
Abstract
Background and Aim: Stump healing is critical to post amputation management. When healing is not optimal, immobility is prolonged and patients risk hospital acquired deconditioning. Two clinical cases with unhealed trans-femoral stump wounds are described. Vacuum assisted closure (VAC) dressing with concurrent prosthetic utilisation was undertaken successfully in both cases.
Technique: Fitting of the prosthetic socket included space for VAC dressing with modifications to allow the suction piping to exit the prosthesis. With VAC application, timely rehabilitation and mobility was enabled despite incomplete wound healing.
Discussion: The two clinical cases described made excellent progress. Discharge home was expedited with the provision of portable VAC pumps. Wounds healed fully without infection. Both patients were able to mobilise sooner than if they had to wait for complete wound closure and, importantly, the consequences of prolonged immobility were minimised. No extra costs were incurred using this novel therapy.
Background and Aim
Optimal stump healing has been stated as a primary objective of post-amputation management. 1 However, problems with wound healing are outlined in the literature, with as many as 46% of wounds reported unhealed on a first visit to a limb fitting centre. 2 These high rates are the result of poor surgical technique, infection, excessive oedema, tissue necrosis and other co-morbidities associated with this population. 3
Early mobilization promotes healing through increased circulation and decreased oedema, enhances correct collagen formation 4 and affects the sequelae of prolonged immobility. These sequelae include muscle wasting, oedema, malformation of collagen, as well as secondary effects such as thrombosis, pneumonia and joint contracture, which ultimately diminish functional capacity. 5
A novel approach to wound management is described with the aim of facilitating early mobilization in two transfemoral amputees who suffered disturbed wound healing after primary amputation and after revision, respectively. Both wounds were treated with vacuum-assisted closure (VAC) dressings, the use of negative pressure dressings to relieve localized oedema and increase blood flow by removing unwanted interstitial fluid. VAC also promotes fibroblast proliferation and reduces bacterial levels in the wound. 6
Technique
Two cases are presented to show the feasibility of mobilizing patients with prostheses adapted for the simultaneous use of VAC dressings because of unhealed amputation wounds. It is hoped that this paper will motivate others to trial this novel treatment modality, as it requires no added cost or componentry, and benefits patient rehabilitation.
Ethical approval was not required, as in each case the prosthesis was constructed and provided in accordance with standard practice. The procedure was risk assessed by the clinical team, the surgeons involved in the amputation, and the patients, as is normal practice at our facility. Formal written consent was obtained for all medical photographs using standardized Trust procedures. Normal patient consent policy dictated that the patients could withdraw at any time from this particular form of treatment and that such withdrawal would not affect their subsequent treatment in any way.
Case 1
The first case was a 37-year-old man who endured 17 years of limb salvage following a road traffic accident, he was physically well-conditioned with the potential to be an excellent prosthetic user. His post-surgical recovery and pre-prosthetic rehabilitation were severely limited by a non-healing wound and infection (Figure 1). He was compliant with bed and gym-based exercise programmes, but became increasingly frustrated by his prolonged stay in hospital and inability to begin an early walking aid (EWA) trial. He could not be fitted with the pneumatic post-amputation mobility (PPAM) AID due to the size of his residuum. There was hesitation from his surgeon regarding mobilization because of the risks of pressure applied to the wound.
Patient 1’s transfemoral residuum showing poor healing and oedema; equal anterior and posterior flaps are evident.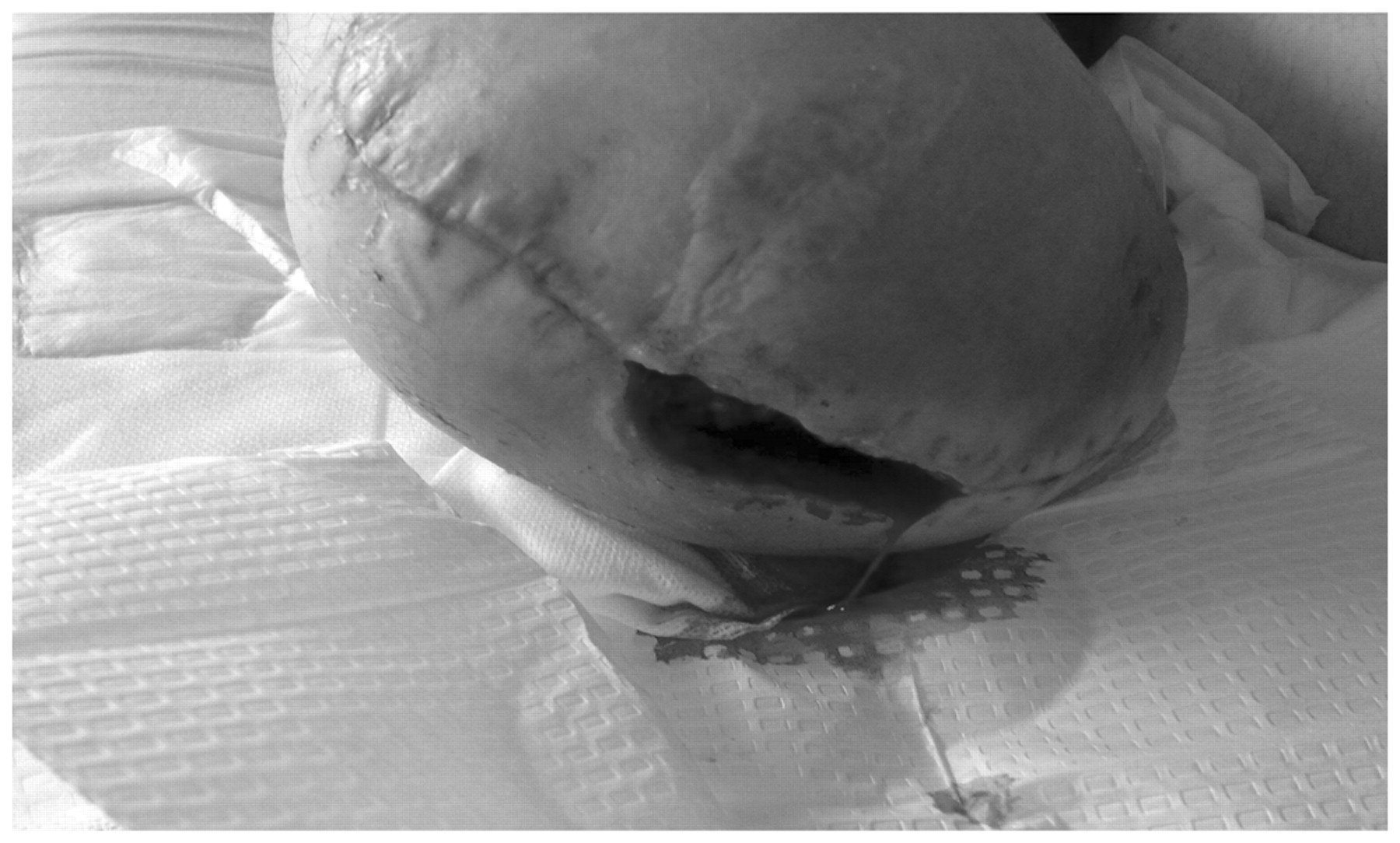
In consultation, the visiting rehabilitation and hospital-based orthopaedic consultants decided to prescribe a prosthesis that could be used as an EWA. Delivery of the device was delayed as the patient returned to theatre for debridement and evacuation of an infected haematoma. Staphylococcus aureus bacteria were identified and treated with six weeks of intravenous antibiotics and the wound left open to drain. A VAC dressing was applied to the wound a few days later. Team discussion led to a decision to continue with the plan of commencing mobilization with a prosthesis. This was fitted with definitive componentry, as is local practice for a primary (first) artificial limb.
When the VAC dressing was applied, the tissue viability nurse was asked to place the hardest components of the dressing (hose plus fitment) as distal as possible to avoid them getting trapped, kinked or applying pressure to the residuum through contact with the socket (Figure 2).
Patient 1’s transfemoral residuum with a VAC dressing correctly positioned with the hardest components as distal as possible. This was undertaken to not apply pressure and to avoid the VAC dressing becoming trapped within the prosthetic socket.
The socket was made with sufficient distal space to reduce pressure on the wound and to enable the application of a VAC dressing. The VAC hose exited the socket through a hole made with a drill cutter, allowing the portable VAC to be used continuously during walking. The hole size was equivalent to that made for a suction valve in a self-suspending socket (Figure 3).
Patient 1 fitted with his adapted prosthesis showing the hole drilled to accommodate the hose and allow fluid to drain unimpaired through the VAC device whilst walking.
The patient was then able to continue with rehabilitation, and began a customized and progressive gait re-education programme until discharged from hospital.
Case 2
The second case was a 45-year-old female. Her original amputation followed complications related to osteosarcoma of the tibia and its treatment in the mid 1980s. She underwent surgical revision to remove necrotic fat tissue following a fall that caused blunt trauma to the posterior aspect of her residuum several months prior to our intervention. During surgery, swabs were taken and Staphylococcus lugdunensis bacteria were identified and treated with six weeks of intravenous antibiotics. The surgical wound was left open to allow free drainage and a VAC dressing was applied after approximately one week. Adjustments were made to the fit of her prosthesis to allow her to use it optimally and with continued use of the VAC. The Northvane liner was removed and extra socks provided to allow an acceptable fit. The original suction valve was removed, providing an aperture large enough to fit the VAC tubing through. A total elastic suspension (TES) belt was added in place of the previous suction fit. As in case 1, the VAC dressing was applied with the hose positioned as distally as possible. The patient was then able to begin mobilizing over short distances with her own prosthesis and stick, successfully improving her exercise tolerance until discharged.
Results and Discussion
We propose that both patients were able to mobilize sooner than if they had waited for complete wound healing. Whilst allowing mobility with VAC dressing, we are pleased to report that at the time of writing both patients were fully healed and free of infection. Both achieved the ability to walk outdoors further than 50 m, and a SIGAM score of D or E. 7
In our opinion, more timely mobilization lessened the patients’ deconditioning and led to quicker rehabilitation with better outcomes. Independent walking was achieved whilst maintaining wound healing therapy, whilst subjective improvements in walking function, exercise tolerance and participation were noted. Muscle wasting and associated deconditioning are commonly experienced with the conventional treatment modality of waiting for the stump to heal before applying EWAs or a prosthesis. 8 Allowing these patients with unhealed stumps to mobilize reduced the effects of immobility, as supported by a previous study. 4
In both cases there was subjective evidence that self-efficacy was being adversely affected by their post-amputation management. The patients agreed that they were becoming increasingly frustrated at having to stay in hospital and expressed losing hope of regaining mobility. Depressive symptoms have been reported most often from patients who found no meaning in their amputation, perceived a lack of control over their disability and were less optimistic. 9 The same authors highlighted mobility and prosthetic-related problems as important in regaining and maintaining quality of life. Both patients in this series expressed relief at commencing their prosthetic rehabilitation after introduction of our novel approach.
Regrettably, we are unable to report objective financial benefits for these cases of expedited mobility, as it is difficult to match age and condition retrospectively to similar cases to assess length of stay or healing times. These two comprised the only local cases of prolonged VAC use after transfemoral amputation in the past two years. We can hypothesize that there were cost savings from reducing the length of in-patient stay and from limiting social care needs such as major home adaptations or re-housing, as has been found in other relevant patient populations. 10 The prosthetic team reported that no extra manufacturing was undertaken and no extra prosthetic costs incurred with this treatment regime. Neither patient required more sockets than would have been expected following either primary amputation or revision surgery.
These patients were mobilized after only two weeks of VAC dressing application, which they continued to use for at least a further seven weeks. Had they followed the established regime they would have been unable to commence prosthetic rehabilitation until the wound was healed. It is proposed that early mobilization through prosthesis modification offers a new approach to the management of transfemoral amputation wounds where VAC dressings have been applied. This treatment regime has multifaceted benefits both for patients and for those supplying their care, as it reduces the impact of prolonged immobilization and gives patients both a psychological and physiological boost that leads to improved outcomes.
Key Points
Conservative management of unhealed trans-femoral wounds is typical in potentially ambulatory amputee patients, and is associated with delay in rehabilitation and hospital-acquired deconditioning. VAC dressings and concurrent early ambulatory training in two clinical cases is feasible, cost effective, with no adverse effects reported. The impact of this novel management may include psychological benefit to patients, decreased hospital length of stay, timely active mobility and less healthcare utilisation on discharge.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.