
Abstract
Background: Community living individuals with lower limb amputation have low balance confidence but the level of balance confidence in the first six months after discharge from prosthetic rehabilitation is not known.
Objectives: To determine if balance confidence levels differ after discharge from prosthetic rehabilitation and to determine if balance confidence at discharge predicts social activity at three months post-discharge while controlling for important covariates such as walking ability.
Study Design: Prospective study.
Methods: Subjects (n = 65) experiencing their first unilateral transfemoral or transtibial amputation were recruited and followed-up one and three months post-discharge. Measures of balance confidence (Activities-specific Balance Confidence Scale) and walking ability (L Test) collected at discharge were used to predict social activity (Frenchay Activities Index) at follow-up.
Results: Despite a 14-second mean improvement in walking ability the mean balance confidence scores did not change significantly between discharge (71.2/100) and at three-month follow-up (69.4/100). Confidence scores and basic walking ability at discharge were the two strongest predictors of three-month social activity. Multiple regression modelling indicated that balance confidence and walking ability explained 64% of the variance (standardized beta = 0.34 and -0.37 respectively) in social activity (adjusted R2 = 39%).
Conclusions: Balance confidence after discharge from prosthetic rehabilitation for lower limb amputation is low and scores do not improve over the first three months post-discharge despite improvements in walking ability. Discharge balance scores confidence independently predicts three-month social activity scores.
Clinical relevance
Our experience suggests that balance confidence is not directly addressed during prosthetic rehabilitation despite evidence suggesting that mean balance confidence of this population is low. Some change in confidence may be indirectly obtained through traditional rehabilitation; however, programmes augmented with strategies based on Bandura’s theory may increase confidence further promoting improved social activity.
Introduction
Individuals with lower limb amputation are at risk of decreased participation in daily and social activities which may have a negative influence on their quality of life.1,2 Obvious factors such as prosthetic fit, strengthening, balance and gait retraining that deal with the physical nature of the amputation receive the majority of attention during rehabilitation while psychological factors receive little or no attention. Acknowledging that learning a new skill, such as prosthetic ambulation, largely relies on having the appropriate physical attributes, whether the individual uses the new skill or not also involves on having the self-efficacy or confidence to perform targeted activities. Past studies have demonstrated that up to 65% of community living individuals who have had their lower limb amputation for more than six months have low balance confidence. 3 Moreover, low balance confidence is strongly associated with decreased prosthetic mobility and social activity. 4 When followed prospectively over a two-year period, levels of balance confidence remained unchanged. 5
Balance confidence (also referred to as falls self-efficacy) is the belief that the individual has the capability toperform an activity or action without losing their balance. 6 It is based on Bandura’s 7 Social Cognitive Learning Theory which suggests that confidence is at least as important to predicting and changing behaviour as having the appropriate skill level. Confidence is hypothesized to influence behaviour both directly and through its interaction with the other determinants of behaviour. High levels of confidence may therefore have positive results on individual functioning and well-being. Further, confidence, like skill, is said to be modifiable given an appropriate and targeted intervention. Therefore, efforts to address low levels of confidence may have a positive effect on behaviour oriented outcomes.
While evidence suggests that balance confidence is an issue among individuals with chronic or long term amputation,3,5 no study has investigated this condition during the period of time immediately after discharge from prosthetic rehabilitation. This information is important as it may provide evidence as to whether intervention should be provided early on in the process of prosthetic rehabilitation. Another gap in our understanding is whether, as Bandura theorizes, self-efficacy is as important a predictor as skill in predicting behaviour. Or, in the context of lower limb amputation, whether balance confidence is as powerful an indicator as walking ability in predicting social activity. The purpose of this study was to assess whether balance confidence varied one and three months after discharge from prosthetic rehabilitation and to investigate whether balance confidence independently predicted participation in social activities while controlling for important covariates, such as walking ability.
Methods
A prospective repeated measures design was used to collect data at discharge and then again at one and three months post-discharge from inpatients attending a tertiary care hospital in Canada. We recruited individuals from an inpatient hospital amputee programme using a consecutive sampling technique. The programme is set in a tertiary rehabilitation hospital in the province of Ontario, Canada. Its primary goal is to achieve a definitive prosthetic device for individuals who have a goal of walking post-amputation. A multidisciplinary team provides the four- to six-week programme, however, only the physical therapists are dedicated to theamputee programme. The primary focus of our rehabilitation program is daily physical therapy sessions (Monday through Friday) to work on shaping the residual limb, strengthening, cardiovascular conditioning and prosthetic mobility which includes basic-to-complex ambulation retraining based on the individuals tolerance. Occupational therapy provides training regarding donning/doffing the prosthesis, bathing and dressing. Nursing provides specialized skin care supervision and social work is available for consultation regarding funding. Individuals with unilateral transfermoral (TF) or transtibial (TT) lower limb amputation were included if they:
were discharged to community;
were older than 20 years of age;
had a goal of walking using their prosthesis;
were able to understand English.
Individuals were excluded if they:
did not use a prosthesis at time of discharge
were having a revision of a previous amputation
did not provide full information at each of the data collection times
were deemed medically unstable by the attending physician.
The sample size was set at 80 participants which would enable modelling of up to six predictor variables given an alpha of 0.05, power of 0.80 and a medium effect size (squared multiple correlation R2 = 0.15) when using multiple regression analyses. 8
Measurement
A number of sociodemographic and clinical variables were captured including age, sex, amputation cause and level, and use and type of gait aid.
Balance confidence data were captured using the 16-item Activities-specific Balance Confidence (ABC) Scale. 6 This captures reported self-efficacy or confidence in performing specific activities without falling. Respondents rate their confidence to perform simple-to-complex activities on a scale ranging from 0 (no confidence) to 100 (extremely confident). A mean score is then calculated. Powell and Myers 6 have suggested a cut point of 80 or less to identify individuals who may benefit from intervention to address balance confidence in the elderly population. The ABC has been found to have good reliability and there is evidence supporting the validity of this scale in the amputee population. 9
The L Test 10 was used to assess basic walking ability. The L test, a modified ‘timed up and go’ test, requires the individual to stand up from a standard height chair, walk three metres, make a 90-degree turn, walk seven metres and then turn around and retrace their path. The time it takes in seconds to complete the 20 metre circuit from the time the individual starts to stand to the point that they sit down again is recorded. The test was demonstrated and participants were provided with a single practice trial at all-time points and then after a short rest of at least two, but no more than five, minutes the individual’s performance on this test was timed with final times reported. Standardized encouragement such as, ‘You’re doing well. Remember to go around the “x” and retrace your steps back to the start’, was provided, as specified by the authors. 10 The reliability and validity of this test in a sample of individuals with lower limb amputation was found to be excellent. 10
The 15-item Frenchay Activities Index (FAI) 11 was used to capture information on social activities at three months after discharge from the rehabilitation programme. The items reflect the frequency of performance of basic and instrumental activities of daily living over three domains (inside, outside and higher order activities). Responses were captured on a four-point scale and item responses were summed. The total scores range from 0 (very limited) to 45 (very active). Evidence from a sample of individuals with unilateral lower limb amputation suggests this index is reliable and support for validity exists to use the FAI in this population. 11
Procedure
Data were collected by two trained research assistants. Physical therapists from the inpatient amputee program asked if individuals would be interested in participating in a study. If they received a positive response one of two trained research assistants explained the study, answered all relevant questions and obtained consent from those who were still interested.
Baseline data, except social activity function, were collected from the subjects within 72 hours prior to discharge. The order of the tests and questionnaires was randomly applied based on a simple random selection scheme of drawing the test name from a hat. Rest breaks were provided as necessary. Keeping with clinical practice at the rehabilitation unit all of the subjects were scheduled for a follow-up appointment for one and three months post-discharge. Information on balance confidence and walking ability was also collected at each point of follow-up. Social activity function was collected at the three-month post-discharge time point. Ethical review and approval was provided by the local university and hospital ethics review board.
Data Analysis
Summary statistics, such as means, standard deviations and proportions, are provided to describe the sample. To address Objective one, we hypothesized that there would be a statistically significant difference in balance confidence over the three time points. Specifically, we anticipated that individuals would have greater balance confidence upon follow-up given that the individuals would be more used to using their prosthesis. One-way repeated measures analysis of variance (ANOVA) was used to address this hypothesis. Multiple linear regression was used to assess our second study hypothesis that balance confidence scores taken at discharge would independently predict social activity at three months while controlling for basic walking ability. Based on Bandura’s premise that confidence or self-efficacy is as important (if not more important) than skill, we anticipated that the standardized beta coefficient of the balance confidence variable would be equal to, or stronger in magnitude than, that of the coefficient for walking ability. Age, sex, amputation level and gait aid were included in the regression analyses as these have been shown to be important in predicting social activity in previous studies. 4 SPSS version 14 was used for data analyses. An alpha of p < 0.05 was set to determine if findings were statistically significant.
Results
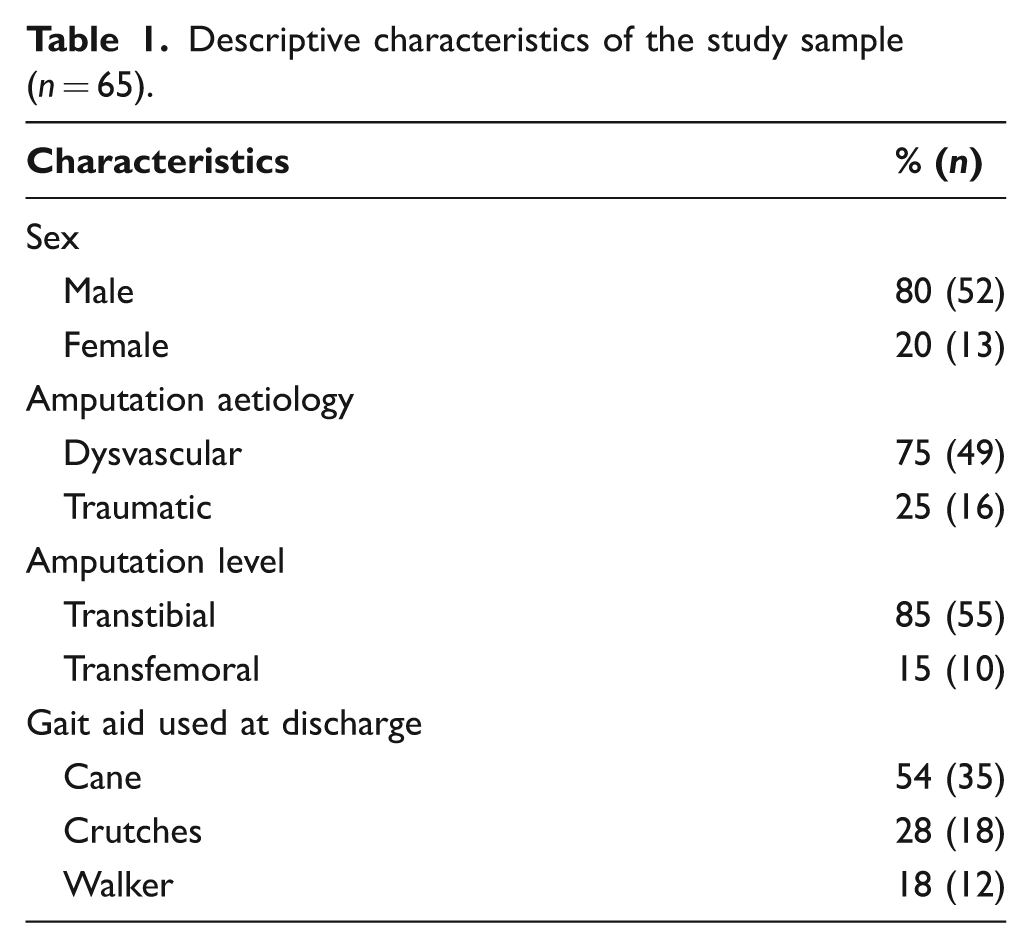
A total of 83 individuals were recruited, however, 18 individuals did not provide full information or complete the study for a variety of reasons (Figure 1) leaving a total of 65 participants, or 78% of those recruited. The mean age at discharge of the mostly male (80%) sample was 59.1 years (SD = 18.1). The majority of amputations were at TT level and the entire sample was ambulating independently at discharge, however all used some form of gait aid, primarily a cane or single crutch. See Table 1 for additional sample characteristics.
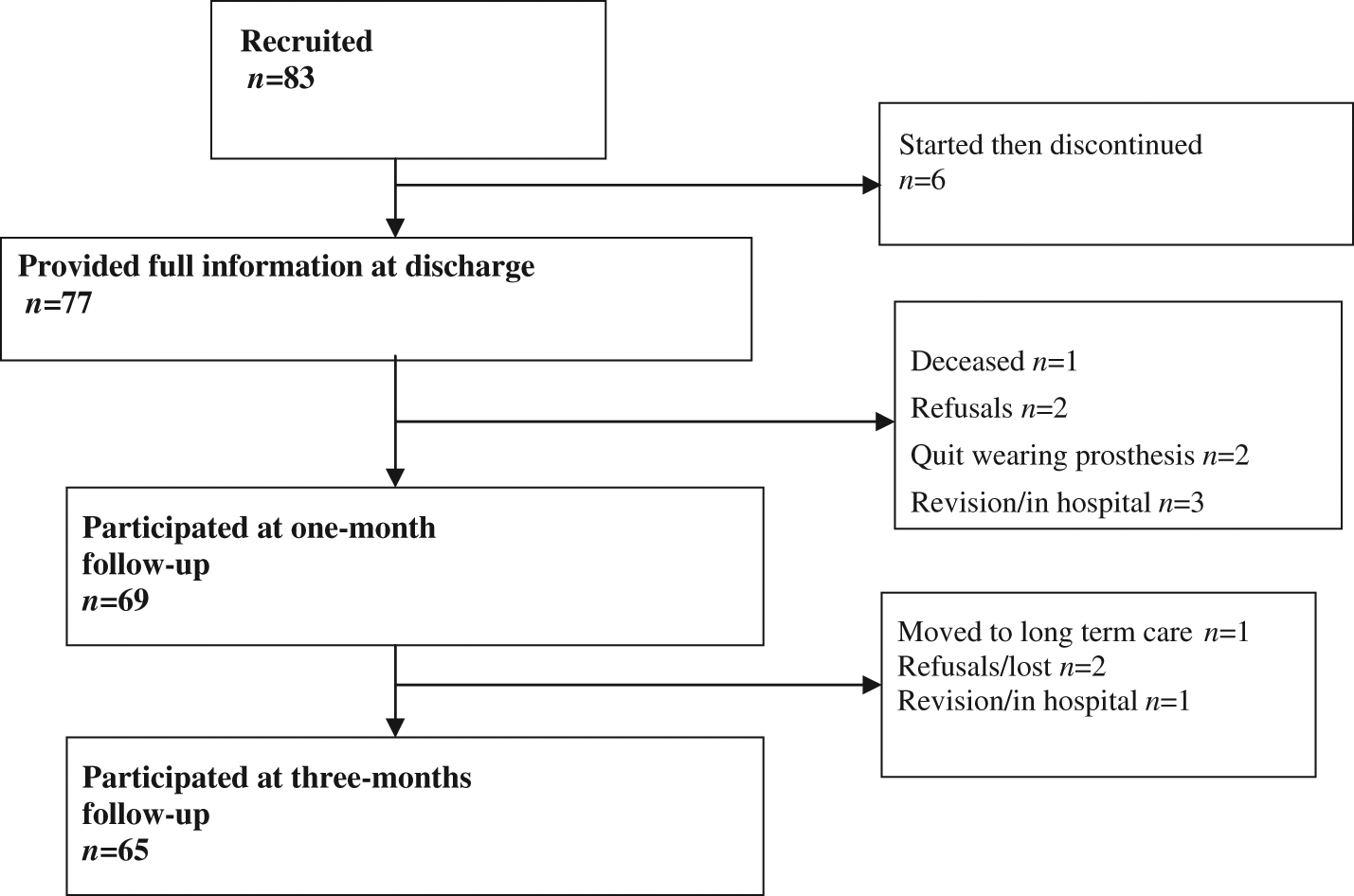
Recruitment scheme for three data collection sections.
Descriptive characteristics of the study sample (n = 65).
The mean balance confidence scores at discharge 71.2 (SD = 17.6), one-month post-discharge 69.8 (SD = 23.4) and three-months post-discharge 69.4 (SD = 24.3) were not statistically different (Table 2). Despite no group change, 14% of the sample reported a one standard deviation (>17.6) improvement between discharge and one-month follow-up and 5% of the total sample reported an increase in scores between one and three months post-discharge. Conversely, 11% of the total sample reported a one standard deviation decline between discharge and one-month follow-up and 9% declined between one and three months follow-up. Interestingly mean walking ability (Table 2) improved as a statistically significant decline in walking time (∼10 seconds) between discharge and follow-up times was observed.
Descriptive for Balance confidence, walking ability, and social activity.
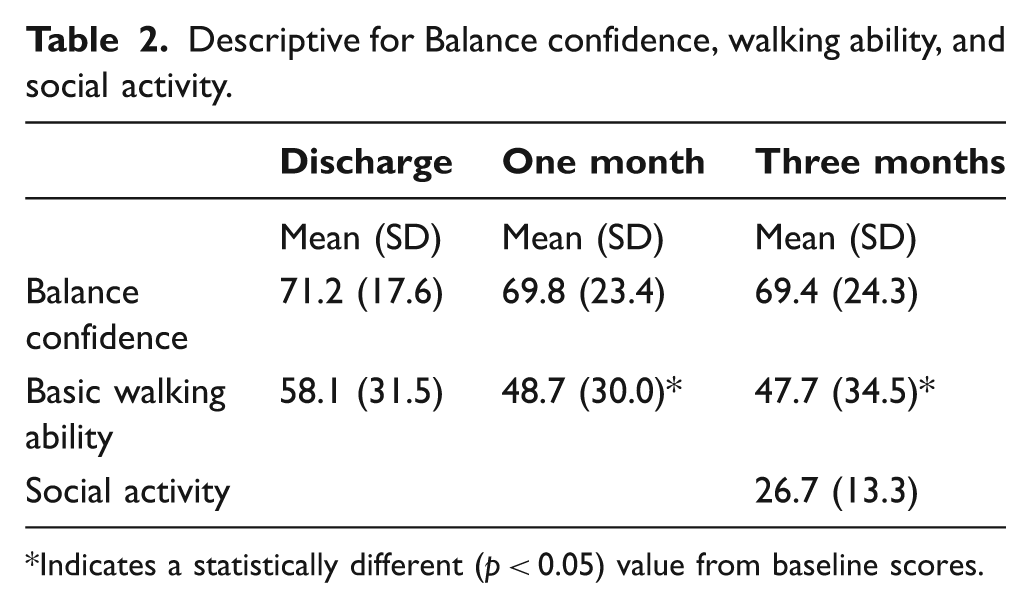
Indicates a statistically different (p < 0.05) value from baseline scores.
The mean social activity score at three months was 27.6 (SD = 13.3). A total of 39% of the variance in social activity was accounted for in the regression model (Table 3). Both discharge balance confidence and basic walking ability were significant in predicting social activity while controlling for other important variables. The inverse relationship with walking ability (denoted by the negative standardized beta) and the positive association with balance confidence were as hypothesized. The magnitude or the strength of the betas was similar for these two variables indicating that skill and balance confidence accounted for approximately the same amount of variance in social activity.
Regression Analysis of social activity on balance confidence, walking ability and control variables.
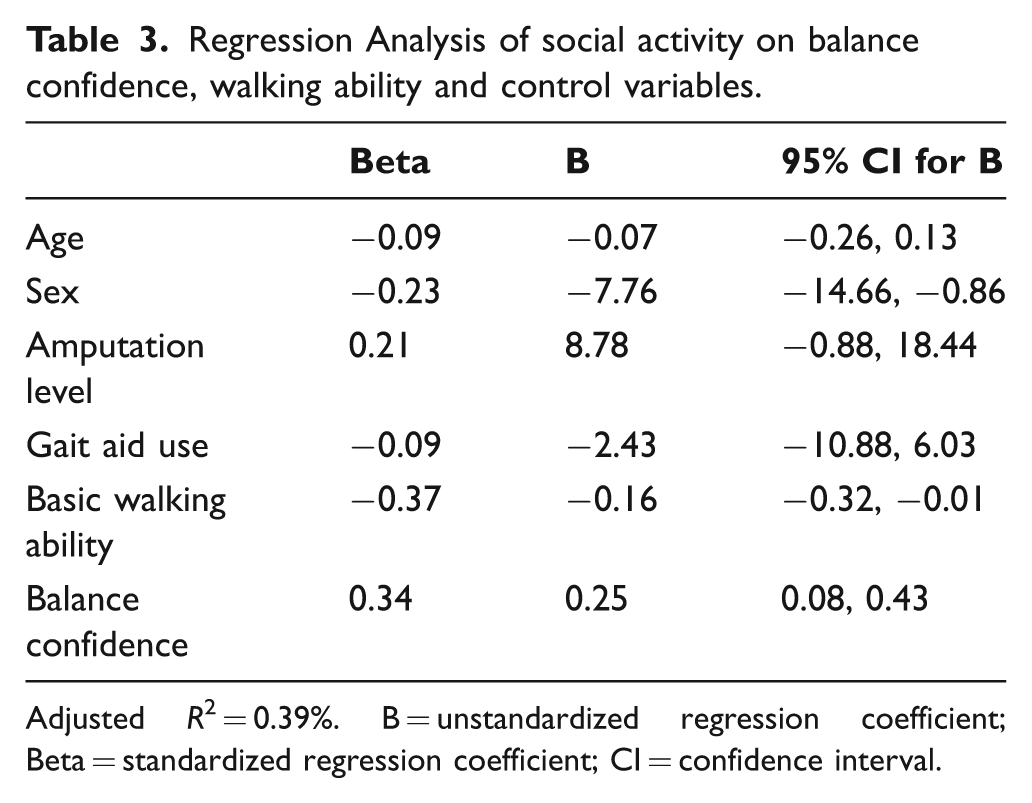
Adjusted R2 = 0.39%. B = unstandardized regression coefficient; Beta = standardized regression coefficient; CI = confidence interval.
Discussion
The results suggest that balance confidence immediately after discharge from inpatient rehabilitation does not vary from discharge to follow-up three months later. As hypothesized, balance confidence at discharge was predictive of social activity measured at three-months post-discharge. Moreover, balance confidence was of equal strength as walking ability (skill) in predicting social activity which lends support to Bandura’s claim about the importance of confidence in predicting behaviour.
Descriptively, our sample generally reflects the population of individuals having a lower extremity amputation in that the majority were older males who had a TT amputation. Although the walking ability of our sample increased from discharge to the one-month follow-up they were still on average 14 seconds slower than a more experienced group of prosthetic walkers. 10 While our data cannot confirm this finding it would suggest that our sample might expect an additional increase in walking ability as they become more experienced walkers. Similarly, the mean level of social activity for our sample was also about one half standard deviation lower than that of the published mean of amputees 11 which may be due to the fact that the reference sample were well integrated into their social activities while using their prosthetic limbs.
Balance confidence ranged between 71% and 69% (respectively) between discharge and follow-up in our sample of individuals who had just completed their inpatient rehabilitation programme. Not surprisingly, given a mean difference of 1.8% the variation in ABC scores was not statistically significant. This finding does not support our stated hypothesis that balance confidence would improve at discharge after rehabilitation and in the few months following.
Interestingly, the level of balance confidence over the study sample was 2% to 7% higher than a large sample of community living individuals with lower limb amputation who had been using their prosthesis for six or more months.3,5 Regardless, the mean confidence level was still lower than the threshold level (80/100) that Myers et al. 12 recommend warrants intervention. This suggests that even individuals who have recently completed their rehabilitation experience an impaired level of confidence. We did note, however, that while the group mean did not change, a number of individuals improved while some declined in their balance confidence upon follow-up. Beyond regression to the mean this may suggest that the experience of community ambulation may have an influence on the level of balance confidence, albeit not always a positive experience. Other explanations for this finding, aside from natural variation, might include a change in health status or the possibility that some of the, but not the entire, sample received additional therapy. While we monitored for the former and found that a substantial number of individuals reported variable health between test periods we did not monitor the latter although this seems unlikely given that our clinic is highly specialized towards prosthetic rehabilitation with no other similar programmes in the region.
We observed an improvement in walking ability over the follow-up period which did not correspond with a parallel change in balance confidence. This fascinating finding suggests that balance confidence is quite independent of improvement in walking ability, or in this case, being a faster walker. This result is not too surprising. The L test is not a complex walking test to complete and it seems very plausible that daily walking would lead to improvement in walking speeds even in those individuals who only walk short distances within their home. On the other hand, the ABC Scale is comprised of an increasingly complex list of activities (items) that are designed to challenge an individual’s balance. It seems plausible that a longer period of adjustment would be required to invoke a change in confidence. Given that improvement has not been observed over time in either our study sample or in a prospective study sample of experienced prosthetic ambulators 5 where daily walking likely occurs provides support for this hypothesis. Therefore, it also seems plausible that an improvement in balance confidence may require a more specialized or targeted intervention. In fact, most of the existing intervention studies designed to improve balance confidence in other populations of older adults, such as stroke, have used traditional approaches such as lower extremity strengthening, balance training and/or walking programmes. 13 While some improvement has been observed related to these types of programmes, primarily Tai Chi, it seems plausible that addressing the key tenants as identified by Bandura 7 may lead to further improvement beyond existing strategies. Specifically programmes would provide experiential and vicarious learning, positive verbal reinforcement and acknowledgement and strategies to cope with physiological reactions related to items on the ABC that lead to anxiety. This hypothesis requires assessment.
Both walking ability and balance confidence scores at discharge were significant predictors of social activity three months later. The strength or magnitude of the coefficients for these variables was virtually the same and together these variables explained a moderate amount of the variation in the frequency of social activity. This finding would appear to support Bandura’s theory that confidence with balance is at least as important as basic walking skill in predicting social activity behaviour among prosthetic amputees. Therefore, clinicians can get a sense of what the future social activity of their patients will be (at three months) by reflecting on the balance confidence and walking skill data collected at discharge. Individuals with low balance confidence and/or those with slow walking times on the L Test could then be identified as those who will require additional treatment and follow-up particularly if their goal is to maximize their participation in social activities.
In this study a number of variables, such as age, amputation level, amputation cause and gait aid use, were not important in predicting social activity yet these variables have been shown to predict social activity in the amputee population in other studies. 4 It is difficult to determine exactly why these variables failed to contribute. Several factors related to the sample may suggest the different findings. Specifically the sample recruited for this study came from a single amputee clinic, consisted of individuals who were on average six years younger, had a greater number of TF level amputations and all used gait aids. While these differences in the distribution of the variables may in themselves explain the different findings it is critical to remember that we sampled individuals immediately at the time of, and then again within a few months of, discharge from prosthetic rehabilitation. It seems very likely that this temporal difference in sampling may identify a different experience in the natural history of recovery particularly when we acknowledge that the balance confidence in our sample was higher than the other studies.3,5 Other covariates would include mood or symptoms of depression, mobility capability and pain. All of which have been shown to contribute to explaining social activity post-lower limb amputation. 3 Future studies which include these additional variables should be considered.
Other limitations include the fact that our study used a volunteer sample of individuals who attended a rehabilitation programme for their first unilateral amputation with the specific goal of obtaining a prosthesis and a secondary goal of maximizing their ability to walk using their prosthesis. This intensive inpatient programme likely targets individuals who have better health and may not be the norm at other centres providing such rehabilitation and therefore the results of this study may not generalize to the larger population of individuals with lower limb amputation.
Providing data from a longer follow-up period would have been ideal. However given the stability of the balance confidence scores and the fact that there was no statistical difference in the basic walking ability times three months after discharge from inpatient rehabilitation and given the fact that the balance confidence scores are relatively similar for the chronic population it seems plausible that additional data collection after the three-month follow-up is likely unnecessary. Replication using different samples of individuals, such as those from other countries or rural regions or those with varying amputation levels/situations (for example, bilateral amputations) is warranted and would determine whether this phenomenon of low balance confidence is an artefact of our sample.
Conclusion
Individuals with lower limb amputation regardless of their time since discharge from rehabilitation have low balance confidence and change in confidence does not correspond with change in walking ability during the first three months post-discharge. Balance confidence at discharge from inpatient prosthetic rehabilitation was important in predicting social activity while controlling for walking ability and other important variables.
Footnotes
Acknowledgements
The authors wish to thank the study participants and Susan Brown and Christine Fraser for their dedication and skill in data collection. The authors would also like to recognize the Parkwood Hospital Foundation who provided operating funds for the study and the Canadian Foundation forHealth Research for the salary assistance provided to Dr Miller.
Funding
This work was supported by an operating grant from the Parkwood Hospital Foundation. Salary support for Dr Miller was provided by the Canadian Institutes of Health Research.