
Abstract
Background: In Turkey there is no amputee-specific instrument to measure health-related quality of life in lower limb amputees.
Objectives: To evaluate the validity and reliability of a Turkish version of the Trinity Amputation and Prosthesis Experience Scales (TAPES).
Study design: Outcome study to determine test–retest reliability and construct validity of the adapted Turkish version of the TAPES.
Methods: After translation/retranslation of the TAPES, the Turkish version of the TAPES was applied to 47 amputees. A quality of life evaluation (Nottingham Health Profile), a satisfaction evaluation (Satisfaction with Prosthesis), and a functional assessment tool (Amputee Mobility Predictor) were also performed and analysed.
Results: On the basis of retesting, the Turkish version of the TAPES was observed to be reliable. The first domain of the Turkish version, which includes psychosocial adjustment, activity restriction and satisfaction with the prosthesis, was found to be valid. However, the validity of the second domain could not be analysed.
Conclusions: The Turkish version of the multidimensional TAPES survey is valid and reliable in Turkish unilateral lower limb amputees and may be used in clinical situations to assess the needs of amputees.
Introduction
Amputation is a permanent disability associated with functional limitations that restrict an individual’s daily activities. A major goal of healthcare professionals involved in the care of amputees is to minimize the negative effects of this type of disability by using prosthetics and rehabilitation, thereby improving quality of life. However, several factors may affect the success of prosthetics and rehabilitation. These include the cause and level of amputation, duration of prosthesis use, prosthetic design, stump pain, phantom limb sensation, phantom limb pain and psychosocial status. Therefore, assessment of prosthetic and rehabilitation outcomes in the post-prosthetic phase requires the use of a multidimensional test. 1 – 4
Although statistical evidence is lacking, it is estimated that there are about 300,000 amputees in Turkey. Our experience and the profiles of our lower limb amputees indicate that the leading cause of amputation in Turkey is trauma, with traffic accidents being the primary cause. This is followed by train accidents, landmines, electrical burns and disasters such as earthquakes. However, since Turkey forms a bridge between Asia and Europe, the reasons for amputation vary from west to east. In the eastern part of Turkey, which is experiencing ongoing war, traumas resulting from shotguns and landmines are seen more often, whereas traffic accidents are the primary reason for amputation in the western part of Turkey. Amputations due to other major causes, namely peripheral vascular diseases, infections, cancer and congenital limb loss, occur at similar frequencies in both regions of Turkey.
While many assessment tools are in use at present, an empirically supported and universally accepted gold standard assessment tool that allows measurement of amputee rehabilitation and prosthetic outcomes has not yet been established. 5,6 This was the conclusion of a review of amputee-specific follow-up surveys that measured prosthetic usage time and factors related to functional outcome. 5
According to Condie et al.’s 5 classification, the Locomotor Capabilities Index, Locomotor Capabilities Index-5, Amputee Mobility Predictor (AMP), Special Interest Group in Amputee Medicine, and Russek’s classification systems all measure mobility and are used specifically to assess amputees. The Prosthetic Profile of the Amputee, Functional Measure for Amputees, Amputee Activity Score, and Houghton Scale are specific measures of amputee function. In addition, the Prosthetic Evaluation Questionnaire, Orthotics and Prosthetics National Office Outcomes Tool, Trinity Amputation and Prosthesis Experience Scales (TAPES), Body Image Questionnaire, Perceived Social Stigma Scale and Amputation Related Body Image Scale are amputation-specific measures of quality of life.
The outcome measurement tools described in the literature can be divided into three categories: self-report, professional report and performance-based measures. Self-report measurements are preferred because they are easy to use and directly reflect the experience of the patient. The best known self-report tools that have beenused with lower limb amputees are the Amputee Activity Score, Sickness Impact Profile, Reintegration to Normal Living survey, Prosthetic Profile of the Amputee, Nottingham health profile (NHP), SF-36 health status profile, Satisfaction with Prosthesis (SATPro), Prosthetic Evaluation Questionnaire, Orthotics Prosthetics Users’ Survey and the TAPES survey. 5,7,8 The TAPES was developed in 2004 by Gallagher and MacLachlan to assess adaptation to amputation and prosthetics. 1 It is sensitive to the special conditions associated with amputees and analyses adaptation to a prosthesis at a multidimensional level using several subscales, including those measuring psychosocial adjustment, activity restriction, satisfaction with the prosthesis, stump pain, phantom limb pain and other medical problems. 9
The lack of a gold standard tool for assessing the prosthetic and rehabilitation outcomes of Turkish amputees as well as the problem of interpreting many of the existing tools led us to perform a study on this issue. The TAPES survey was preferred in our study for several reasons: it requires self-report and is practical, understandable, suited to the socio-cultural environment of Turkish amputees and widely used in research. 1,5 The present study aimed to determine whether the Turkish version of the TAPES reliably and validly determines the outcome of unilateral lower limb amputation in a group of Turkish amputees.
Methods
Patients
The study included 50 invited adult individuals (>18 years old) who underwent lower limb amputation, completed prosthesis training and rehabilitation, and had been using a prosthesis for at least six months prior to the beginning of the study. The causes of amputation were trauma, congenital deformity, circulatory problems and cancer. None of these causes induced limitations that prevented prosthetic use. All participants provided written informed consent. The study was approved by the Hacettepe University ethics committee. Exclusion criteria were illiteracy and bilateral amputation.
Translation into Turkish
After obtaining permission from the developers of the TAPES, the Turkish version of the instrument was developed. For the translation process we used the recent guidelines for cross-cultural adaptation. 10 Two translations from English to Turkish were performed by two independent translators whose mother tongue was Turkish, allowing detection of errors and divergent interpretations of items with ambiguous meaning in the guidelines for the original instrument. The two translations were then retranslated into English, also blindly and independently, by two native English speakers. Each English translation was then compared with theoriginal English TAPES and checked for inconsistencies.
The Turkish version was then jointly reviewed by a bilingual team, including the four translators, one public health physician and three physiotherapists, to assess the necessity of performing a cultural adaptation for the use of the Turkish version among Turkish amputees. They again compared the Turkish version with the original English version to detect errors of interpretation and nuances that might have been missed. One of the most important issues associated with the translation process was to obtain consensus from the translators regarding terminology. For example, two separate Turkish terms were initially used by the translators to express ‘artificial limb’. Moreover, in the original TAPES survey developed by Gallagher and MacLachlan, the measurement units in the activity restriction subscale are ‘yards’ and ‘miles’. However, in Turkey the metric system is generally used. After discussions between the study investigators and translators, a Turkish version of the TAPES survey that corresponded as closely as possible to the original survey was produced. 10,11
Each subject was asked to complete the Turkish version of the TAPES twice (1–3 days apart). The survey comprises two domains. The first consists of the subdomains psychosocial adjustment, activity restriction and satisfaction with the prosthesis. Psychosocial adjustment comprises three subscales, namely general psychosocial adjustment, social psychosocial adjustment and limited psychosocial adjustment. Each section consists of five items answered with a 5-point Likert-type scale. Activity restriction consists of athletic activity restriction, functional activity restriction and social activity restriction subscales, each of which has three items answered with a 3-point Likert-type scale. Satisfaction with the prosthesis has the following subscales: aesthetic satisfaction with the prosthesis, weight satisfaction with the prosthesis and functional satisfaction with the prosthesis. The weight satisfaction subscale has just one item, which is answered with a 5-point Likert-type scale, whereas both aesthetic satisfaction and functional satisfaction with prosthesis have five items, each answered with a 5-point Likert-type scale. The second domain of the TAPES determines the average duration of daily prosthetic use, general health status and physical capabilities. This domain also identifies other medical problems not associated with amputation. The subdomains of this second domain determine whether any pain is present, how often it is felt, the length of each pain episode, average level of pain and its impact on daily life. The second domain also includes questions regarding pain that are not in the original TAPES survey of Gallagher and MacLachlan. 1
To evaluate the validity of the Turkish version of the TAPES, the NHP, SATPro and AMP surveys were used. The Turkish version of NHP, a generic quality of life measurement tool, has been showed to be a valid and reliable outcome measurement. 12 For this reason it was used to analyse the construct validity of the TAPES. The Turkish version of the NHP (translated by Küçükdeveci) was used with permission. This survey includes the following six subdomains: energy level, physical activities, pain, sleep, emotional reaction and social isolation. The sum of the scores of each subdomain equals 100. 12 The SATPro is a 15-item questionnaire that measures general satisfaction with a prosthesis. 13 The Turkish version of the questionnaire, developed by Simsek, was used. 14 Each item on the questionnaire is scored between 0 and 3. 13 The AMP was designed to determine the functional capabilities of lower limb amputees, and is a 21-item questionnaire that assesses transfers, sitting/standing balance and various gait capabilities. Item 21 determines whether subjects use a walking aid. AMP scores range between 0 and 47. 15
Data analysis
The data were analysed using SPSS version 16.0 for Windows. The measured variables are presented as mean ± SD while the categorical variables are expressed as percentages. The student’s t-test was used to compare differences between the means of two variables in the same group, and the Wilcoxon paired sample test to compare ordinal scores in a group obtained via test and retest. P values <0.05 were considered to be significant.
Reliability
The most frequently assessed forms of reliability are test–retest reliability and internal consistency. Test–retest reliability measures the stability of a test over a given period of time. In the present study, retesting occurred within three days. The intra-class correlation coefficient (ICC, range 0.00–1.00) was used to determine test–retest reliability. A reliability coefficient between 0.60 and 0.80 is deemed very good, while over 0.80 is deemed excellent reliability. 16 However, Portney and Watkins 17 have suggested that for clinical applications the ICC should be at least 0.90.
Validity
Construct validity requires that similar tests have similar outcomes and strong correlation. 18 The Spearman’s rank correlation coefficient was used for construct validity analysis.
Results
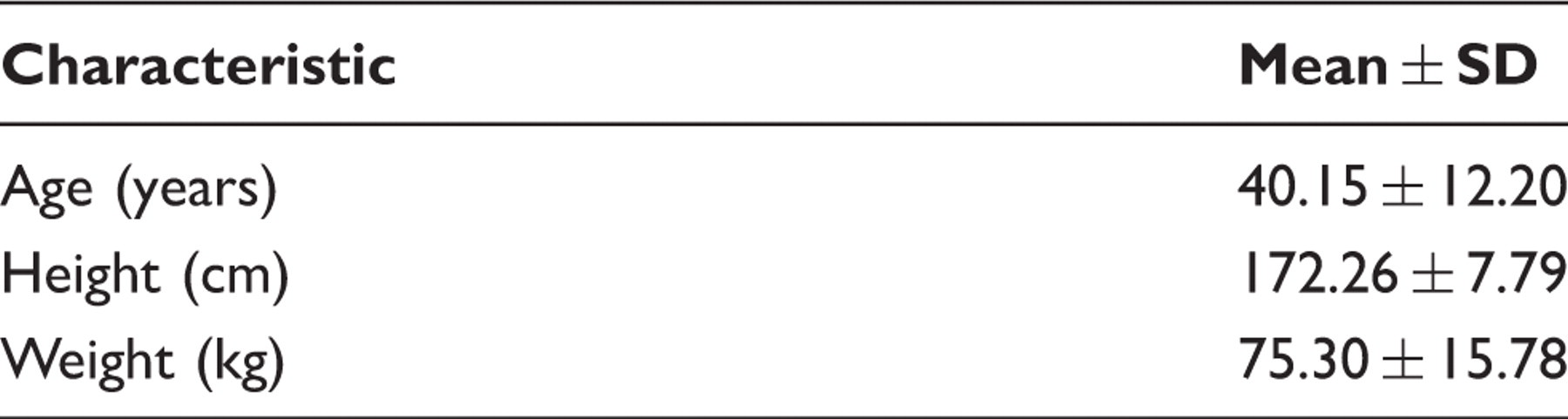
Physical characteristics of participants (n = 47).
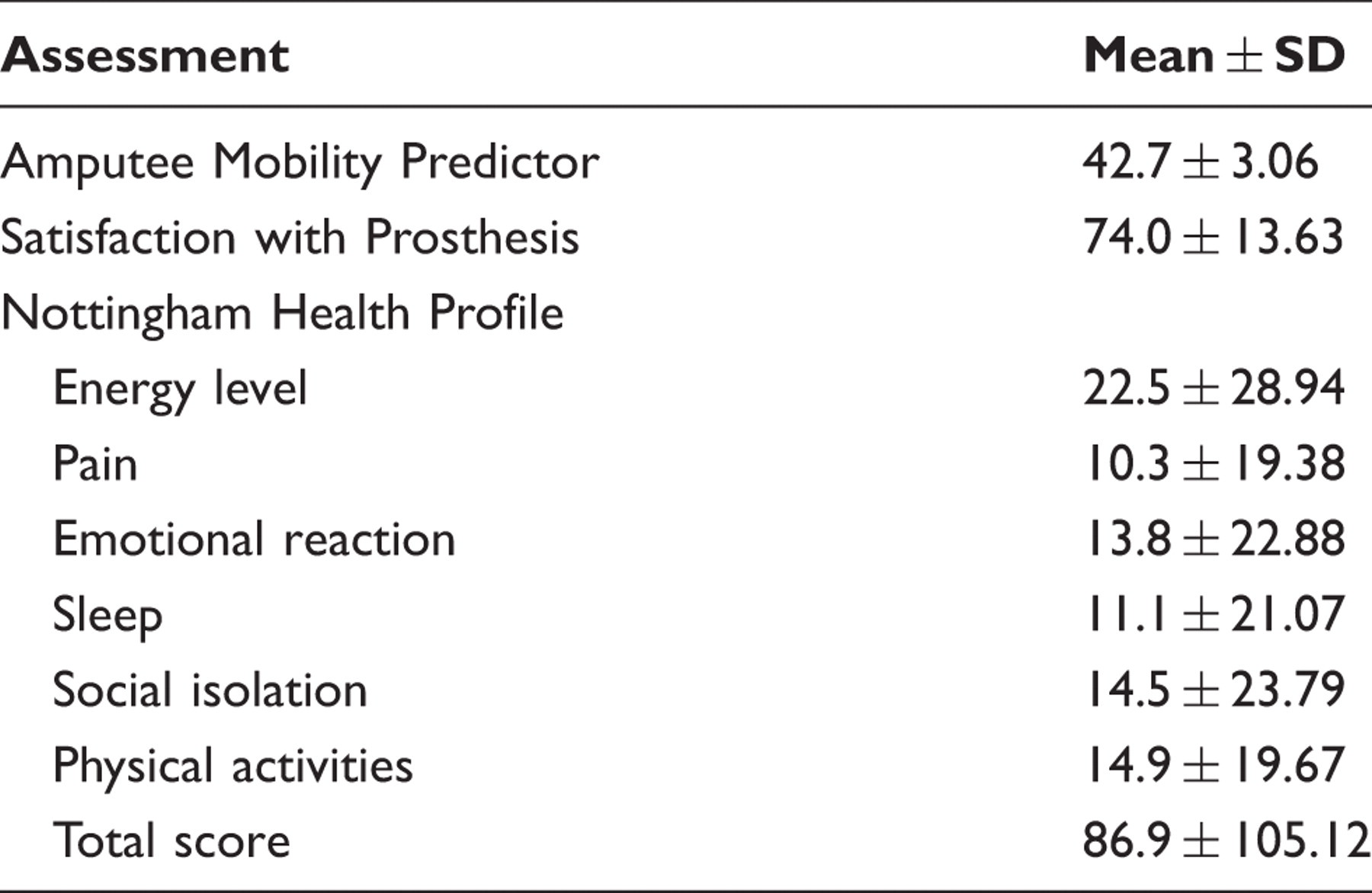
Results of the Amputee Mobility Predictor, Satisfaction with the Prosthesis and Nottingham Health Profile.
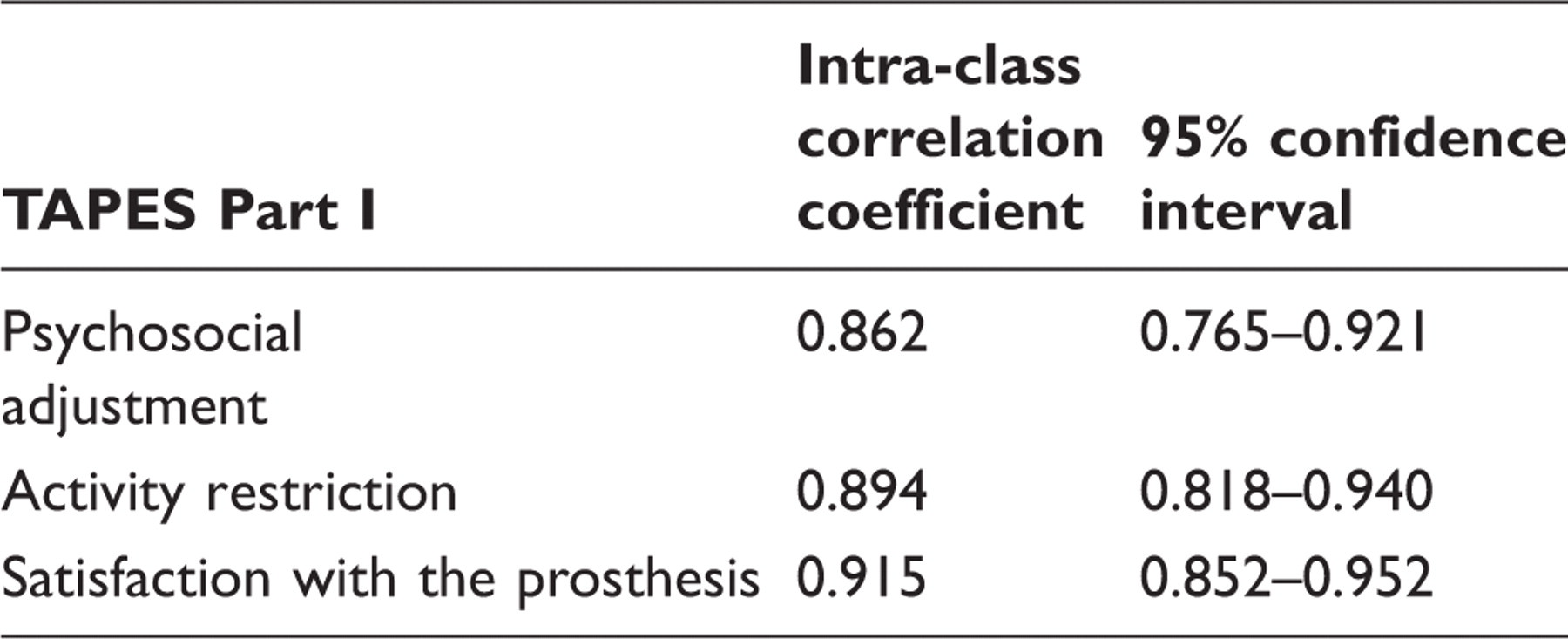
Test–retest reliability of the TAPES Turkish version Part I.
Correlation analysis of the TAPES Turkish version psychosocial adjustment total score with the Nottingham Health Profile (NHP) emotional reaction and NHP total score.
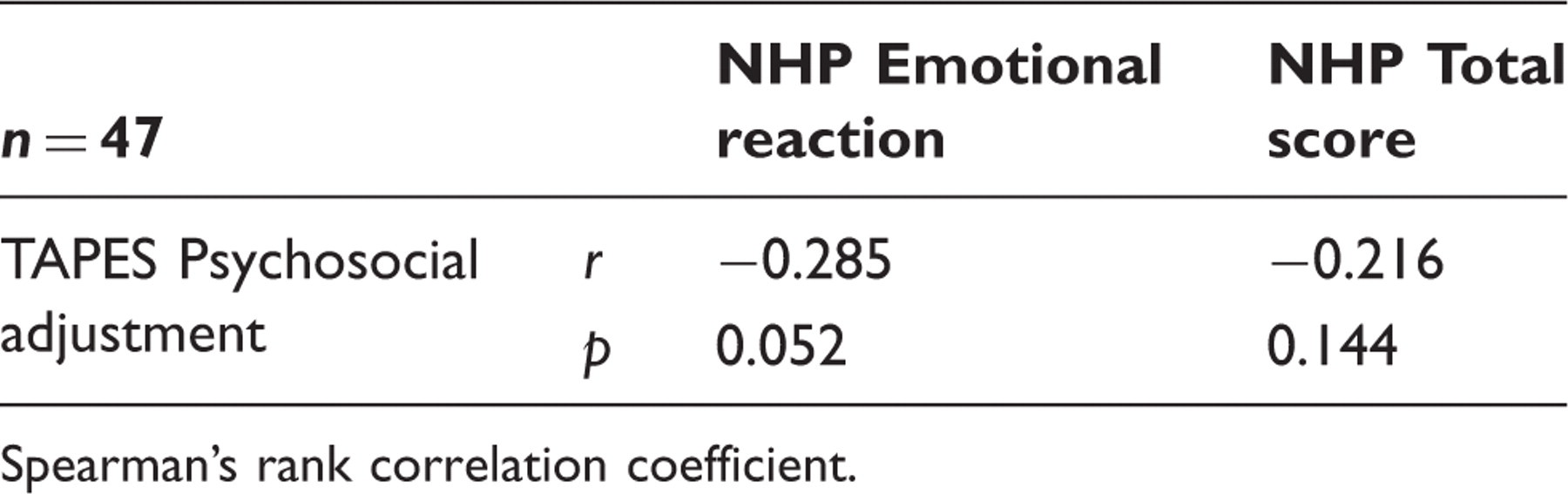
Spearman’s rank correlation coefficient.
Correlation analysis of the TAPES Turkish version limited psychosocial adjustment with all Nottingham Health Profile (NHP) subscales and NHP total score.

Spearman’s rank correlation coefficient.
p < 0.05.
Correlation analysis of the TAPES Turkish version activity restriction with NHP physical activities and the Amputee Mobility Predictor (AMP).
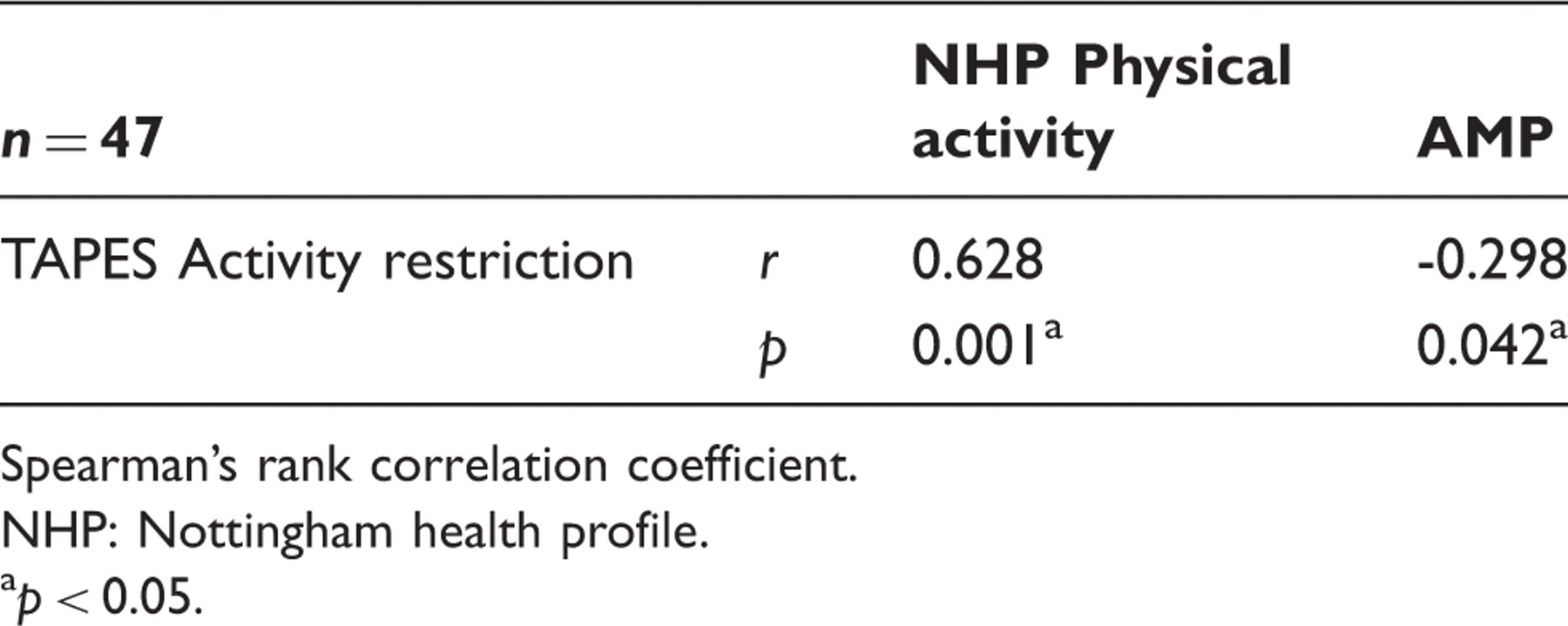
Spearman’s rank correlation coefficient.
NHP: Nottingham health profile.
p < 0.05.
Correlation analysis between the TAPES Turkish version satisfaction with prosthesis and SATPro Satisfaction with Prosthesis.
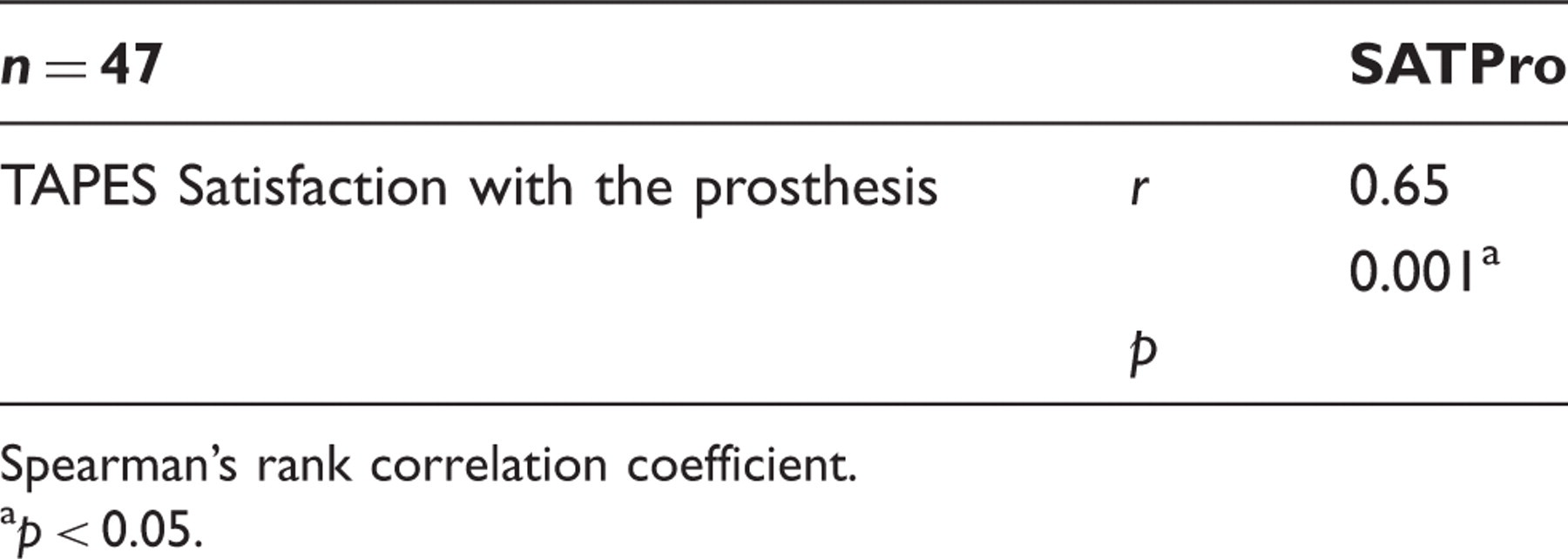
Spearman’s rank correlation coefficient.
p < 0.05.
Discussion
The Turkish version of the TAPES used in the present study was observed to be a reliable instrument for determining the rehabilitation outcomes of a group of Turkish unilateral lower limb amputees. The first domain of the instrument, which includes the subscales psychosocial adjustment, activity restriction and satisfaction with the prosthesis, showed construct validity. However, the validity of the second domain could not be assessed since it does not involve a scoring system.
Reliability
There was no statistically significant difference between the results of the test and retest, which were administered 1–3 days apart. This result was expected because the retest was administered no more than three days after the initial test. This is supported by the ICC scores for the Turkish version that were obtained in the present study. It has also been reported previously that the TAPES is an efficient instrument with good internal validity, and that it is safe to use in routine clinical applications as well as in research. 1,9 We also used item–total correlation to test each part of the first domain of the TAPES and observed a strong correlation with the total score.
Since a total score was not possible for the second domain of the survey, each question was tested individually. The test–retest results were similar, as assessed by the Wilcoxon signed ranks test, except for items 4d and4e. Item 4d concerns the level of stump pain experienced during the previous seven days, and item 4e concerns the impact of the level of stump pain on daily life during the same seven days. For both items, the retests recorded better scores than the first test. This may reflect the generally positive psychological state of these patients, all of whom volunteered to participate in this study. The good psychological well-being of this cohort may have led them to score their stump pain better during the retest. It is likely that patients in a clinical setting, who are more likely to have intolerable stump pain, would yield more consistent answers upon retesting. Items 4a, 5a and 6a of the second domain were observed to be reliable based on the test–retest results. However, there was a difference between the test and retest regarding item 6g (‘Do you experience any other pain that you have not previously mentioned? If yes, please specify’). The response rate for item 6g during the test was only 25.53% (12 participants). When, after the test, 35 participants were asked why they did not respond to item 6g, they said they had not experienced any other pain. The patients were then told to choose ‘no’ if they had not experienced any other pain. The 35 participants then corrected their answer. After these corrections were made, item 6g was found to show test–retest reliability.
Validity
The total score of the psychosocial adjustment subscale in the first domain of the Turkish version of the TAPES did not show correlations with the NHP emotional reaction subscale or the NHP total score. It is possible that a relationship between the Turkish version of the TAPES psychosocial adjustment and the NHP was not observed because all patients in the present study were unilateral lower limb amputees, most being below-knee amputees. Moreover, the psychosocial adjustment questions relate to prosthesis use, whereas the NHP measures the emotional state regarding an existing medical problem or a permanent disability. Checking the validity of the Turkish version of the TAPES psychosocial adjustment subscale against an instrument that is specific to amputees may yield a different outcome. Thus, amputee-specific instruments should be used in future studies.
The limited psychosocial adjustment subscale correlated with all the NHP subscales and with the total NHP score, which may reflect the psychosocial problems experienced by amputees during their adjustment to conditions that require physical function. To determine the validity of the TAPES psychosocial adjustment, its three subscales, namely general, social and limited psychosocial adjustment, should each be assessed separately.
The activity restriction subscale of the first domain of the Turkish version of the TAPES correlated with the AMP and NHP physical activities. Thus, the Turkish version of the TAPES is a valid instrument for determining the activity level of Turkish amputees.
The AMP is a multilateral instrument that can assess the manner in which a particular activity is performed. 15 In our study, the AMP was observed to correlate with activity restriction. This correlation between activity restriction and the AMP, which is a reliable and valid instrument specifically for the assessment of amputees, shows that the activity restriction subscale is valid.
The correlation observed between satisfaction with the prosthesis and SATPro means that this subscale has very good validity.
After the Turkish version of the TAPES test and retest were administered, 36 participants (28 high school graduates and 8 university graduates) were asked if they were experiencing any adjustment problems at home, at work or socially. They were also asked if they had any other problems that were not covered by the survey. The participants considered the coverage of the survey questions to be sufficient and also reported that the survey was clear and comprehensible.
Conclusion
In summary, this study has found that the Turkish version of the TAPES is a valid and reliable instrument suitable for assessing amputees in terms of psychosocial adjustment, activity restriction and satisfaction with the prosthesis. Moreover, it is a multilateral instrument that can be used to assess stump pain, phantom limb pain and other medical problems that may occur in amputees. Based on these findings, the Turkish version of the TAPES may be used by physiotherapists and academics to assess unilateral lower limb amputees in Turkey. This will help determine the needs of amputees as well as facilitating evidence-based research. However, as a limitation of this study, the authors note that while the TAPES has the advantage of being a self-report test, responses should be checked after the test. This is indicated by the fact that the Turkish amputees left one item (6g) blank but, upon clarification after the test, were able to respond correctly to this item.
Footnotes
Funding
This study was financed by the Hacettepe University Office of Administrative and Financial affairs [grant number is 08T09 102 001 (4533)].
Acknowledgements
The authors wish to thank Pamela Gallagher for granting permission to use the TAPES.