list. Two suggested nests (affect, communication) and all categories from two other suggested nests (mobility, dexterity) were included. From five nests (digestion, bodily excretion, self-care, interpersonal relations, social functioning), some selected categories were included, as well as from the suggested two chapters on usual activities (chapters 6 and 8 of Activities and participation). Code for pain was also included. Because some other categories are usually checked that are not in Annex 9, six additional categories were added for body functions, seven for body structures, three for activities and participation, and three for environmental factors. The final list had seven categories and two nests for body functions, seven categories for body structure, 20 categories and three nests for activities and participation, and three categories for environmental factors. All categories were used at the second level and no qualifiers were used at the beginning, just either zero (meaning that the variable was checked and the patient had no problems) or one (if the patient had problems). For environmental factors +1 means that the environmental factor was facilitator, 0 that it was checked but was neither facilitator nor barrier and -1 that it was a barrier. If during a medical examination additional things relevant for P&O prescription werechecked, categories for new categories ware added later.
Later, it was realised that in order to demonstrate the influence of P&O devices on a person's functioning, qualifiers have to be used for the domain of activities and participation. The qualifiers for capacity and performance were thus added. The basis for selection of a qualifier was the description of the variable in the medical record. Zero means no difficulty (0–4%), 1 mild difficulty (5–24%), 2 moderate difficulty (25–49%), 3severe difficulty (50–95%) and 4 complete difficulty (96–100%). 4
The second part of the list was a list of the P&O devices and mobility aids (wheelchair, walker, crutches, cane) that can be prescribed in the clinic. Additionally, ICDcategories and general data (age, gender) were collected.
The list was used for one month for all patients seen at the author's P&O outpatient clinics and filled in by the author during or immediately after the examination. For each patient, the scores for capacity and performance were computed as the sums of all the corresponding qualifiers used as described by Garin and colleagues. 25
Descriptive statistics (frequencies, minimum, maximum, median, means, standard deviation) and paired t-test for comparison of performance and capacity scores were used.
This study was approved by the Institute's Ethics Committee.
Results
One hundred patients (59 men and 41 women), with anaverage age of 58 years (range from 18 to 95), were included in the study. They had between one and seven(median 1) different ICD codes. Twenty-five had had a lower limb amputation, 17 were polio survivors, 17 had different paresis of lower or upper limb, 12 had hadan upper limb amputation, 12 had suffered a stroke, six hadfoot problems, five had knee or other lower limb problems and three had suffered a traumatic brain injury and combined upper and lower limb amputation.
Number of ICF categories used from different components.
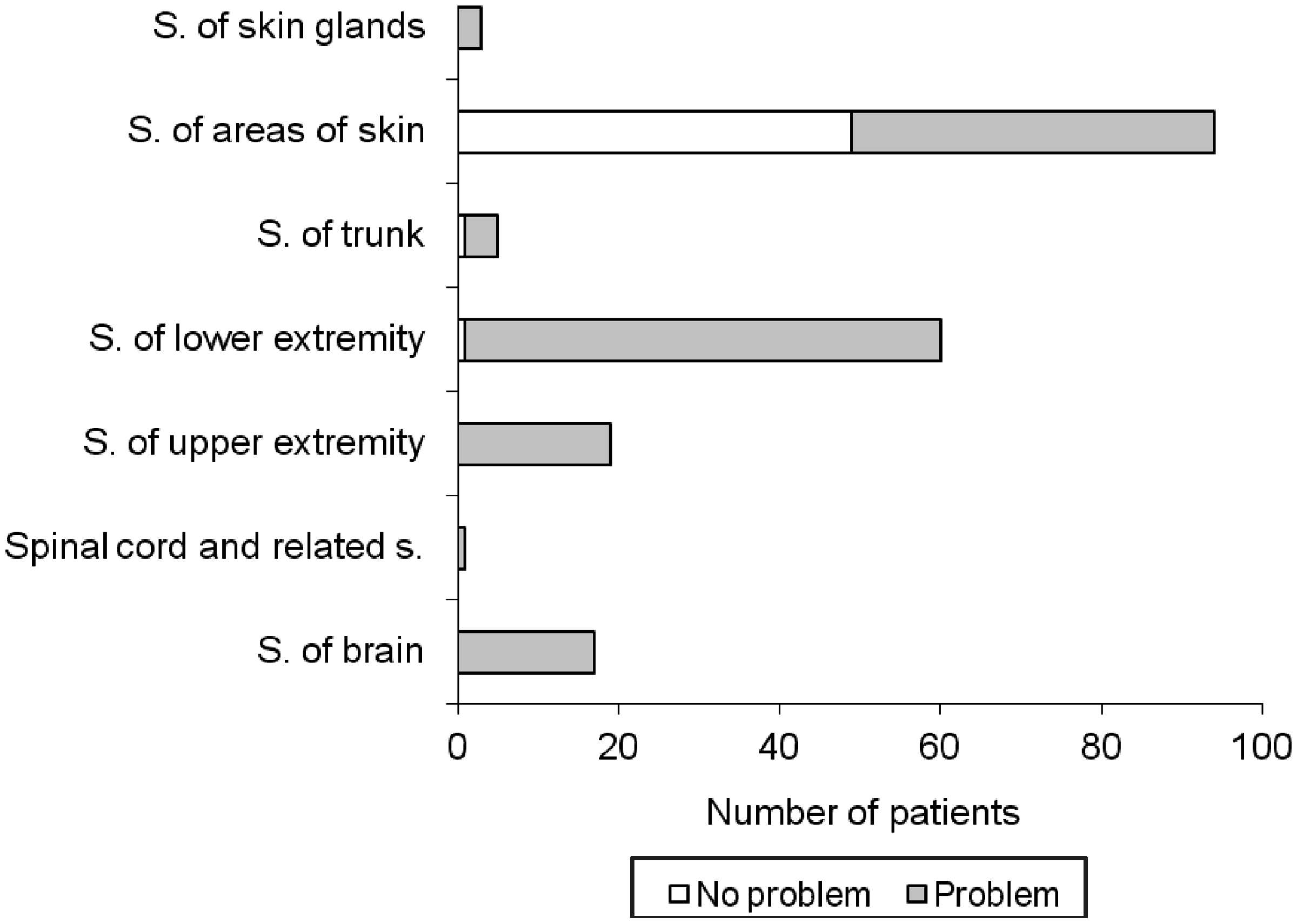
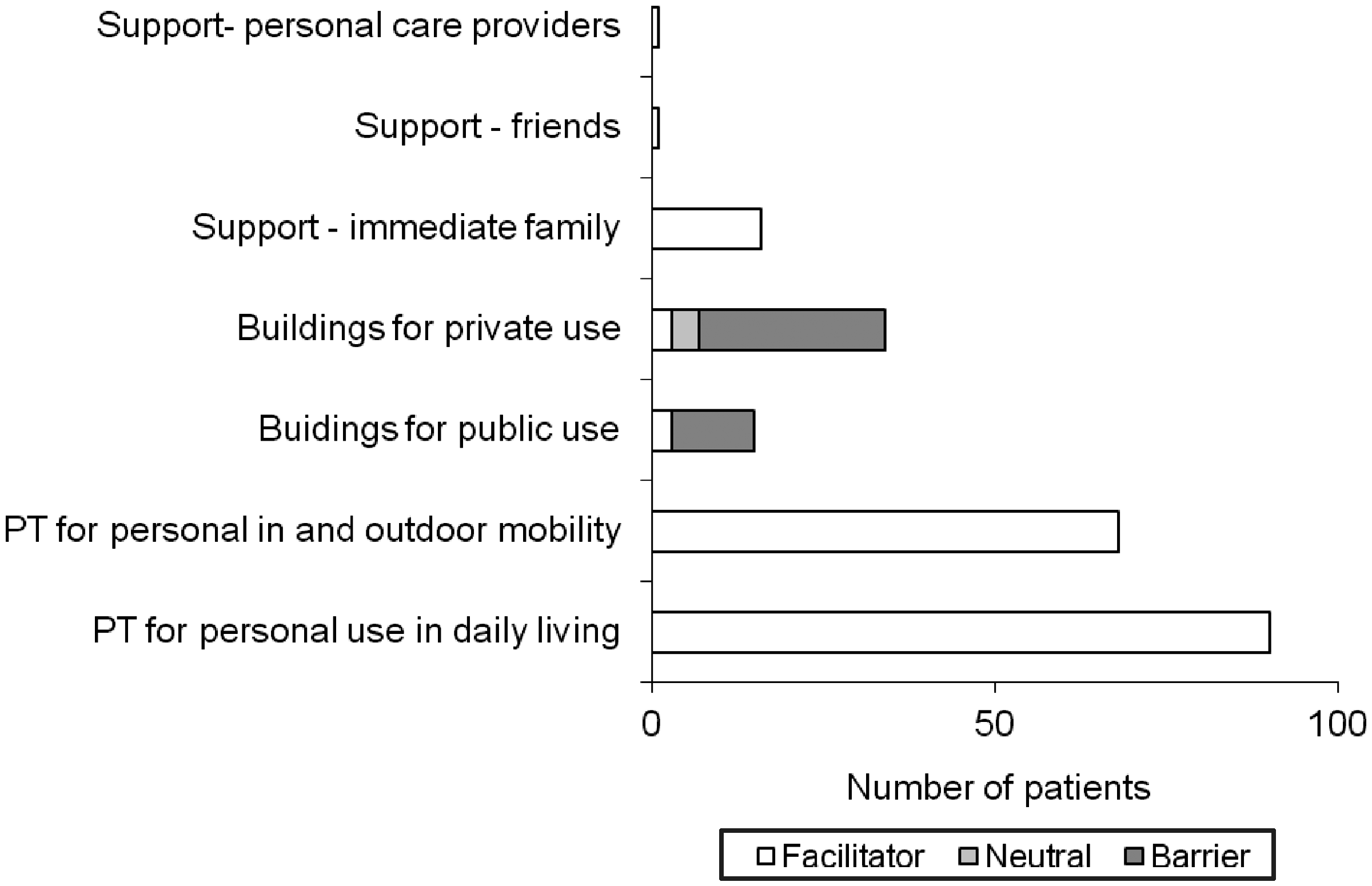
The most frequently used category for body functions was mobility of joint functions (Figure 1) and the most frequently used category for body structures was structure of the skin (Figure 2). Frequency of the checked activities and participation is presented in Figure 3. Products and technology for personal use was the mostfrequent facilitator (Figure 4). Public and private buildings were the only found barriers (Figure 4).
Frequency of used categories for body functions (F., f. – functions) (no problems means that the variable was checked and the patient had no problems, problem means that the patient had problems). Frequency of used categories for body structures (S., s. – structure) (no problems means that the variable was checked and the patient had no problems, problem means that the patient had problems). Percentage of subjects with different functional problems for whom the categories have been used. Frequency of used categories for environmental factors (PT – products and technologies).
It took one to two minutes to fill in the prepared list and up to five further minutes to find the categories for the categories not on the list. To rate the categories using the qualifiers required an additional five to 15 minutes. Performance with the P&O devices was significantly better than capacity (t = −10.393, p < 0.001, Figure 5).
Capacity (ability to do tasks in standardised environment without any assistive devices) and performance (ability to do tasks in their environment and with assistive devices).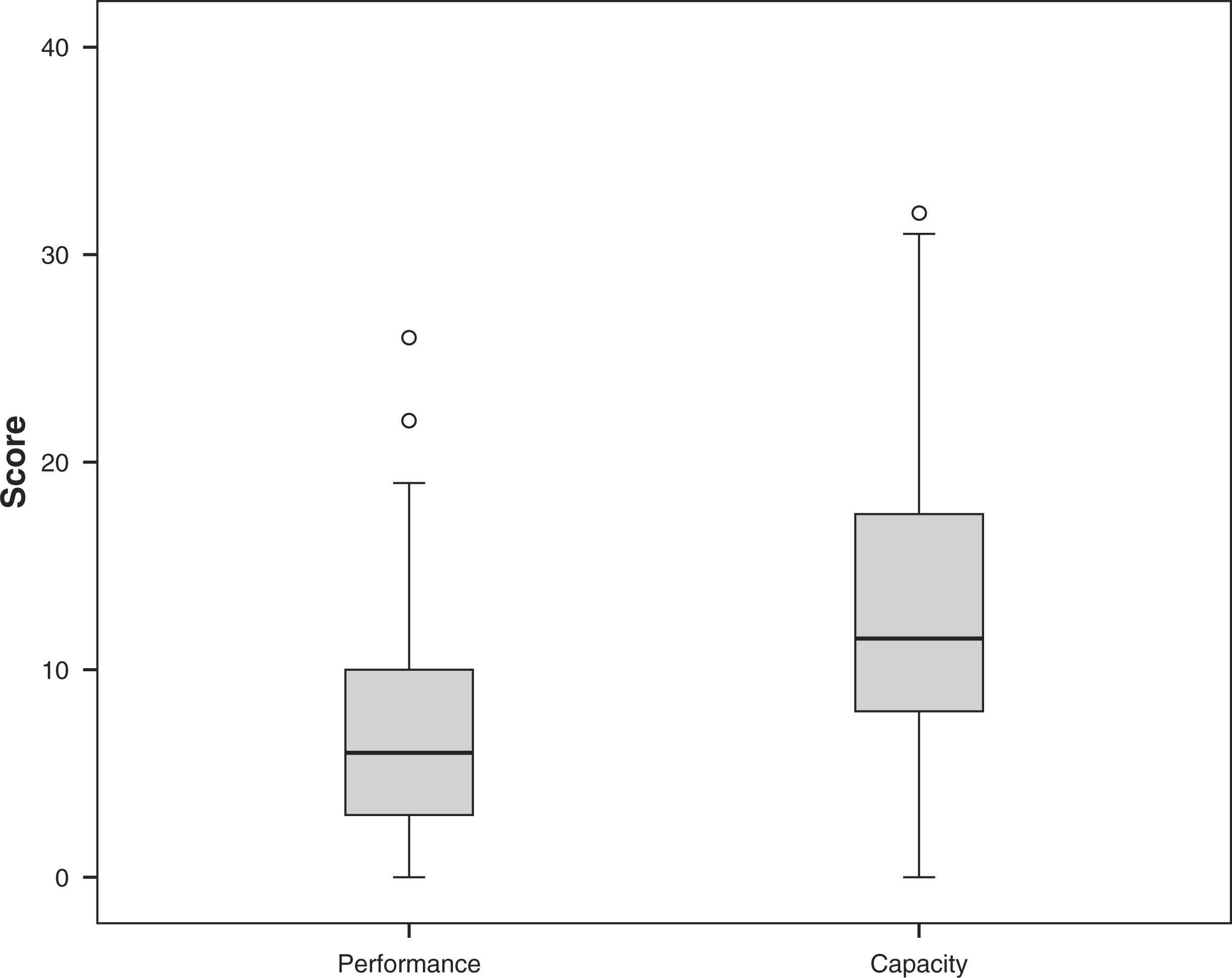
Elderly subjects had slightly more ICD diagnoses (r = 0.284, p = 0.004), more categories used for environmental factors (r = 0.392, p = 0.003) and worse performance (r = 0.297, p = 0.003). Subjects who had more ICD diagnoses and problems with a larger number of body functions also used a larger number of devices (r = 0.415, p < 0.001 and r = 0.367, p < 0.001, respectively).
Discussion
We found out that ICF can be used in everyday P&O clinical practice. Using a limited number of categories and no qualifiers only slightly prolongs the time needed for examination of the patient. The largest number ofcategories was used for activities and participation, followed by body functions. The same number of categories was used for body structures and environmental factors. Activity and participation limitations are the main factors for defining the purpose of P&O use.7,15 Impairments of body functions and structures determine the functional requirements, design and components of the device.7,15 Environment in which the device will be used may influence material selection and sometimes also the components.
Some categories were used in almost all patients, whereas others, such as communication and transfers, only in a few cases. History was obtained from each patient, but when there were no problems, it was usually not coded. Some categories were used only in patients who had problems and not if a patient did not have problems, even though several times they were inadvertently checked. Some other categories that are the basis for decision making regarding the appropriate P&O device, such as range of motion, muscle power, gait pattern, structure of the skin and so on, were also used if the patient did not have a problem. It seems that the results represent the author's opinion on which categories are relevant and which are not. For stronger conclusions, additional studies are necessary, whereby more clinicians from different facilities and different countries should be involved.
The fact that in all patients, categories from all four components of the ICF were used validates the philosophy and the main idea of the ICF that all components are important and interrelated. It also demonstrates thebroad profile of a specialist of physical and rehabilitation medicine 26 who – even at an outpatient clinic – realizes that all these components are important for a person's functioning.
Using categories at the second level keeps the list within a reasonable length. Adding categories on the third or even fourth level would probably give more detailed information, but the list would become several pages long and much more difficult to use. Adding qualifiers would also give additional information, but when using categories on the second level the qualifiers are not sensitive enough. For example, subjects may have decreased muscle power only in one muscle or one group of muscles (e.g. ankle dorsal flexors), which results in activities and participation problems, but this may not cover four per cent of all muscles that would justify assigning the qualifier one. An additional problem is the nonlinearity of qualifiers, so our belief is that it is enough to demonstrate that a person has problems with a certain category and then use more accurate measurement tools for quantification. To demonstrate the impact of P&O devices on a person's functioning, we have to measure capacity and performance. It can be done using existing ICF qualifiers, using the new qualifiers suggested by Schraner et al. 27 or using some other measurement tools. For the body functions component we can use the outcome measures suggested by Hebert et al. 5 while for activities and participation such a review is needed. But even with ICF qualifiers we demonstrated that P&O devices improve an individual's functioning.
Annex 9 is not as useful as it may seem upon first glance. It is actually not a list of categories and categories, but mainly of nests and it also contains two whole chapters. 4 The result is actually a much longer list or very limited information of only nests and chapters. It seems that the author's selection of categories was good but, again, it would have to be verified by other clinicians from other facilities and other countries in order to arrive at a final shortlist for use in P&O practice. Actually, several lists may prove to be better, because Figure 4 shows that there are categories mainly checked in subjects with lower limb problems and others mainly checked in subjects with upper limb problems, while very few were used in both. This may indicate that short core sets for lower limb and upper limb problems will be the best solution for P&O practice. A larger number of ICF rather than ICD codes provide quick additional information to clinicians on the profile of problems that a person has their functioning. However, a further study would be desirable on how valuable this additional information actually is.
Another limitation of Annex 9 is that it does not contain any categories from the body structure component or from environmental factors. Another limitation is that the study has only been used in clinics of one clinician and no subjects with spinal problems were included, so additional studies are needed.
Conclusion
The ICF can be used in everyday P&O clinical practice. A list of all checked categories provides quick additional information. To be able to demonstrate the influence of P&O devices on a person's functioning at least for activities and participation, we have to use qualifiers or alternatively some other outcome measures that measure the domains in which the patient has problems.
Footnotes
Funding
This research was part of the project L3-0113 (B) entitled ‘Development and validation of clinical tools developed on International Classification of Functioning, Health and Disability (ICF)’ (applied research project) funded by Slovene Research Agency.