
Abstract
Amputation is a common late stage sequel of peripheral vascular disease and diabetes or a sequel of accidental trauma, civil unrest and landmines. The functional impairments affect many facets of life including but not limited to: Mobility; activities of daily living; body image and sexuality. Classification, measurement and comparison of the consequences of amputations has been impeded by the limited availability of internationally, multiculturally standardized instruments in the amputee setting. The introduction of the International Classification of Functioning, Disability and Health (ICF) by the World Health Assembly in May 2001 provides a globally accepted framework and classification system to describe, assess and compare function and disability. In order to facilitate the use of the ICF in everyday clinical practice and research, ICF core sets have been developed that focus on specific aspects of function typically associated with a particular disability. The objective of this paper is to outline the development process for the ICF core sets for persons following amputation. The ICF core sets are designed to translate the benefits of the ICF into clinical routine. The ICF core sets will be defined at a Consensus conference which will integrate evidence from preparatory studies, namely: (a) a systematic literature review regarding the outcome measures of clinical trails and observational studies, (b) semi-structured patient interviews, (c) international experts participating in an internet-based survey, and (d) cross-sectional, multi-center studies for clinical applicability. To validate the ICF core sets field-testing will follow.
Invitation for participation: The development of ICF Core Sets is an inclusive and open process. Anyone who wishes to actively participate in this process is invited to do so.
Keywords
Introduction
The International Classification of Functioning, Disability and Health (ICF)
The ICF defines components of health and some components of well-being. It was developed by the World Health Organization (WHO) to provide a unified and standard language and framework for the description of health and health related states. The ICF is used increasingly in various settings within health and in the wider community. It is one of a ‘family’ of international classifications developed by the WHO for application to various aspects of health as a framework for coding a wide range of information about health. It uses standardized common language permitting communication about health and healthcare across the world in various disciplines and sciences.
The classification is divided into two main subdivision: Functioning and Disability as well as Contextual Factors.
The components of the part Functioning and Disability are: Body Functions and Structures, where body functions are defined as the physiologiocal functions of the body systems (including psychological functions) and body structures are defined as anatomical parts of the body such as organs, limbs and thier components and, Activities and Participation, where activity is defined as the execution of a task or action by an individual and participation is involvement in a life situation. Activity limitations are difficulties an individual may have in executing activities and participation restrictions are problems an individual may experience in involvement in life situtions.
The components of Contextual Factors, which represent the complete background of an individuals life and living, are environmental factors and personal factors. Environmental factors make up the physical, social and attitudinal environment in which people live and conduct their lives. They are external to the individual and may have a positive or negative influence on the individuals performance as a member of society. Personal factors, refer to the particular background of an individual's life and living, including gender, age, lifestyle, habits etc are not classified in ICF.53
Amputation
Amputation refers to the surgical or spontaneous partial or complete removal of a limb or projecting body part covered by skin. This generally occurs in the transverse plane, but may be in the longitudinal plane if part of a limb is removed. The incidence and prevalence of amputation is difficult to determine precisely internationally for numerous reasons including: Multiple pathological aetiologies culminating in amputation, Various definitions of clinically significant amputation, Multiple amputations performed in the same individual on the same limb, but at sequentially more proximal levels, and Underlying difficulty and incompleteness of retrospective data collection in many of the studies.1-4
In Europe the prevalence seems to lie somewhere between 17 and 30 per 100,000 with very limited data being available for international comparisons and no current worldwide monitoring.5,6 Non-industrialized countries generally have a higher incidence due to a higher rate of war, trauma and less developed medical systems etc.7 The mortality rate is strongly influenced by the high incidence of comorbidities especially in the person with an amputation resulting from dysvascular causes.8 There are considerable differences in predominant aetiology depending on geographic location. Peripheral vascular disease, either primary or secondary to diabetes, is the most common cause for amputation in the industrialized countries. Trauma is the most common cause in the non-industrialised countries.1 The number of international as well as internal disputes and the continued use of landmines as well as the increased use of motorised transportation has resulted in a significant increase, (more than doubling from 1980–1995) in the incidence of traumatic amputations worldwide.9 The predicted continued high levels of conflict worldwide will result in an increasing prevalence of persons with an amputation, equating to an increase in the number of persons with chronic disabling conditions.
Consequences of amputation
In the acute setting, long-term functional outcomes after lower limb amputation are not easy to predict accurately. Better functional outcomes correlate to a younger age group, better general health in particular cardiovascular health, fewer comorbidities, higher pre-amputation ambulatory ability, transtibial rather than transfemoral amputation, and an environment which is wheelchair and disability friendly.10-12 The actual functional outcomes of contemporary upper limb prosthetic fitting have not been quantified and this greatly restricts the ability to prognosticate regarding expected vocational outcomes and eventual quality of life.13 An important basis for the optimal acute and long-term management of amputees is an in-depth understanding of the patient and the functional consequences of the amputation, systematic and detailed consideration of the patient and their environment and sound measurement of functional outcomes for the different sites and levels of amputation.
Limb amputation results in significant alterations of Body Functions and Body Structures. There is the physical loss of a body part as well as the closely related effects of the underlying aetiological disease, comorbidities or concurrent injuries. These effects may be localized to the affected limb or may involve other body structures as well. Treating underlying conditions may have a considerable impact on the body functions while prosthetic fitting may, at least partially, compensate for the loss of body structures and function of the affected limb(s); especially the lower limb(s). Persons with an amputation may also often experience phantom sensation and phantom pain and this may affect their function.14,15 In the long term, there may be changes related to localized muscle atrophy and altered mechanics of mobilization.16-18 Psychological, social and sexual issues also impact significantly on the overall function of the person with an amputation, but are currently, generally managed less well than physical or functional issues.19
Persons with amputation may experience a wide range of activity limitations and participation restrictions. The typical spectrum of activity limitations and participation restriction relate to self care and extended self-care activities as well as mobility for lower limb amputees.20 Consequently this affects the ability to return to and maintain work,21,22 maintain social relationships, participate in leisure activities and be active members of the community.23 Participation restrictions that a person with amputation may experience are also dependent on environmental factors as well as personal factors such as age, sex, level of education and ability to adjust.24,25 For persons with lower limb amputation, barriers in the community are particularly related to physical/structural environment.25 For persons with upper limb amputation, restrictions are more diverse, reflecting the broad range of activities in which we require manual dexterity, partially depending on the level of the amputation.26-28
Measuring consequences of amputation
A wide range of instruments is used in research to measure health, psychological and social functioning, well-being and life satisfaction of persons with amputation.29-31 Commonly used instruments to measure quality of life include the Short Form 36 (SF-36) and its abbreviated version, Short Form 12 (SF-12),32,33 the Sickness Impact Profile (SIP), and its shortened version, containing 68 items (SIP68) and the Prosthesis Evaluation Questionnaire (PEQ) measuring prosthetic-related quality of life.31 Generic measures of mobility that are used in the assessment of the amputee are the timed walking test34 and the timed get up and go test35 as well as amputee specific mobility scores such as Locomotor Capabilities Index (LCI) and the amputee mobility predictor with prosthesis (AMPPro). Self Care function has been measured most commonly by generic measures such as the Functional Independence Measure or the Barthel index.36,37 Amputee specific measures of function include the amputee activity score, which is specifically for outpatients fitted with a prosthesis.37
In a recent review of lower limb prosthetic outcome measures, it was concluded: Specifically in the field of amputee and prosthetic rehabilitation, there has been a parallel increase in the use of outcome measures; however, there are a multitude of measures currently being used by researchers and clinicians, and there currently is no consensus regarding the most appropriate, or gold standard, measure or measures in this field. Further, it is important to be able to distinguish between outcome measures that have adequate evidence and statistical estimates of validity and reliability and those that lack such evidence. An evidence-based approach to selecting outcome measures involves making judgments about the quality of the validity and reliability studies, interpreting the findings, and deciding whether they are applicable to one's specific practice.30
Similar conclusions can be made regarding outcome measures for persons with amputation of the upper limb.
Reasoning for developing ICF Core Sets
The current classification systems and outcome measurements are useful but are not comprehensive and do not fully encapsulate human functioning and activity limitations for patients with amputations. At best they capture a limited amount of information regarding the patient's functional status, when a fuller description would better enable patient classification, prognostication, and estimation of other parameters regarding the patient and their progress.
Often the information is captured in ‘data silos’ in which assessment data acquired in one episode of care cannot be carried across to the next phase or the next episode of care involving a different clinical focus. To compare data across diseases and interventions, across various health and community settings and on an international basis we need a common framework and language. The ICF makes it possible to link together data across settings, conditions and interventions, making for more efficient, transparent and cost effective healthcare, and serving as a ‘Gold Standard’.38 With the approval of the ICF39 by the World Health Assembly, there is now a comprehensive and universally accepted framework to classify and describe functioning, disability and health in persons with all kinds of diseases or conditions, including limb amputation. With the ICF, the patient experience, including body functions and structures and activities and participation becomes the central perspective. Patients' functioning is now seen as associated with, and not merely as a consequence of a health condition. Functioning and health are considered not only in association with the underlying health condition but also in association with personal and environmental factors.40
Completeness and exhaustive detail are essential traits of an international language of functioning and disability, however not every user of the ICF will require the range and detail that the ICF provides. Clinicians, for example, who wish to apply the bio-psycho-social model to their daily practice, will require only a fraction of health and health-related states classified in the ICF. Realizing that the significance and power of the ICF lies in its conceptualization of functioning and disability, there is a need for creating ICF-based instruments that are more appropriate to clinical information requirements.41 The ICF Core Sets are responding to this need.38 To date, ICF Core Sets have been developed for 15 chronic conditions (Table I)40,42,43 and others are currently being developed. To address the need for interventions in a specific setting, separate ICF Core Sets have been developed for use in the acute hospital and early post-acute rehabilitation facilities.44-46 Recently work has been carried out to demonstrate that ICF Core Sets can also be used as an outcome measure and this may also be a longer term benefit of ICF Core sets for amputees.47,48
The 15 chronic conditions ICF Core Sets have been developed for to date.
Objective
The objective of this paper is to outline the proposed development process for the ICF Core Sets for Amputees and to invite clinical and consumer experts to actively participate in this process.
Developing ICF Core Sets for persons with an amputation
The plan to develop ICF Core Sets for persons with limb amputation was derived in numerous meetings, discussions and subsequent correspondence with clinicians and experts particularly in the second half of 2007 and in early 2008. These discussion involved members from the ICF Research Branch of the WHO Collaboration Centre of the Family of International Classifications, Germany, representatives of the International Society for Prosthetics and Orthotics, and numerous other interested clinicians. An open meeting was convened in Bruges, Belgium, in conjunction with the meeting of the board of ISPMR and the European Congress of Physical and Rehabilitation Medicine. Invitations to this meeting were also extended to all at the first Asian Oceania Society of Physical Medicine and Rehabilitation meeting in Nanjing, China. Starting points agreed on during these discussions and issues to be resolved at a later stage are described in this paper. Some of these preliminary decisions may need further consideration and refinement as the work progresses. The project has been approved by the Human Research Ethics Committee, of Sydney South West Area Health Service, Western Zone.
What types of ICF Core Sets need to be developed?
A key issue when developing ICF Core Sets for amputees is the decision of what core sets should be developed, i.e., for which situation and which purpose. The congenital amputee has a different progression to the adult amputee and while there are overlapping goals and treatment aspects, the time frames and associated conditions tend to be considerably different. Therefore initial rehabilitation of the person with a congenital limb deficiency is not included in the scope of this ICF proposal. The long-term issues of the person with a congenital limb deficiency would however be similar to those of other amputees and could be included in the ICF Core Set for the long-term context.
Adult amputees are a diverse group of patients, from the point of view of both aetiological factors and variable activity limitations of the condition secondary to site and level of the amputations. ICF Core Sets for amputees need to address the variable consequences of amputation as well as the progress of the amputee patient from the acute episode through the stages of recovery and return into integrated community living as well as long term ongoing management. The ultimate configuration of the ICF Core Sets for amputees will be determined by the steering group as the project develops. It would be ideal to have one comprehensive Core Set for all amputees. This comprehensive Core Set would include all ICF categories relevant to persons with an amputation; however, this may prove to be too cumbersome and too extensive to be clinically useful and shorter versions, i.e., brief ICF Core Sets could be useful in clinical practice, but not describe the conditions as comprehensively. Alternatively a ‘common’ ICF core set module, with other modules addressing specific phases of treatment, specific subgroups of people with amputation may be a potential solution. Development of a brief core set that could be integrated easily in routine clinical practice should also be considered. Considerations that need to be taken into account are discussed in the subsequent sections.
The acute context
Patients who undergo amputations are generally first treated in the acute context by trauma, vascular, orthopaedic or surgical services or in rehabilitation clinics with special facilities for acute care. They have particular issues related to the acute management, wound healing and other issues relating to their primary disease.
The early post acute context
Early rehabilitation of the person with an amputation is quite variable. Following an amputation persons require specialized rehabilitation care. In addition to this, they also need ongoing surgical, medical and nursing care.
The long-term context
The long-tem functional, activity and participation issues are present from the time of amputation and in many cases, especially the vascular amputees; some of these issues are already present prior to surgery. This may therefore serve as the ‘common’ module for all persons with an amputation.
The site of amputation
Functional consequences of persons with upper and lower limb amputation are significantly different. The functioning of patients also varies with the level of the amputation as well as the type of prosthetic aid used. In view of the diversity of specific issues related to the amputee and the diversity of comorbidities encountered in patients with amputation none of the currently developed Post-Acute ICF Core Sets for Neurological, Musculoskeletal or Cardiopulmonary Conditions 49-51 would be appropriate.
Methods to be used in the ICF Core Set development
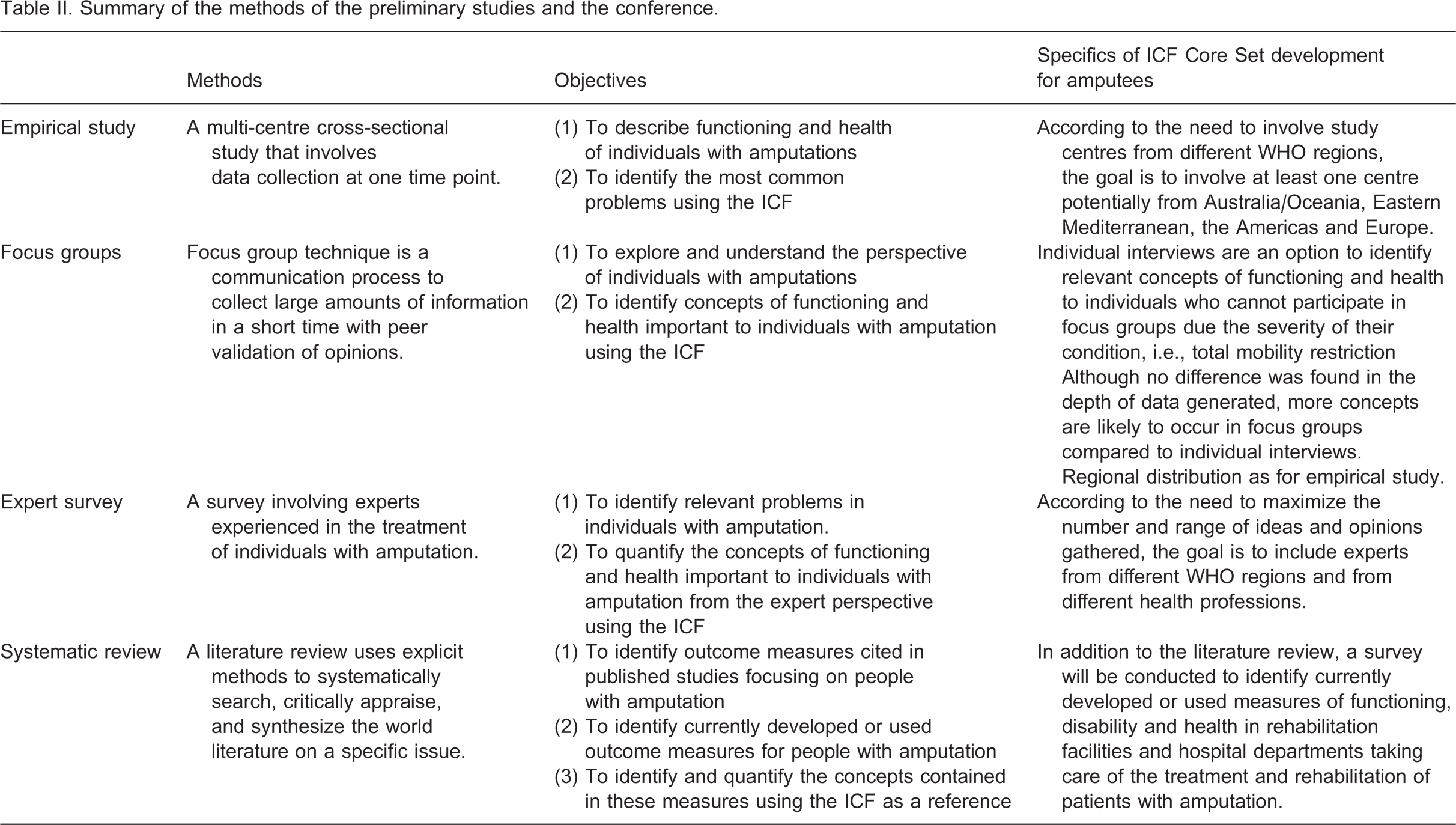
The development of ICF core sets can be considered in three phases: Preparatory phase; core set development; testing and validation. In the preparatory phase of the project, all relevant perspectives will be addressed by: (a) researchers, (b) patients and (c) clinical experts. In the last component of the preparatory phase (d), the applicability of the ICF in typical clinical situations will be tested. (See Table II) A systematic literature review will identify and quantify the concepts underpinning the currently published and developed outcome measurements. Studies are selected through pre-defined inclusion and exclusion criteria in broad literature searches to capture the relevant research. The underlying concepts in the outcome measures will be linked to ICF categories using standardised linking rules.52
The patient interviews explore the concepts of functioning and health important from the perspective of the individual with an amputation. These may take place in a focus group or individually. The underlying concepts are then linked to ICF categories. The expert survey will be an electronic survey of clinical experts to identify their perspective of relevant problems for an individual with an amputation and to quantify these concepts of functioning and health. The survey aims to include experts from all WHO regions and all health professionals groups involved in the treatment of amputees. The empirical study will be a cross sectional multi-centre study using an extensive ICF check list to identify the most common problems and describe function and health in an amputee population.
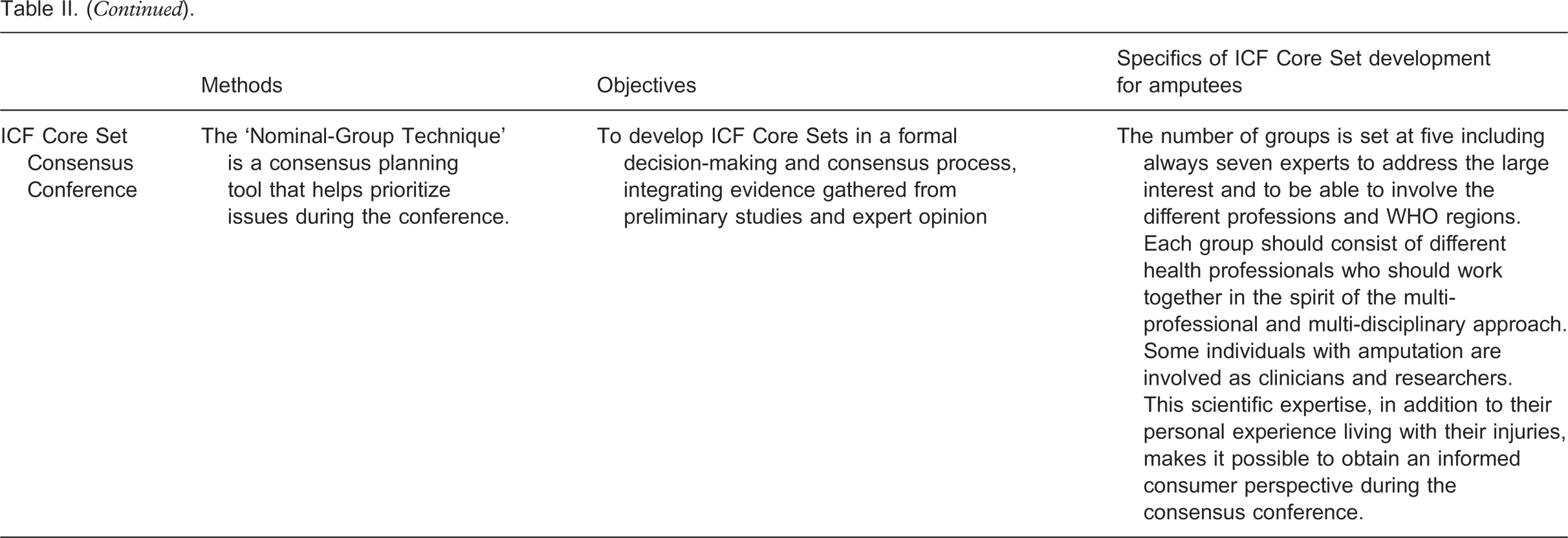
The final result of the preparatory phase will be an extensive and all inclusive list of ICF categories. This list will include the perspectives of the literature, patients, clinical experts as well the findings of the empirical cross sectional study. In a consensus conference which includes a broad range of international representatives the ICF categories derived from the preparatory phase are then discussed in detail over numerous iterations until consensus is reached about which categories should be included in the core sets. A detailed description of the process is found in the paper: ‘Development of ICF Core Sets for patients with Chronic Conditions’.40
Summary of the methods of the preliminary studies and the conference.
The ICF Core Sets for persons with an amputation will be defined at an ICF Core Set Consensus Conference which will integrate the information gained from the above process to develop internationally accepted ICF Core Set(s).
Figure 1 shows a summary of the time schedule for the ICF Core Set development for amputees. The final phase of the development of initial ICF Core Sets is the testing and validation phase which will be carried out in international multicentre studies.
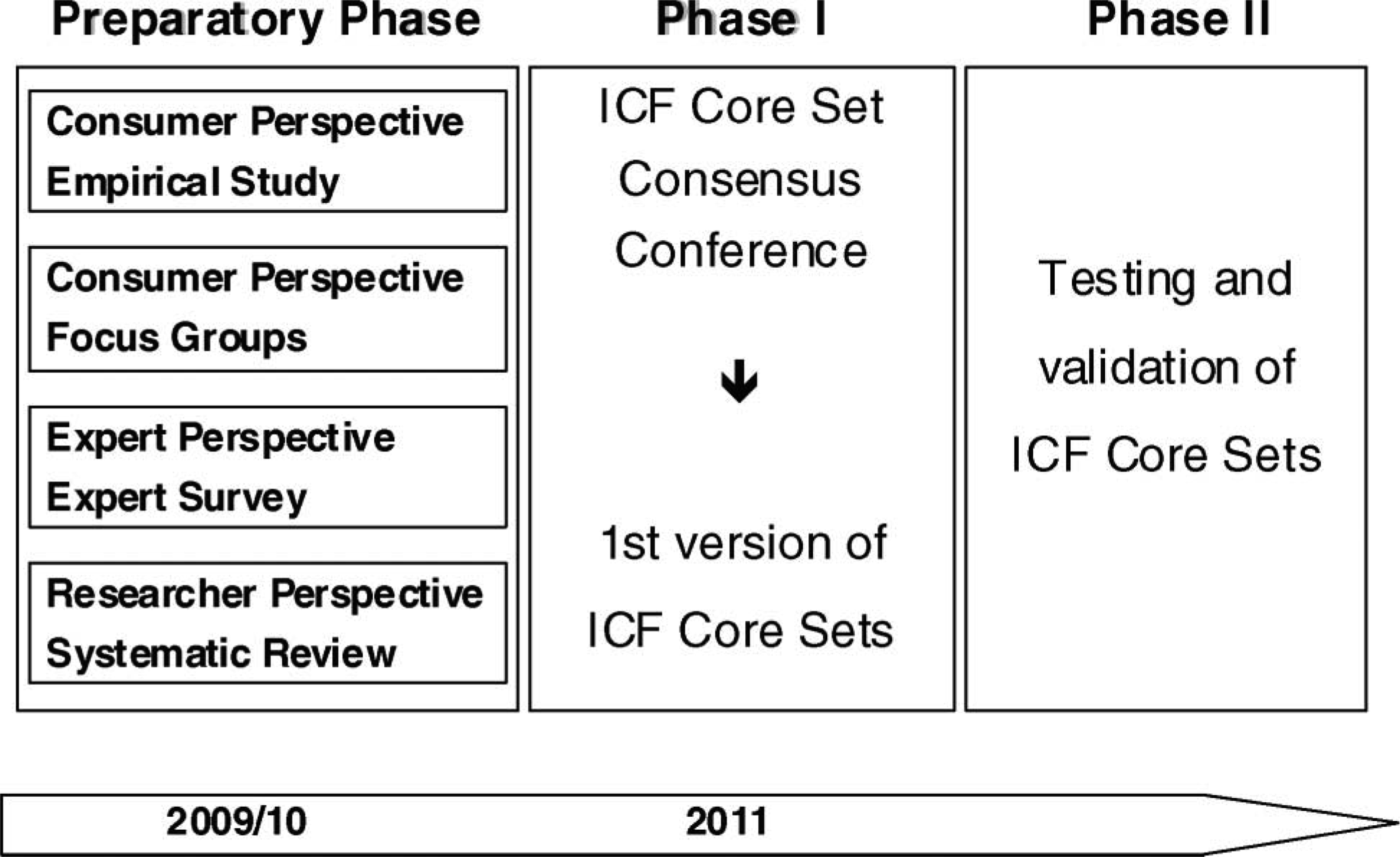
Time schedule of the development process of ICF Core Sets for persons following amputation.
As the development of ICF Core Sets for persons with an amputation must result in practical tools, the ICF Core Set Consensus Conference will primarily involve health professionals from different parts of the world. The maximum number of experts attending the conference will be set at 35 (five groups of seven persons), which is considered necessary to address the broad interests and include the different professional groups and regions of the world. It is important, that each group should consist of different health professionals who will work together in the spirit of partnership and the multi-professional and interdisciplinary approach, which is typical for care and research for persons with amputations. However, when inviting experts to the conference, the Steering Committee will need to ensure that members are sufficiently fluent in English to be able to contribute to the process.
Logistics
The project will be a cooperative effort of the ICF Research Branch of the World Health Organization (WHO) Collaboration Centre of the Family of International Classifications (DIMDI, Germany), the Classification, Assessment and Terminology (CAT) team and the Disability and Rehabilitation (DAR) team at WHO, the International Society for Prosthetic and Orthotics (ISPO) and the International Society for Physical and Rehabilitation Medicine (ISPRM) and their partner institutions across the world. The steering committee for the process will consist of two Chairs: Friedbert Kohler, President of ISPO Australian National Member Society and Chair of the ICF Special interest group of the Australasian Faculty of Rehabilitation Medicine, and Gerold Stucki for the ICF Research Branch Munich, Germany. The other members are the co-authors of this paper.
Discussion
ICF Core Sets are practical tools for different purposes. They allow clinicians and researchers to classify and describe individual's functioning by using the most relevant ICF codes. The Brief ICF Core Set may facilitate international studies and studies comparing the consequences of different conditions. The Comprehensive ICF Core Set can be used in the clinic as a checklist to assess patient's needs, to formulate rehabilitation goals and to evaluate progress. A general reference framework is powerful with regard to communication between health professionals within specific settings and between settings. Similarly it may be useful when communicating between health professionals and persons with amputation.
The goal of the ICF Core Sets to specify what is relevant to study and report for persons with amputation is very much in line with the broader goal to define a Core Data Set of variables that can be collected in any study in persons with amputation, as well as various Basic and Extended amputee Data Sets and Modules for specific topics related to persons with amputation. As in any scientific endeavour, there are uncertainties that have to be resolved during the process. As mentioned, the preliminary studies will provide the necessary information to guide decisions on: (a) which type of ICF Core Sets for amputees to proceed with, and (b) necessary stratification by a number of variables, e.g., between persons with different sites and levels of amputation. Active contributions by the amputee community to the preliminary studies and the ICF Core Set Consensus Conference will be essential to make this project successful. It is important to realize that the ICF Core Set Consensus Conference will provide only a first, best possible version of ICF Core Sets for persons with an amputation, which will then need to be tested worldwide.
Invitation for participation
The development of ICF Core Sets is an inclusive and open process. Therefore, the authors of this paper encourage clinical and consumer experts to actively participate in the process. Anyone who wishes to actively participate in contributing to any of the phases as delineated in the methods section is invited to contact Dr Friedbert Kohler at