
Abstract
Background and Aim: Education programmes of the International Society for Prosthetics and Orthotics (ISPO) are directed primarily at prosthetists and orthotists. In a multidisciplinary setting, greater attention should be given to other professionals working in the field of amputation, prosthetics and orthotics. This includes, among others, physiotherapists, occupational therapists and residents and physicians from orthopaedics, vascular surgery and physical medicine and rehabilitation (PM&R). The aim of this paper is to describe the education programme in amputation and prosthetics for residents in PM&R in the Netherlands. The programme is based on concepts of the International Classification on Functioning, Disability and Health (ICF).
Technique: This narrative paper presents the amputation and prosthetics education programme for residents in PM&R in the Netherlands. The programme is based on two models: the ICF and the Canadian Medical Education Directives for Specialists (CanMEDS).
Discussion: ICF core sets for amputation and prosthetics need further development. Subsequently, the application of these core sets can help stimulate the education of residents in PM&R, and other multidisciplinary team members who work in amputation rehabilitation
Through this education programme, residents work closely with other team members using the common language of the ICF, enhancing treatment and technical advice in amputee care.
Keywords
Background and aim
The International Society for Prosthetics and Orthotics (ISPO) is committed to facilitate and enhance education in all healthcare disciplines that are involved in prosthetics and orthotics (P&O) throughout the world. ISPO has detailed appropriate education and training guidelines for professional prosthetists/orthotists (Category I) and for orthopaedic technologists (Category II). The philosophy and curriculum are widely accepted by international governmental and non-governmental agencies in this field.
ISPO compiles and reviews education standards throughout the world, governing the practice of professions working in P&O care, rehabilitation engineering and related areas. Information exchange and dissemination is achieved through world congresses, instructional courses, workshops, conferences, educational symposia, publications, websites and audiovisual media. Furthermore, ISPO provides consultation and expertise where there is an identified need for development. Upon request, ISPO evaluates P&O training programmes throughout the world for ISPO Category I and II recognition. The evaluation includes student entry requirements, teaching content, clinical training, quality and administrative procedures. 1 The ISPO Education Committee has to date focused only on students of P&O, with no attention toward training of other health professionals, such as physiotherapists or physicians.
This paper outlines the contents of the amputation and prosthetics education program for residents of Physical Medicine and Rehabilitation (PMR) in the Netherlands with reference to concepts from the ICF, as an example of how ISPO could be involved with furthering the education of other health professionals.
Technique and discussion
The International Classification of Functioning, Disability and Health
The International Classification of Functioning, Disability and Health (ICF) model is presented by the World Health Organization (WHO) as an instrument for analysis of functioning of the patient. 2 The model defines the underlying pathology, problems at the level of organ functioning, activity level, the potential for restoring optimal personal function and preventing further limitation. The ICF model considers the ability of an individual to participate in society. This can be dependent not only on personal functioning, but also on personal factors and contextual factors affecting the individual's life and environment.
The ICF model is also used as an educational instrument. It can help to explain functioning in individuals with different diseases, including conditions that result in a need for an orthosis or prosthesis. For medical students and PM&R residents, the model can be used during their training programme to help provide an understanding of the relationship between disease and functioning.
Physical Medicine and Rehabilitation
PM&R, or physiatry, is a branch of medicine which aims to enhance and restore functional ability and quality of life to those with physical impairments or disabilities. 3 A physician who has completed training in this field is referred to as a physician in PM&R, or physiatrist. Physicians in PM&R specialize in restoring optimal function to people with muscle, bone, tissue, and/or nervous system disorders and impairments. These include, among others, people with amputation, stroke or spinal cord injuries, who experience loss of function and/or performance. A team approach is essential, and the team should aim to provide well coordinated care to all patients. An emphasis is placed on optimizing function through a combination of treatments including medication, physical modalities, physical training with therapeutic exercise, modification of movement and activities, adaptive equipment and assistive devices, orthoses (braces), prostheses, and experiential training approaches. The key focus of rehabilitation is to enable an individual to function optimally within the limitations placed upon them by the condition experienced. These conditions are often permanent, with no known cure, and restoration to a pre-morbid level of function may not be possible. The emphasis of rehabilitation is instead placed on optimizing an individual's quality of life.
ICF model in education and training P&RM
Theme chart – amputation.
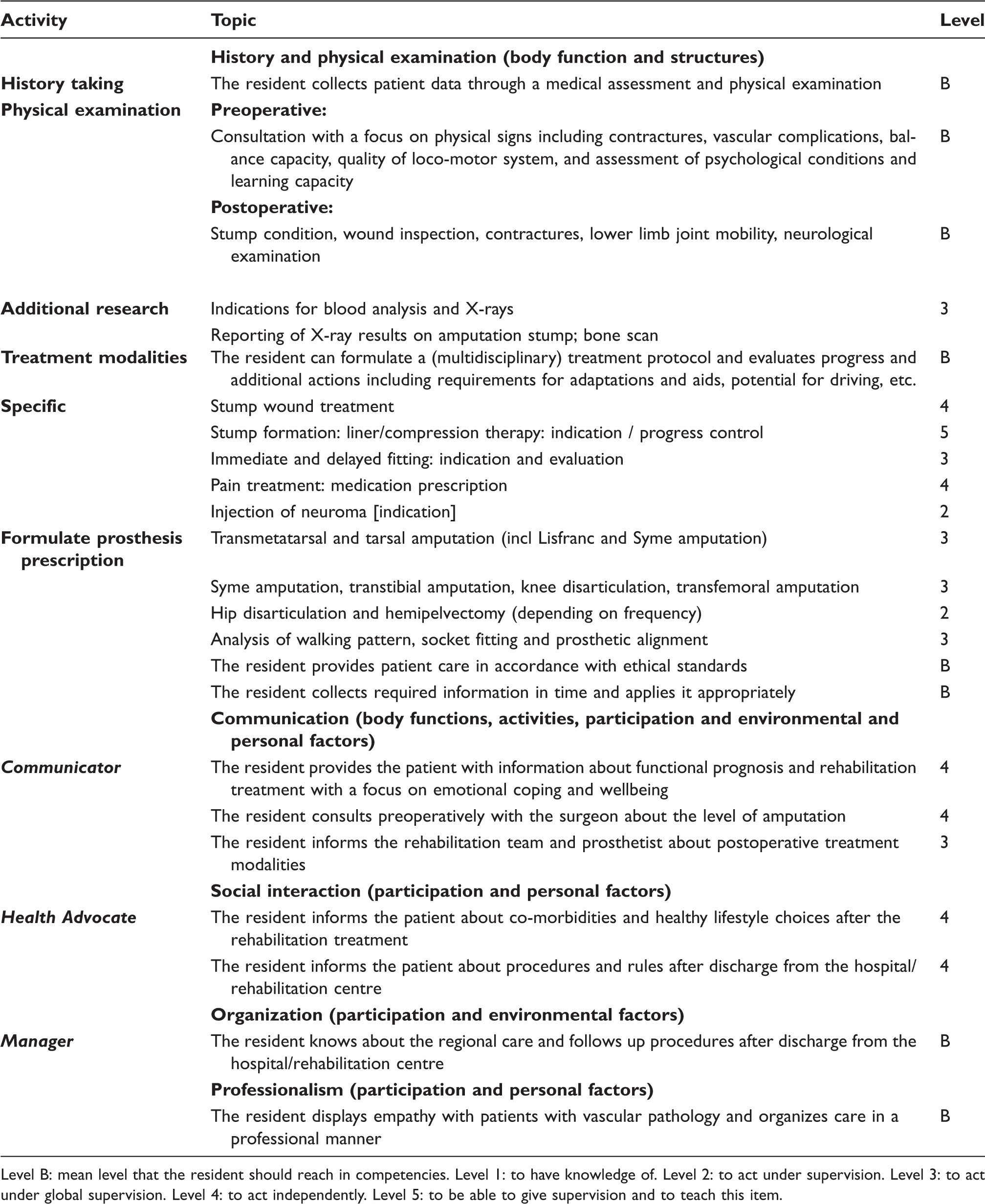
Level B: mean level that the resident should reach in competencies. Level 1: to have knowledge of. Level 2: to act under supervision. Level 3: to act under global supervision. Level 4: to act independently. Level 5: to be able to give supervision and to teach this item.
Throughout their education, residents in PM&R refer to the ICF model during teaching groups, ward rounds and in bedside training in hospitals or rehabilitation centres. The model is used, for instance, in patients with diabetes, stroke, amputation or spinal cord lesions and provides possibilities toward analysis of function and adequate prescription of the assistive devices related towards function. The ICF model is an instrument for every doctor and health professional to relate the medical aspects towards functioning and participation. A quick change can be made from the disease model (diabetes; amputation) towards functioning (walking, Activities of Daily Living (ADL)) and participation (work, hobby and well-being). It is informative for students and professionals working with a multidisciplinary approach.
At the end of their training period, core competencies of Dutch physicians, including PM&R, are expected to be met. These competencies are formulated from the Canadian Medical Education Directives for Specialists (CanMEDS) and are to be a medical expert, a good communicator, a collaborator, a manager, a health advocate, a scholar and a professional (Figure 1).
4
CanMEDs model.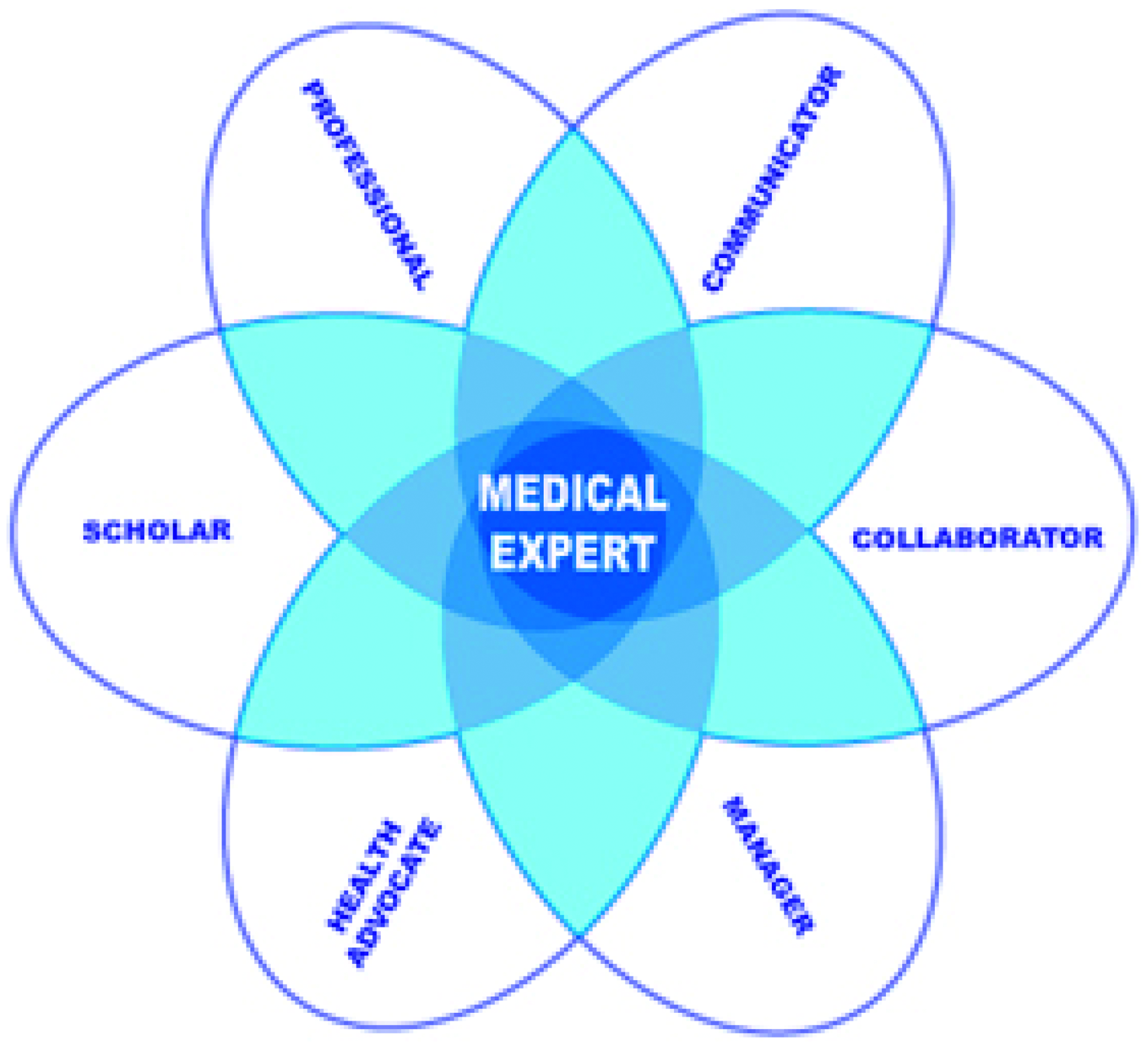
In the ICF model, these core competencies can be achieved at different levels. Analysis of body structures includes the role as medical expert and professional. In activities, there is a focus on being a collaborator and health advocate. Under participation, the role as health advocate, communicator and manager is essential. These competencies form a base on which each physician in PM&R should work. Consequently, the ICF is the fundamental tool of every PM&R physician.
Training in PM&R
Prescription of prostheses, orthoses, orthopaedic shoes and most assistive technologies in the Netherlands is given by a PM&R physician. In the medical notes of the physician, a pre-printed ICF-based scheme helps in analyzing a medical problem and formulating a prosthetic or orthotic solution. In Figure 2, an example of the ICF model related to aspects of care for individual's with transtibial amputation is shown. This scheme assists the resident and team members in determining items to be discussed in team meetings or to be addressed with patients.
Example for applying the ICF-model in case of transtibial amputation.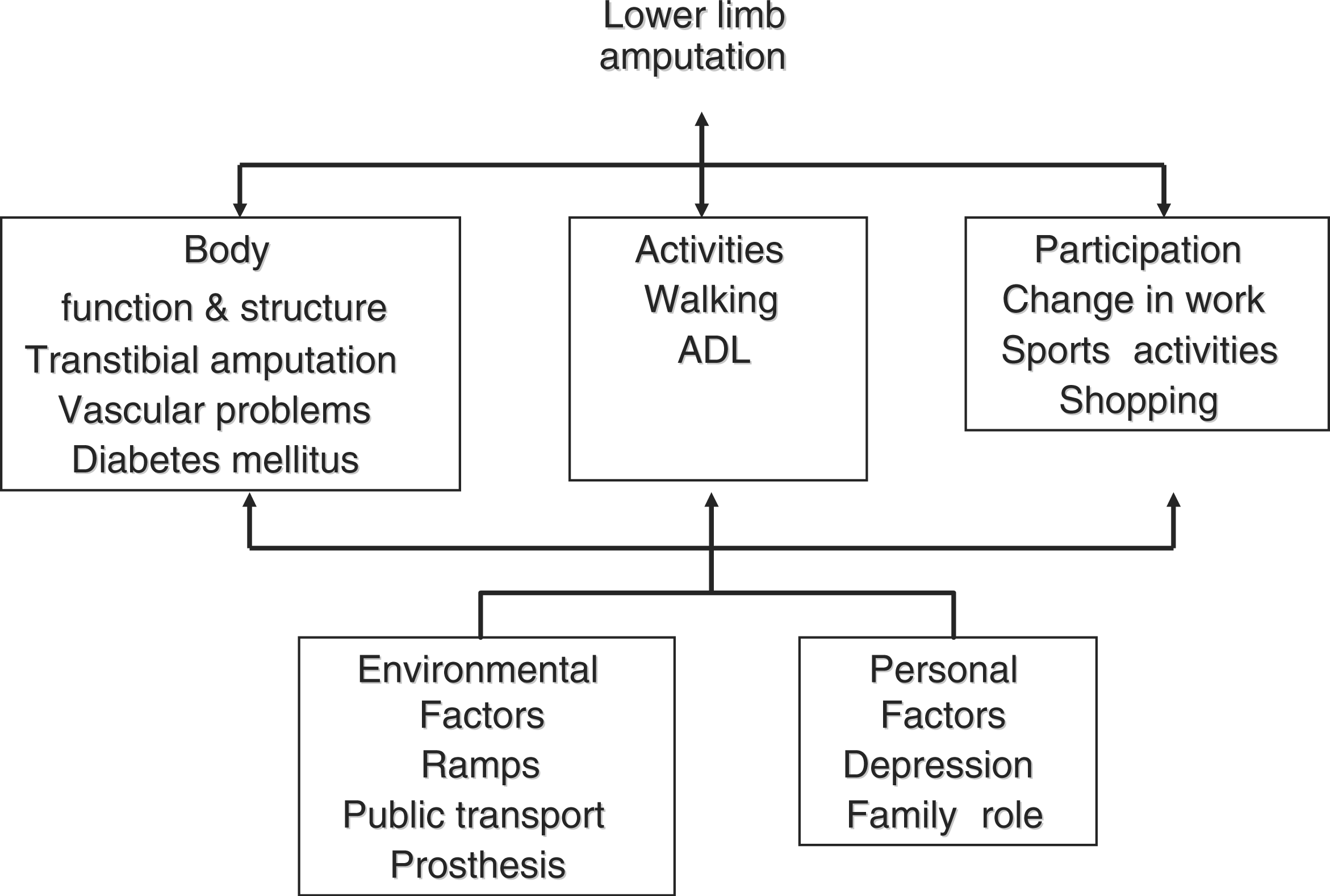
Medical charts, discharge letters and prescription forms for prostheses and orthoses give an overview of potential issues with functioning and participation which should be addressed. There has been some research performed on the selection of outcome measures for rehabilitation of people with lower extremity amputation within the ICF activities. However, there is a universal absence of quality evidence demonstrating responsiveness. 5 – 7 The same findings apply for upper limb amputations. 8
National training in PM&R in the Netherlands
In the Netherlands, residents in PM&R are trained in a four-year curriculum. In 2010, a new national training scheme was approved by the General Assembly of the Dutch Society for PM&R. The new scheme incorporates concepts from the ICF and CanMEDS models (Figure 1). In developing the new training scheme, key components of the CanMEDS Model in PM&R were used as the basis of the curriculum. Residents are trained in eight themes: stroke and cerebral contusion, spinal cord lesions, neuromuscular diseases, osteoarthritis, pain, poly-trauma, paediatric rehabilitation and lower extremity amputation and prosthetics. 9 All themes have their own theme chart similar to the one for amputation in Table 1. The eight themes address two areas of training: (1) competencies and (2) acting/having knowledge. The competencies have three levels: level A is below the level a resident should achieve in respect to the four-year programme; level B is in concordance with the programme; and level C is above the level expected. The second area of training ‘acting/having knowledge’ has five levels: level 1 reflects that the resident has knowledge; level 2, the resident acts under direct supervision; level 3, the resident acts under global supervision; level 4 the resident acts independently without supervision; and level 5, the resident is able to supervise and teach this item to others (Table 1). These levels are a variance of the pyramid of Miller: 1st level, knows; 2nd level, shows how; 3rd level, shows how; and 4th level, does. 10
During training, feedback is given to the resident according to their level of competence and level of acting/having knowledge. New teaching goals are set and re-evaluation is performed to reach higher levels, for example ‘level B-C 4’, for all aspects of the theme chart. After completing the training programme in a hospital or rehabilitation centre, the resident must be able to prescribe prostheses for all levels of lower limb amputation (level 4). Prescriptions must be based on ICF goals which are relevant for the expected activity and participation levels of the individual with amputation.
To facilitate use of the ICF in everyday clinical practice and research, ICF core sets have been developed that focus on specific aspects of function that are typical of a particular disability. The ICF core sets are designed to translate the benefits of the ICF into routine clinical care. Currently, however, no core sets are available for amputation. 11
Key points
The ICF model is an education and analysis instrument for functioning within different diseases. The model can be used in education of residents of PM&R to help with understanding the relationships between disease and functioning. ICF core sets should be developed for persons with a lower extremity amputation. These core sets can then be used in education and research, not only for residents in PM&R but all members of the multidisciplinary team.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.