
Abstract
Objective: The purpose of this study was to identify factors that predict an individual's subjective quality of life (QoL) after having a lower limb amputation.
Design: Cross-sectional descriptive study design.
Subjects: A total of 415 unilateral, above knee (27.0%) and below knee (73.0%) amputees with an average age of 61.9 years (SD = 15.7) who had lost their limb related to vascular (53.0%) or non-vascular (47.0%) etiology.
Methods: Medical chart review, questionnaires (Frenchay Activities Index, Interpersonal Support Evaluation List, the Center for Epidemiology Studies – Depression scale, Prosthetic Evaluation Questionnaire mobility subscale, and the Activities-specific Balance Confidence Scale) and a QoL Visual Analogue Scale were assessed using multiple linear regression analysis.
Results: The analysis revealed seven significant factors (depression, perceived prosthetic mobility, social support, comorbidity, prosthesis problems, age and social activity participation) as predictors of subjects' perceived QoL. Depression explained 30% of the variation, while the full model explained 42% of the variation.
Conclusion: Several modifiable characteristics influence QoL after lower limb amputation including depression and participation in daily living. This finding suggests the importance of addressing individuals' affective status to regain or maintain QoL.
Introduction
It is estimated that there were approximately 1.9 million people living with limb loss in the United States in 1996 (Adams et al. 1999) and that there was an average of 133,735 amputation-related hospital discharges per year between 1988 and 1996 (Dillingham et al. 2002). Approximately 73.5% of limb losses were lower limb amputations (LLA), the majority of which were caused by traumatic injuries and vascular disease (Owings and Kozak 1998). People with LLA experience multiple challenges which can range from learning how to care for their amputated limb, how to walk, and how to adjust and cope with their limb loss. It seems plausible that given the associated challenges and adjustment that they may experience a change in their quality of life (QoL) (Weiss et al. 1990). The majority of the literature to date has focused primarily on the physical aspects of the adjustment after amputation (Gallagher and MacLachlan 2002) and only more recently have researchers really begun in earnest to pay attention to psychosocial adjustment to LLA (Horgan and MacLachlan 2004). Given the large number of individuals experiencing amputation (Owings and Kozak 1998), a more holistic inquiry into the factors impacting QoL after LLA is warranted.
QoL is often referred to as an overall sense of well-being related to a person's health perception and ability to function (Muldoon et al. 1998). The World Health Organization Quality of Life (WHOQOL) Group defines QoL as an individual's perception of his/her position in circumstance of the culture and values in which he or she lives and with respect to his/her goals, expectations, principles, and concerns (WHOQOL GROUP 1998). It is operationalized as a personal statement of one's characteristics, satisfaction, adaptation to the changes, or perceived health and well-being (Dobkin et al. 1999; Lawton et al. 1999; Pinar 2004).
There are two main conceptualizations of QoL that are prevalent today: (i) The subjective approach whereby the focal point is the individual's emotional or cognitive assessment of the congruence between his/her life expectations and achievements; and (ii) the objective approach which is based on an individual's characteristics that can be objectively measured by an external appraiser (Dijkers 2003). The latter is oriented more towards a functional approach or what is better known as health related quality of life that is largely based on societal standards. On the other hand the subjective approach is based on the premise that QoL can only be determined by the individual (Dijkers 2003) and includes appraisal of an individual's emotions or feelings in the context of their expectations and achievements.
For the past decade, QoL has been acknowledged as an important outcome for rehabilitation programs (Streppel et al. 2001) for not only people who experienced LLA but also for those who experienced stroke or traumatic spinal cord injuries (SCI) (King 1996; Westgren and Levi 1998) as they all face sudden life changes and challenges. As a complex multidimensional construct which is highly personal (Fayers and Machin 2000), QoL is difficult to measure. LLA, stroke, or SCI often prevent individuals from performing activities of daily living and/or participating in physical and social activities. Many measures link QoL to functional capacity, assuming if a person is unable to achieve full physical capacity their QoL is poorer. Such instruments do not reflect the true level of an individual's QoL because they typically only measure factors that contribute to QoL.
Quality of life after amputation
A number of studies have revealed that the QoL of individuals with a LLA is related to a number of characteristics unique to this population including the condition of the residual (Pell et al. 1993; Matsen et al. 2000) and contra-lateral limbs (Pell et al. 1993), the fit of their prosthesis (Matsen et al. 2000), and the time since amputation (Rybarczyk et al. 1995). In addition, common factors such as walking distance (Pell et al. 1993), mobility problems (Behel et al. 2002), symptoms of depression (Livneh et al. 1999), and social support (Rybarczyk et al. 1995) have also been suggested as important predictors of QoL. Despite the growing popularity of QoL and amputee studies, QoL remains a relatively poorly studied concept in this population (Gallagher and MacLachlan 2002). Part of the challenge lies in the different meaning and consequences loss and replacement of body parts has for each person (Weiss et al. 1990; Matsen et al. 2000; Streppel et al. 2001). Additionally, the adjustment process after an amputation is a life-long challenge concerning not only physical but also psychological change (Gallagher and MacLachlan 2002).
To date there are few studies of the amputee population that have considered a multivariable approach to determining which factors are most important in predicting QoL. Most of the previous studies focused on objective measures of QoL. The purpose of this study was to identify and describe the factors that predict subjective QoL in a large sample of community living individuals who have a LLA.
Methods
Design
The data for this cross-sectional descriptive study was captured by linking clinical chart information from two outpatient prosthetic clinics with a follow-up postal survey.
Subjects
Eligible community dwelling adults (> 20 years of age) who attended either of two regional outpatient amputee clinics in South Western Ontario, Canada, were identified through the chart review. Subjects were included if they: had a major unilateral amputation (Syme's level or higher); had used their prosthesis for at least six months; and wore their prosthesis on a daily basis. Subjects were excluded if they had a hip disarticulation or hemipelvectomy.
Protocol
A survey was developed consisting of a number of questionnaires and items. More precisely, socio-demographic, amputation specific factors, physical, psychological, daily activity function, general health, and QoL information was collected. Dillman's (1979) total survey method was used. This approach included sending three follow-ups in addition to the original survey in order to maximize the response rate. The reminders were sent approximately every two weeks after the initial letter of information and survey was mailed. The final reminder included a second copy of the survey. Subjects were instructed to return the survey in the self-addressed prepaid postage envelope if they did not want to participate in the study. The Human Ethics Board at the local university approved the protocol.
Measurement
All of the variables selected for the study were based on factors that were deemed important to QoL based on both literature review and the authors' clinical experience. Existing health scales and standardized reliable and valid outcome measures were used to collect data on these variables.
Socio-demographics
Socio-demographic information such as marital status, education level, employment, and income status were collected from the demographic questionnaire. Chart review was used to obtain the subjects' age, gender, and clinical information (such as comorbidities, cause and level of amputation, and medications). Information on social support was collected using the 6-item version of the Interpersonal Support Evaluation List (ISEL) (Cohen and Hoberman 1983). The ISEL uses a 4-point Likert scale ranging from 0–3 to determine the degree of emotional and instrumental support available. Summing the responses provides a total score which ranges from 0 (no support) to 18 (maximum support) (Cohen and Hoberman 1983).
Amputation related factors
A number of amputation-related factors were captured including the date, cause, level and years since amputation. The cause of the amputation was defined as being related to vascular disease or for non-vascular reasons which included trauma, cancer, congenital conditions or infection not related to a vascular oriented etiology. We clustered the latter group for two reasons: (i) Our clinical experience suggests that individuals who have amputations for vascular reasons are different than the others, and (ii) in our sample there were too few individuals who had their amputations related to cancer, congenital conditions and strict diagnosis of ‘infection’ to permit meaningful statistical analyses of these individual groups. Individuals who had a Symes amputation were classified as below knee (BK) level and those who had a through knee amputation were classified as above knee (AK) level. The number of problems with their prosthesis and residual limb was based on items from the Prosthetic Profile of the Amputee (Gauthier-Gagnon and Grise 1994). Use of mobility device (none, cane, crutches, or walker) was also recorded based on survey information.
Function and physical health
Seven function and physical health-related variables were analysed in this study. Restrictions on activities of daily living (ADLs) were established using the postal version of the Barthel Index (BI) (Gompertz et al. 1994). This measure assesses limitation in nine selected ADLs. Examples of the ADLs are bathing, feeding, and toileting. Two prosthetic specific items (donning and doffing the prosthesis) were added as has been done in previous studies (Miller et al. 2001a, 2001b). Total scores range from 0 (totally limited) to 18 (no limitations) with higher scores indicating greater independence. The 13-item Prosthetic Evaluation Questionnaire mobility subscale (PEQ-MS) was used to assess perceived mobility capability related to walking and transfers over the past four weeks (Legro et al. 1998; Deathe and Miller 2005). Participants rated themselves on an 11-point numerical scale anchored from 0 (‘cannot do it’) to 10 (‘no problem’). A mean score is calculated to provide a rating of general mobility. The 15-item Frenchay Activities Index (FAI) is a behavioural measure of the frequency of participation in selected social activities such as working, gardening, and preparing meals (Datta et al. 1992) over the past 3–6 months. Total scores are summed and range from 0 (no participation) to 45 (frequent participation). The number of comorbidities was determined by asking subjects whether a doctor had diagnosed the subject with any of 19 common health conditions over the past 12 months. Information regarding prescribed medication taken for each of the identified co-morbidities was also obtained and summed to provide the number of medications taken by each subject. A count of common problems experienced with the contralateral limb provided insight regarding the condition or the ‘good leg’. Problems included pain, weakness, swelling, open sores and altered sensation. Lastly, self-assessed health over the last 12 months was evaluated by having subjects rank their health on a 5-point Likert scale, ranging from 0 (poor) to 5 (excellent).
Psychological factors
The 16-item Activity-specific Balance Confidence scale (ABC) was used to assess subjects' perceived balance confidence. Subjects rate their balance confidence on a scale from 0% (no confidence) to 100% (very confident) that they will not lose their balance when performing specific activities such as reaching over-head, bathing, and climbing stairs (Powell and Myers 1995). A mean confidence score is calculated to indicate overall confidence with balance. The Center for Epidemiology Studies-Depression (CES-D) scale was used to assess the level of depressive symptoms over the past week. The CES-D contains 20 items and subjects are asked to answer each item using a 4-point Likert scale. A higher score suggests a greater number of symptoms indicating depression with scores of greater than 16 suggesting likelihood that subjects are depressed (Radloff 1977).
Quality of life (QoL)
A single item question using a Visual Analogue Scale (VAS) to capture the subject's response was used to provide an overall appraisal of subjective QoL. Respondents were asked: ‘All things considered over your life to date, how would you rate your overall quality of life’. The VAS consisted of a 100 mm line with possible scores ranging from 0 (worst possible QoL) to 10 (best possible QoL). Subjects were asked to mark the score along the line that best corresponded with their subjective feelings regarding their QoL. We chose a single-item subjective QoL measure for three reasons. First, other data was being collected in the survey and therefore high correlations would be expected as both the predictors and the dependent variables would be measuring the same constructs. Second, given the complexity of QoL, use of a measure that offered the subjects the opportunity to consider and differentially weight all personally relevant aspects of the experience, while ignoring aspects that are not relevant was considered to provide the best information (Fayers and Machin 2000). Third, use of the VAS in the measurement of QoL has been shown to be a valid and reliable tool (de Boer et al. 2004). Overall, use of the VAS is the simplest form of measuring QoL, yet found to be efficient, easy to use, understand and provides meaningful values.
Analysis
Statistical analyses for the study included the calculation of means, standard deviations and percentages of all variables for descriptive purposes. T-tests and Chi square analyses were used to assess for significant differences for continuous and binary categorical variables, respectively, while ANOVA was used for ordinal and categorical variables with >2 response categories.
Highly skewed continuous variables, such as ABC and CES-D, were collapsed into groups based on their distribution or meaningful cut-off points. For example, a cut-off point of 16 for the CES-D and 80 for the ABC was used to divide our sample into two groups. The CES-D scores greater than 16 suggest individuals who have significant symptoms related to depression and the ABC scores greater than 80 indicate individuals who are deemed to have balance confidence which does not require clinician attention. Some categorical variables, such as education level and perceived health were collapsed into discrete variables; grade 12 or higher versus less than grade 12 and good to excellent health versus poor to fair respectively.
Bivariable analysis was used to determine which variables should be considered for the multivariable analyses. Variables with differences of p < 0.05 were all included in the regression analyses. Forward stepwise multivariable linear regression was used to determine which variables predicted QoL. All of the variables were entered into the regression analysis. Dummy variables were created for a number of factors such as income, the number of prosthesis problems, years since amputation, co-morbidities and medications, based on their distribution. A final parsimonious model was retained based on those factors which achieved statistical significance (p < 0.05). Data entry and analysis were conducted using SPSS Windows (version 11.5).
Results
Of the 535 eligible subjects, 415 (77%) provided complete data (e.g., surveys with no or minimal missing information) for the study. There were no significant differences noted for non-responders based on age, gender, amputation cause, level, or the number of years since amputation.
The average age±standard deviation (SD) of the subjects was 61.9±15.7 years. Most of the subjects were male (71.1%), married (61.9%), and unemployed (74.2%). Most had a BK (73.0%) amputation and the cause of amputation was more commonly related to vascular (53.0%) than non-vascular (47.0%) etiology. The mean time since amputation was 14.5±16.5 years.
Descriptive statistics and mean QoL scores for study variables.
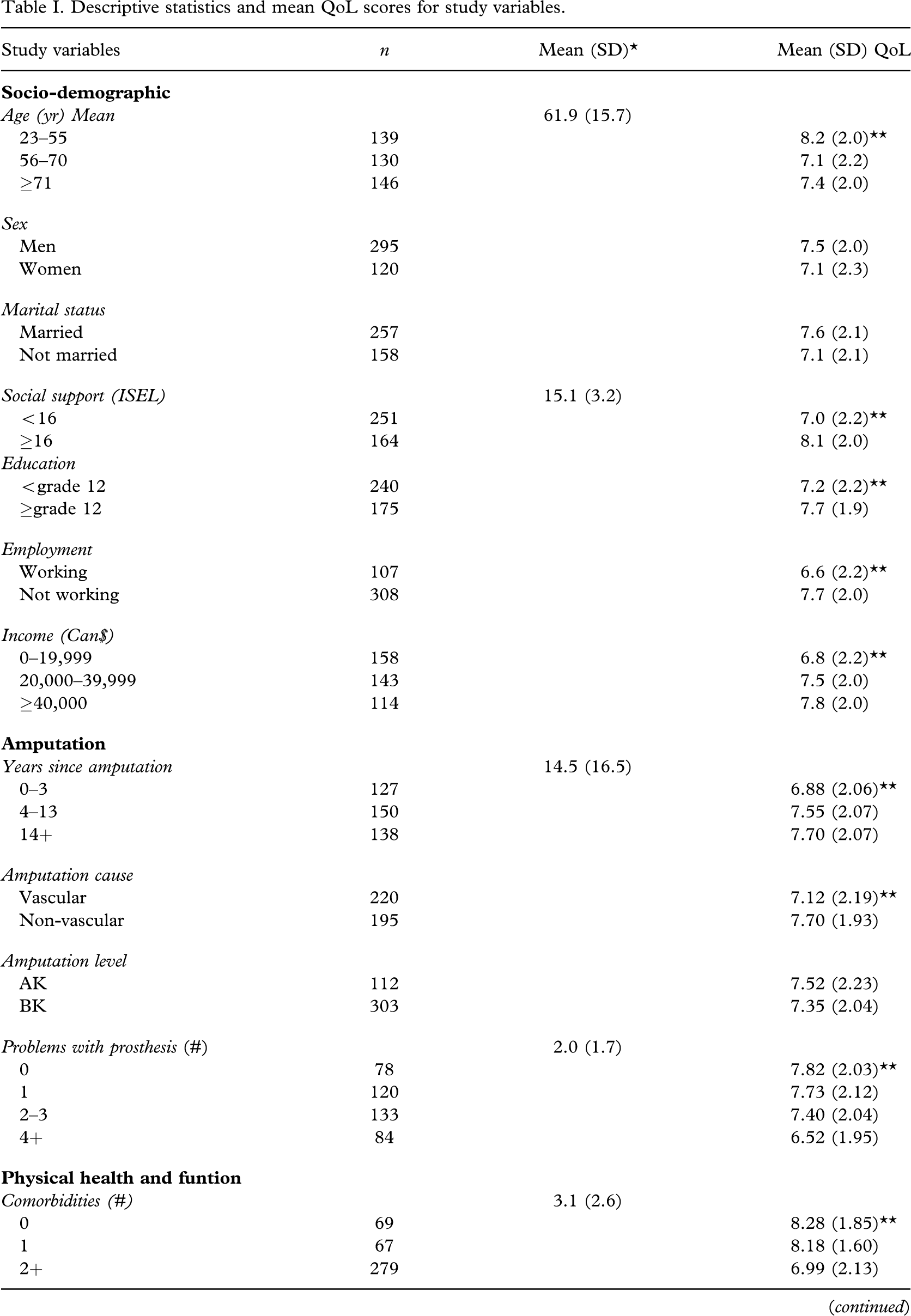
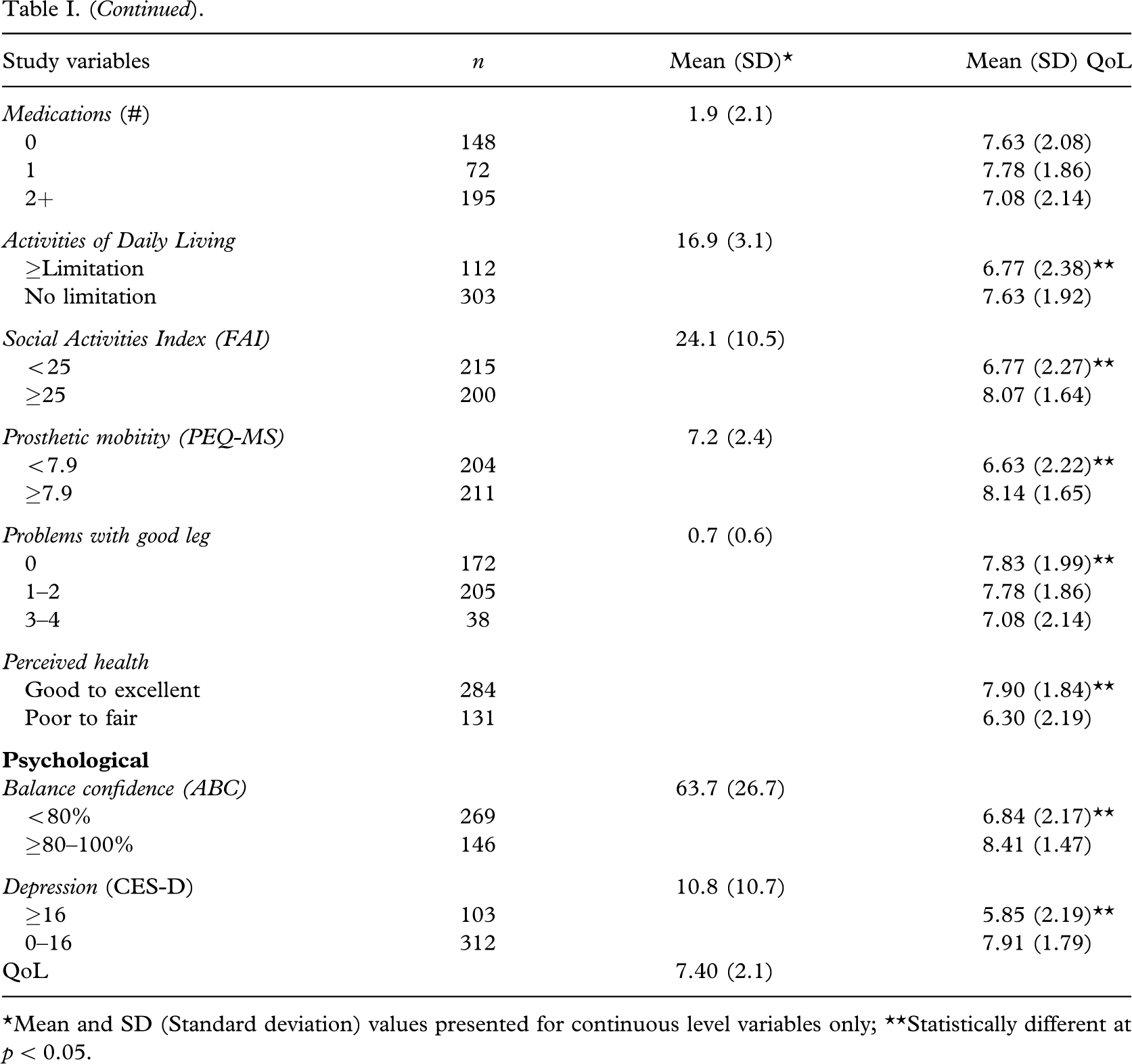
∗Mean and SD (Standard deviation) values presented for continuous level variables only; ∗∗Statistically different at p < 0.05.
Multi-variable regression of predictors of Quality of Life.
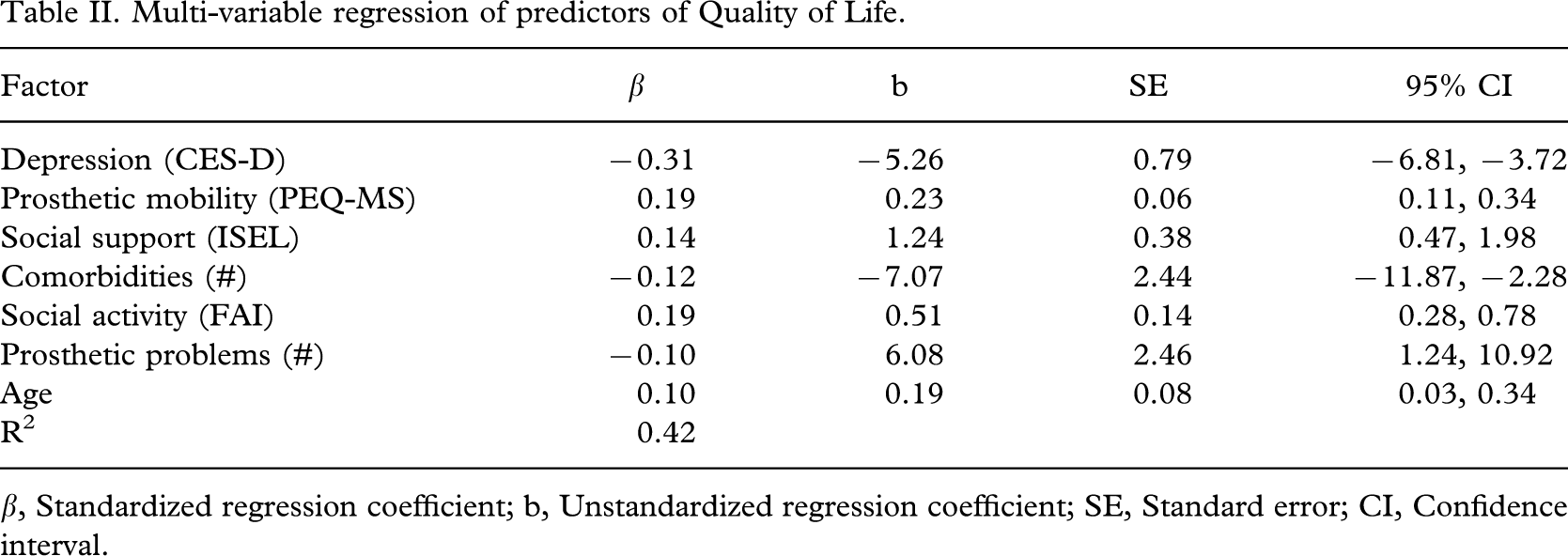
β, Standardized regression coefficient; b, Unstandardized regression coefficient; SE, Standard error; CI, Confidence interval.
Discussion
In our study, subjects reported relatively high quality of life (QoL) with a mean score of 7.4 (±2.1) out of 10.0. This level or magnitude of the QoL was somewhat surprising initially as our clinical impression was that individuals with LLA would have a poorer outcome relative to the quality of their life. One possible explanation of this finding is the response shift phenomena, which has been previously explained as a change in one's evaluation related to a redefinition in the respondent's internal standards, values and conceptualization of the target variable (Sprangers and Schwartz 1999). Therefore, while a respondent may initially report a reduced QoL immediately after their LLA over time their response may be modified related to adaptation to their situation. According to the bivariable analyses in Table I there is a significant difference in reported QoL across the three categories of years reflecting time since amputation. It is interesting to note that there is a moderate improvement in QoL as participants live longer with their amputation. However time since amputation did not enter the final regression model.
Our multiple regression model explained only 42% of the variance in QoL, which given the complexity of this variable, is quite good. The predictors that we found to be important included symptoms of depression, prosthetic mobility, social support, number of comorbidities, daily social activity, number of prosthetic problems, and age. Many of the predictors of QoL are modifiable factors which given appropriate attention may alter the mean population QoL and provide a better outcome after amputation.
A higher QoL was reported by those individuals in this study who had lower depression scores. Approximately 30% of subjects in this study demonstrated a score indicative of depression, which is consistent with the amputee literature. In terms of depressive symptoms measured using the CED-S, prevalence reported in the literature has ranged from 29% for inpatients (Langer 1994) to 21–35% for outpatients (Rybarczyk et al. 1992; Darnall et al. 2005). Dunn (1996) reported that depressive symptoms were found among persons who did not find meaning in their amputation, were less optimistic, perceived less control over their disability, and were younger. Given the significant proportion of the amputee population experiencing symptoms of depression, a holistic rehabilitation program incorporating not only physical, but also psychosocial components is recommended. By improving depressive symptoms, it is anticipated that an improvement in QoL for these individuals would also follow.
Mobility capability was the next best predictor of QoL in this study, explaining 6% of the final model. This predictor suggests that it is important for an individual to feel that he/she is able to move around their environment safely and independently after their amputation and rehabilitation and is well stressed in the literature (Pell et al. 1993; Matsen et al. 2000; Miller et al. 2001a; Refaat et al. 2002; Van der Schans and Geertzen 2002). Failure to regain and maintain full ambulation skills after amputation restricts mobility, which, in turn, can influence an individual's choice of activities (Munin et al. 2001). As such, it stands to reason that subjects' perceptions about their mobility were moderately related to their perceived QoL while controlling for other important variables.
Social support explained an additional 2% of the final model variance. The demonstrated need for social support following amputation in this study is also consistent with results found by Williams et al (2004), whereby the degree of perceived social support predicted pain interference, life satisfaction, and mobility after amputation. These findings suggest that interventions aimed at improving the quality of social relationships after amputation may facilitate participation in social and physical activities, thereby improving QoL.
The remaining 4% of variance explained by the final model includes: the number of comorbidities, degree of social participation, prosthesis problems, and age. Multiple co-morbidities can lead to physical discomfort and disabilities, as well as negative psychological issues, such as anxiety and depression (Darnall et al. 2005). Consequently, it is reasonable that the number of existing comorbidities, which may also reflect the general overall health of the sample, is one of the important factors related to one's perceived QoL. Social participation is impacted by a variety of factors, including social support and mobility capability. Given the link between these three factors, it is not surprising the degree of social participation is related to QoL. Prosthesis problems can cause mobility and residual limb issues which can lead to other problems, such as reduced activity participation and increased isolation (Datta et al. 1992; Muldoon et al. 1998; Dobkin et al. 1999). Since having good mobility skills and an appropriate prosthesis can provide individuals with physical freedom to go places and to participate in activities of their choice, it is clear that this factor can influence an individual's QoL. Finally, the mean age of our sample was 61.9 years and was found to be important but the least significant predictor of QoL in this study. With increasing age, individuals commonly experience a decrease in muscle mass, strength, and flexibility, as well as an increase in medical complications (Kegal et al. 1977; Pohjolainen and Alaranta 1992; Nair 1999; Bennett 2000). These changes may result in other deficiencies in their activity performance and participation. As a result, it is reasonable that age was found to be one of the predictors of perceived QoL in this study.
QoL for individuals who have experienced a LLA is influenced by physical, sociological, and psychological changes (Dunn 1996). As one would suspect, mobility and prosthesis related problems are often identified as the major concerns among individuals with a LLA to regain and maintain QoL (Niseen and Newman 1992; Pell et al. 1993; Dunn 1996). This perception of equating QoL with mobility may be facilitated by the physical focus of most amputee rehabilitation programs, such as an individual's ability to perform their daily activities, including transfers and gait training. In contrast, the psychosocial aspect of an individual's rehabilitation has a relatively minor focus. It is unknown whether the physical focus of amputee rehabilitation programs is due to the health care team's lack of knowledge and/or resources regarding the importance of psychosocial factors in amputee rehabilitation, a limited amount of therapeutic time secondary to short lengths of rehabilitation stays and the push to achieve tasks necessary to live independently (such as toilet transfers), or lack of program development. Although the physical aspect of rehabilitation remains the focus in most amputee rehabilitation programs, it is recognized in the literature that social and community reintegration is an important component of rehabilitation. Furthermore, anxiety and depression or emotional disturbances have been identified as key factors toward QoL and healthy recovery after a LLA (Rybarczyk et al. 1995; Refaat et al. 2002). This research investigating factors that predict or influence the QoL of individuals with a LLA contributes to this body of knowledge and demonstrates the need for a comprehensive rehabilitation program incorporating both physical and psychosocial components.
Differences in the findings between our study and those of other studies may be explained by the variation in time since amputation of our sample. Many previous studies (Streppel et al. 2001; Williams et al. 2004) involved inpatients or outpatients with shorter time frames since their amputation. Therefore a response shift may have influenced the magnitude of QoL of our sample and indeed we did notice a small but statistically insignificant increase in the mean QoL among individuals who had their amputation for a longer period of time. The response shift hypothesis we the authors pose cannot truly be tested in our sample given the cross-sectional nature of our data. A longitudinal design would provide a more robust design which would enable better description of the variation in QoL over time.
Other limitations associated with our study such as only using an English version of the survey, having a relatively young and the heterogeneous sample potentially threaten the validity of our findings. In particular, the mixed nature of our non-vascular group may be an issue and potentially could be a reason why amputation cause was not a predictor of QoL in the final regression model. For example, unlike vascular disease and diabetes reported to be common causes of LLA and more frequent in older adult populations in the United States, LLA due to cancer/tumor was reported to be more common in all age groups including younger and working population (Kauzlaric et al. 2007). Despite the significantly lower rate of LLA caused by cancer/tumor in the United Sates (Dillingham et al. 2002; Kauzlaric et al. 2007), it was reported that those individuals' physical, mental and social well-being were intensely affected (Rybarczyk et al. 1992). As we have recognized the importance of assessing (or finding out predictors of) QoL among individuals with LLA due to cancer/tumor as well, it is our regret that we were not able to differentiate this particular study sample and/or to take this matter into consideration at the analyses due to the previously provided reasons in the methods (amputation related factors) section. However, given that our mixed non-vascular group was similar with respect to sex, age and QoL (analyses not shown) we are confident that this is not the case for our sample.
Despite the fact that Canada is a bilingual nation, English is used by 97% of our target population (Statistics Canada 2007) therefore there would be minimal benefit in using a multi-lingual survey.
Considering a reportedly increased rate of LLA with age (Dillingham et al. 2002) and the estimated amputation rate in United States being higher for persons age 65 years and older (National Diabetes Data Group [NDDG]1995), the age range of 23–91 seen in our study sample with the mean age of 61.9 years might be considered as a relatively young LLA population. This fact could be one of our study limitations as it could affect the generalizability of the study results to a typical LLA population. Furthermore, regardless of a relatively large group of individuals drawn from two large regional outpatient amputee clinics our sample may not be representative of the larger population of individuals with a major lower limb amputation.
Despite the good response rate and the knowledge that the responders did not vary from the non responders on a number of key variables there is potential for response bias as not everyone who was contacted responded to the survey. Therefore there may be a different magnitude of QoL in the non responders.
Finally, while recognizing the limitation related to using self-report data and the important influence that issues such as mental status, recall bias and subjectivity play with respect to the quality of the data, self-report data is currently the most efficacious method of collecting information on variables such as QoL.
Conclusion
In decreasing order of prediction, this study revealed that depression symptoms, prosthetic mobility, social support, comorbidities, social participation, number of prosthesis problems and age are important factors that predict the perceived QoL among individuals with LLA. Given the physical focus of most amputee rehabilitation programs, these results are of great clinical importance. More specifically, therapeutic interventions should address not only the physical aspects of amputation, but also the psychosocial adaptation to limb loss.
Footnotes
Acknowledgements
The authors wish to recognize Dr Mark Bayley for assisting with subject recruitment and the Canadian Institutes of Health Research who provide salary support for Dr W. C. Miller.