
Abstract
Background: Although many core sets of measurement concepts have been published in the literature, this has not been done for the field of lower limb orthoses.
Objectives: This paper provides an overview of the measurement concepts that are relevant in lower limb orthotic evaluations, and it proposes a candidate Core Set of outcome measures to be used in clinical studies on ankle-foot orthoses (AFOs) and knee-ankle-foot orthoses (KAFOs).
Study Design: Literature review.
Methods: The International Classification of Functioning, Disability and Health (ICF) was used as framework to select relevant concepts.
Results and conclusion: Measurement concepts covering all ICF levels of functioning were identified as relevant for the Core Set, including functions of the joints and bones (b710–b729), muscle functions (b730–b749), gait pattern functions (b770), walking (b450), moving around in different locations (d460), and daily-life functioning (d5–d9). Further validation of this candidate Core Set through a formal decision-making process is needed to obtain consensus among experts in the field. Based on such a consensus, the next step will be to systematically review the literature and identify those measurement instruments that are best suited to assess the proposed concepts, based on their psychometric properties in a given sample and context. Thereafter, we suggest that this ICF Core Set of measurement instruments should be applied in orthotic studies on AFOs and KAFOs in ambulatory patients with gait problems.
Although many ICF Core Sets have been published, this has not been done for the field of lower limb orthoses. We feel that such a Core Set is urgently needed, to enable comparison of results, and establish evidence on the efficacy of orthotic treatment, which will improve patient care.
Background
Lower limb orthoses are often applied to improve standing and walking in patients with various medical conditions affecting the neuromuscular and musculoskeletal system. With an estimated 1.6 million users merely in the USA, 1 the application of lower limb orthoses is high. Given this large scale of use, and the importance of orthotic devices to promote mobility, reliable information on their effectiveness is essential. However, in current practice, the prescription of lower limb orthoses is largely based on clinical experience, whereas evidence-based knowledge, based on studies using proper outcome assessments is lacking.2–7 This lack of evidence is also reflected by a scarcity of prescription guidelines,8–12 which often results in poor clinical decision making, and, therewith, in suboptimal orthoses. 13 Therefore, (multi-centre) clinical studies on lower limb orthoses, involving large numbers of patients and using similar measures of outcome are needed to provide solid evidence for clinical practice.
As proposed by Harlaar and colleagues, 14 the effects of lower limb orthoses on a patient's functioning need to be evaluated at two levels; i.e. at the mechanical level, expressing the correct functioning of the orthosis, and at the activity level, expressing the gain for the patient. Most orthotic studies, however, predominantly evaluate the mechanical contribution of the orthosis to the wearer's gait.15–19 Although these intervention-related evaluations are important, they may not always be clinically relevant, and do not capture the patient's perspective. For example, 3D-gait analysis explicitly quantifies changes in joint kinematics and kinetics during gait, but it does not provide information about the effects on standing and walking activities, nor on the patient's functioning in daily life. Both from the viewpoint of the researcher and the patient, evaluating multiple aspects of a persons’ functioning should be considered as fundamental to the design of studies on lower limb orthoses.14,20
To assemble a common set of outcome measures, a so-called Core Set, 21 as a minimal required standard in orthotic studies, the prime measurement concept(s) should be defined, prior to choosing specific instruments to evaluate these concepts. In this paper, we provide an overview of measurement concepts that are relevant in lower limb orthotic evaluations, based on the International Classification of Functioning, Disability and Health (ICF); 22 we clarify our preferences for selecting these concepts, and we propose a candidate Core Set for use in orthotic studies on ankle-foot orthoses (AFOs) and knee-ankle-foot orthoses (KAFOs).
Methods
For proposing a candidate Core Set that captures multiple aspects of functioning, the ICF 22 was used. According to the ICF, measurement concepts can be separated into two components of human functioning: i.e. the component ‘body functions and structures’ and the component ‘activities and participation’. With regard to ‘activities and participation’ the World Health Organization distinguishes two qualifiers: the ‘capacity’ qualifier, describing an individual's ability to execute a task or action in a standardized environment, and the ‘performance’ qualifier, which describes what an individual actually does in their current environment. The ICF also includes the components ‘personal factors’ (e.g. coping style, gender) and ‘environmental factors’ (e.g. social attitudes, and climate or terrain), which may act as barriers or facilitators.
Using the ICF as reference, an overview is given of concepts that are considered as most relevant for lower limb orthotic evaluations. Hereby a distinction is made between intervention-related concepts, which relate to the efficacy of the orthosis (i.e. does it work under controlled, optimal conditions), and patient-relevant concepts, relating to the effectiveness of the intervention (does it work for the patient). In addition, examples are given of instruments that can be used to measure these concepts. This list of examples is not exhaustive, and, moreover, the suitability of the instruments is dependent on the psychometric properties in a given sample and context, which should be investigated in future research. Finally, a candidate ICF core set is proposed for use in orthotic studies on AFOs and KAFOs in ambulatory patients with gait problems.
Results
ICF-component – body functions and structures
With regard to the ICF-component of body functions and structures, several outcome measures can be used to cover a variety of relevant concepts (Table 1). These concepts are mainly intervention related, and they predominantly associate with the domain of neuromusculoskeletal and movement-related functions (b7) (e.g. functions of the joints and bones (b710–b729), muscle functions (b730–b749), and gait pattern functions (770)). Patient-important concepts related to this ICF-component may be at the second level categories of pain (b280–b289) and/or exercise tolerance functions (b455).
Functions of the joints, bones and muscles
Many conditions of the neuromusculoskeletal system will be brought to the physician's attention because of gait abnormalities. 23 In order to appreciate these abnormalities, it is key to become familiar with the patient's impairments in joint, bone and muscle functions.24,25 For optimal orthotic management, awareness of these motor function deficits is required, as it will allow the physician to better differentiate primary impairment from substitutive actions. 26 A tool that is commonly used for the assessment of joint, bone and muscle functions is the physical examination. Generally, a physical examination comprises various elements of assessment, including testing range of motion (e.g. with goniometry), muscle strength (e.g. with manual muscle testing or hand-held dynamometry) and muscle tone (e.g. with the Ashworth scale). For specific conditions, a more extensive assessment may be needed, including testing reflexes and control of movement.
Gait pattern functions
Because the physical examination does not provide sufficient information on the patients’ impairments, additional assessment of the gait pattern is warranted. This allows the physician to clearly identify the deviations to be addressed with the orthosis. This is a complex process, and observation of the gait pattern functions can be extremely helpful in determining what changes at the joint level are required to provide stability and support for ambulation. Especially the use of 3D-gait analysis has proven to be a particularly powerful instrument to explicitly quantify the gait pattern in terms of joint kinematics and kinetics. 27 It can be used as a tool for clinical decision making, but also for orthosis evaluation. In this context, evaluating orthotic interventions at the level of gait kinematics and kinetics can be regarded as a technical quality check of the orthotic intervention itself. 14 Especially for complex clinical questions, and for scientific purposes, measuring this construct has shown its value. 28 Examples of gait parameters that have been shown useful in evaluating orthoses are the knee angle in midstance,13,29 (timing of) peak ankle moment in terminal stance 28 and ankle dorsiflexion in terminal swing.30,31
Pain
Pain is a common complaint resulting from deviations in the gait pattern.25,32– 35 Although it can have variable causes, it is mostly associated with overload of muscles, tendons or joints of the affected lower limb.25,26 In medical conditions with an asymmetric distribution, such as polio or spastic hemiplegia, pain may not only be present in the muscles or joints of the affected lower limb, but also in the contralateral limb. Appropriate orthoses may be helpful in reducing pain, by stabilizing one or more joints or by restricting painful motion. 35 Pain ratings, for example assessed using the Visual Analogue Scale (VAS), or the pain-subscale of the 36-Item Short-Form Health Survey (SF36), 36 can be taken pre-/post-intervention to evaluate whether the orthosis was effective in reducing pain.
Exercise tolerance functions
Deviations in the gait pattern may also result in impaired exercise tolerance functions. According to the ICF, exercise tolerance functions are defined as ‘functions related to respiratory and cardiovascular capacity as required for enduring physical exertion’. These include functions of physical endurance, such as walking efficiency, and fatigability. Walking efficiency in patients with gait deviations has been shown to be typically lower, when compared to normal gait. 37 – 43 Consequently, this may result in complaints related to severe fatigue. Both the degree of lower extremity muscle weakness41,44 and reduced ankle and knee joint ranges of motion are strongly associated with the reduced walking efficiency.31,40 In these instances, orthoses that substitute for loss of muscle function or reduced lower extremity joint motion may be effective in improving walking efficiency and the associated energy cost (EC) of walking.40,41 Measurement of walking EC with ambulatory gas-analysis systems can provide valuable information regarding treatment impact.13,28
ICF-component – activities and participation
Measurement concepts relevant to lower limb orthotic evaluations of ankle-foot orthoses and knee-ankle-foot orthoses in ambulatory patients with gait problems based on the International Classification of Functioning, Disability and Health (ICF).
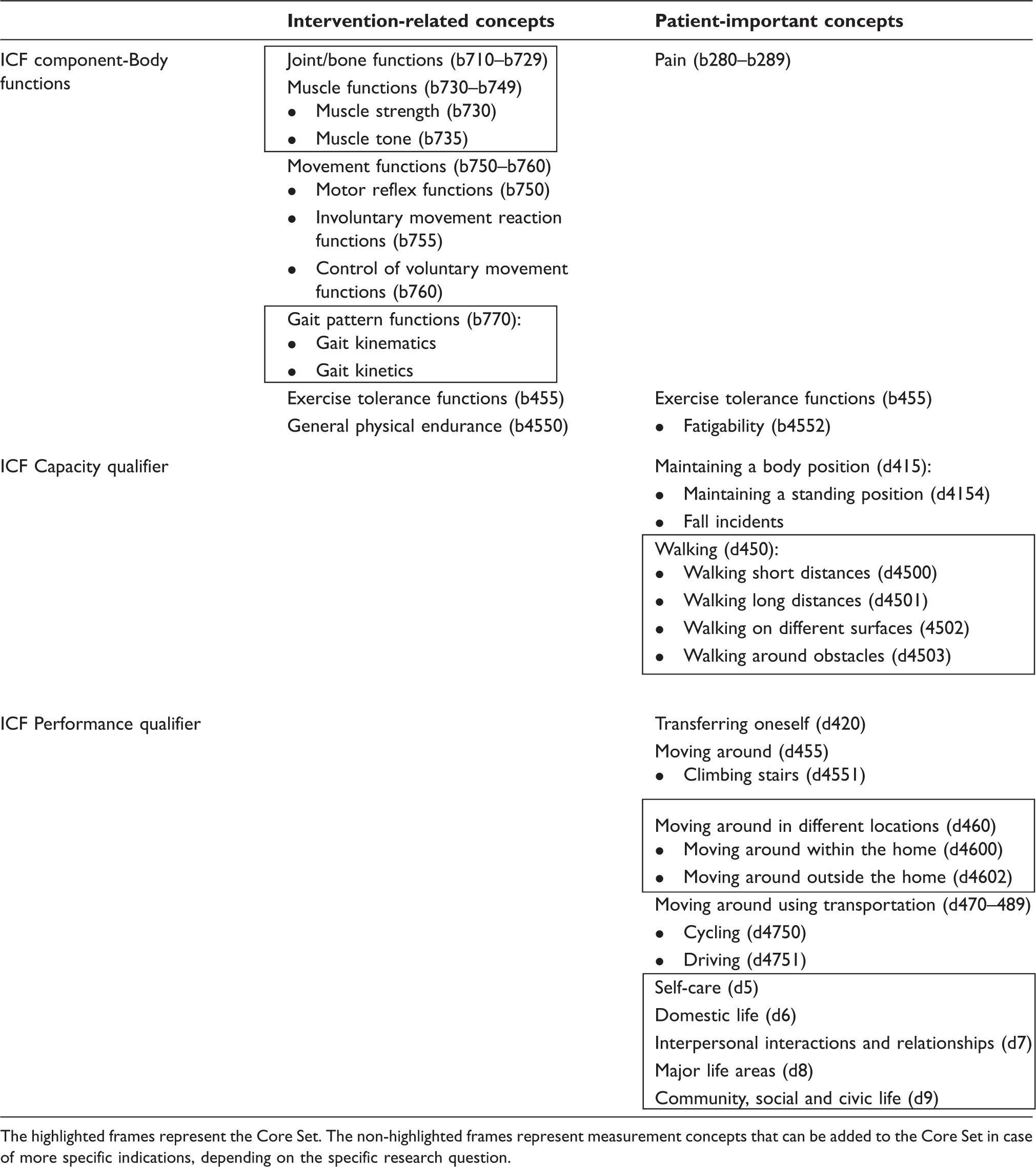
The highlighted frames represent the Core Set. The non-highlighted frames represent measurement concepts that can be added to the Core Set in case of more specific indications, depending on the specific research question.
Maintaining a body position
Concepts linked to the second level category of maintaining a body position commonly relate to standing problems, e.g. instability. Instability during standing can be caused by lower extremity muscle weakness, abnormal movement synergies and/or spasticity, and often contributes to increased fall risk and consequent decreased independence in activities of daily living.45,46 For this indication, an orthosis might be beneficial in providing stability during stance.19,47,48 To determine whether the orthosis was effective for this purpose, static and dynamic balance measures can be taken before and after intervention. Instruments that can be used for this include the Berg Balance Scale, 49 the timed up and go test, 50 as well as static and dynamic posturographic tests. 51 Furthermore, registration of fall incidents may be informative.
Changing a basic body position and transferring oneself
Changing a basic body position incorporates changing from lying down, from squatting or kneeling, and from sitting or standing (and vice versa). This includes getting up out of a chair to lie down on a bed, or moving to a toilet seat, bike seat (i.e. getting up and down on a bike), or car seat (i.e. getting in and out of the car). The ICF defines transferring oneself as ‘moving from one surface to another, such as sliding along a bench or moving from a bed to a chair, or from a chair to a toilet seat without changing body position’. Using an orthosis may enable these activities. However, inevitably, they may also be hampered by the orthosis, due to the requirements for orthotic design. These aspects of changing a basic body position and transferring oneself should be systematically addressed before an orthosis is provided and should be evaluated afterwards, for example with the ACTIVLIM questionnaire. 52
Walking
In addition to providing stability during standing, and enable (safe) transferring, orthoses must also give sufficient comfort for a full day of activities, such as walking and other mobility-related activities. The ICF defines walking as ‘moving along a surface on foot, step by step, so that one foot is always on the ground’. This includes walking short distances (d4500), walking long distances (d4501), walking on different surfaces (d4502), and walking around obstacles (d4503). Since one of the primary functions of an orthosis is to enable walking, it is therefore a clinically relevant activity to evaluate. Important aspects related to this activity include endurance, distance and speed, and these can be assessed with time-scored walking capacity tests, measuring what a person is capable of doing in a standard environment. An example of a capacity-based walking test is the two-minute walk test (2MWT). This test measures walking distance at comfortable speed, and has been recommended as a core qualifier to assess walking capacity in research and clinical practice. 53 Walking speed, measured with the six-minute walk test (6MWT) is also considered a clinically relevant outcome, as it is assumed to reflect walking in daily life.54,55
Moving around in different locations
Since the characteristics of walking under standardized conditions may differ from those in daily life, 56 an assessment of actual walking in the patients’ own environment, i.e. walking performance, is also needed. For the assessment of walking performance, outcome measures related to the second level category of ‘moving around in different locations’ can be used. For example, the amount of walking inside and outside the home can be measured with activity accelerometry. 57 Walking performance or activity performance in daily life can also be assessed with questionnaires, such as with the physical functioning subscales of the SF36 or Nottingham Health Profile (NHP). 58 Especially for assessing the perceived capability by the user of an orthosis to engage in daily-life activities, the use of these and other questionnaires is required. Examples of relevant daily-life activities that can be linked to ‘moving around in different locations’ include the third level category climbing stairs (d4551), cycling (d4750) and driving (d4751).
Domains d5–d9
With regard to the domains d5–d9, concepts related to restrictions in self-care, domestic life, interpersonal interactions and relationships, major life areas, and community, social and civic life are considered relevant. Generally, these concepts are assessed by means of multidimensional questionnaires, such as the Impact on Participation and Autonomy (IPA),59,60 and, for the assessment of participation concepts in children, the Children's Assessment of Participation and Enjoyment (CAPE). 61 These are both examples of generic instruments that can be used for evaluating physical and mental aspects of health status. The advantage of such generic instruments is that they can be used in different populations, enabling comparison of results. A disadvantage may be that such instruments are too generic to capture specific changes in participation. An example of a disease-specific questionnaire is the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 62 which is commonly used in osteoarthritis research. A disease-specific instrument measures health aspects specific to the patient's condition, and might therefore be more helpful in detecting more subtle changes.
ICF-components – personal and environmental factors
Since the success of an orthosis is also dependent on environmental factors and personal factors (the latter are not currently coded within the ICF), such as motivation, aspects related to these ICF-components must also be regarded. The most successful results are achieved in well-motivated patients, who perceive their functional limitations as severe, walk regularly, and are able to adapt their gait pattern to the use of an orthosis. 35
Discussion
The primary aim of this paper was to provide an overview of measurement concepts that are relevant to orthotic evaluations. Using the ICF as a reference, relevant concepts at all levels of functioning were identified. These concepts have been described extensively in patients with neuromuscular skeletal disorders. 24 –26,35,63 The proposed concepts are also in accordance with the ICF Core Sets that have been published for patients with neurological conditions64,65 and musculoskeletal conditions 66 in early post-acute rehabilitation facilities. Patients with these conditions are typically characterized by impaired joint and muscle functions, deviations in the gait pattern, pain and limited mobility, leading to restrictions in activities of daily living. 26 According to the consensus reports of the International Society for Prosthetics and Orthotics (ISPO), 8 – 10 primary orthotic treatment goals in patients with these conditions are therefore aimed at prevention or correction of deformities, and at improving gait, mobility and independent and safe performance of daily activities.
Taking each of these treatment goals into account, 8 –10,35,43 it is suggested that a candidate Core Set of outcome measures for use in orthotic trials should cover all ICF levels of functioning, thereby allowing the mechanical assessment at the body-function level to take the role of explaining the result at the activity and participation levels, i.e. ‘it creates explaining evidence on the patient/orthosis match’. 14 Therefore, the candidate Core Set should include the following concepts (Table 1, highlighted frames); i) concepts related to the ICF-component of body functions (including ‘functions of the joints and bones’, ‘muscle functions’, and ‘gait pattern functions’), expressing the correct functioning of the orthosis, ii) concepts at the ICF-component of activities and participation measured with capacity qualifiers (such as time-scored walking tests), expressing the gain in the ability to ‘walk’, and iii) concepts at the ICF-component of activities and participation measured with performance qualifiers, expressing what a person actually does in the usual environment, i.e. ‘moving around in different locations’ (measured with activity monitoring and as perceived by the user with questionnaires), and performance of daily-life activities. Including a performance qualifier is required, given the moderate relationships that have been demonstrated between capacity (can do) and performance (do do).56,67 In case of more specific indications, the addition of extra outcome measures to the Core Set can be considered. These can, for example, include measures to evaluate pain, frequency of falls, and exercise tolerance functions (Table 1, non-highlighted frames). Individualized outcome measures, such as the Goal Attainment Scale can also be used to evaluate specific patient problems. Finally, measures of user-satisfaction and adverse effects must be regarded.
Two example assessment sets for evaluating the effect of ankle-foot orthoses.
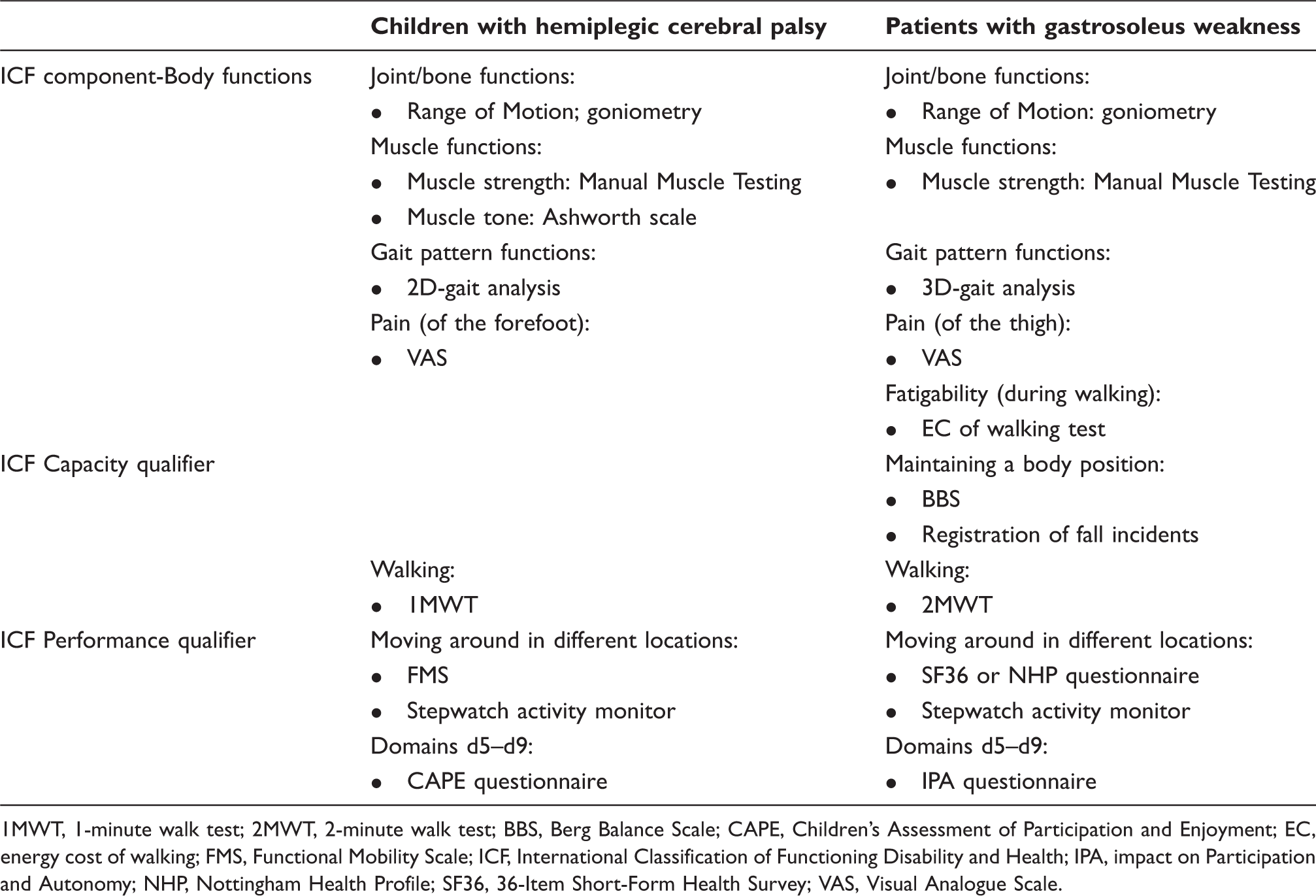
1MWT, 1-minute walk test; 2MWT, 2-minute walk test; BBS, Berg Balance Scale; CAPE, Children's Assessment of Participation and Enjoyment; EC, energy cost of walking; FMS, Functional Mobility Scale; ICF, International Classification of Functioning Disability and Health; IPA, impact on Participation and Autonomy; NHP, Nottingham Health Profile; SF36, 36-Item Short-Form Health Survey; VAS, Visual Analogue Scale.
While selecting an instrument with good measurement properties is important, the test should also reflect the conceptual basis one intends to measure. That is, prior to choosing an instrument, the primary outcome(s) should be defined, depending on the specific aim (i.e. treatment goal) of the study. Without an explicit definition of this goal, it is difficult to decide on the best measurement instrument(s) to address the research question(s). Consequently, this hampers valid outcome assessment.
Conclusion
The use of a Core Set of outcome measures in clinical studies on lower limb orthoses is urgently needed to enhance the evidence base for orthotic interventions. This Core Set should cover all components of functioning, as defined in the ICF, including the functions of the joints and bones, muscle functions, gait pattern functions, walking, moving around in different locations, and daily-life functioning (d5–d9). Within the Core Set, the primary outcome(s) should be defined, depending on the aim of a study. Furthermore, in case of more specific indications, the addition of extra outcomes should be considered. These can include measures to evaluate pain, fatigability and frequency of falls. We propose that such a Core Set of ICF outcomes is applied in orthotic studies on AFOs and KAFOs in ambulatory patients with gait problems, to a) improve the clinical relevance of these studies, b) enable the comparison of obtained results, and c) contribute to establishing evidence on the efficacy of orthotic treatment, as well as to the development of orthotic guidelines, which will improve patient care.
Footnotes
Funding
This work was supported by ZonMw [grant number 14350057]; and the Stichting Kwaliteitsgelden Medisch Specialisten (SKMS) [grant number 7033905].