
Abstract
Background:
The refined clothespin relocation test is a test used to evaluate the performance of a prosthesis user by analysing the compensatory motions and time to complete a grasping and placement exercise. The test has been studied previously with a motion capture laboratory and has now been adapted for a clinical setting. A comparison of prosthesis user to an able-bodied group is needed to determine efficacy as an assessment tool.
Objective:
To modify the previous refined clothespin relocation test and assess whether it can distinguish between able-bodied and prosthesis users.
Study design:
Comparative analysis.
Methods:
Forty-two able-bodied subjects and three prosthesis users completed the adapted refined clothespin relocation test protocol. Average refined clothespin relocation test scores describing the degree of compensatory movements and the time to complete the protocol were compared using a Mann–Whitney U-test.
Results:
A significant difference was found in the refined clothespin relocation test score between the able-bodied (Md = 65.32, n = 42) and prosthesis users (Md = 23.07, n = 3) with a medium effect size (p < 0.001, r = 0.43).
Conclusion:
Prosthesis users demonstrated larger compensations and longer completion times, as reflected in the refined clothespin relocation test final score. The refined clothespin relocation test has the potential to be a useful clinical tool to assess user performance on a functional task.
Clinical relevance
This preliminary study demonstrates that the adapted protocol can distinguish between the two groups based on refined clothespin relocation test score. A future multi-centre study is required using multiple raters and comparing it with the existing outcome measures to validate the refined clothespin relocation test and determine inter-rater reliability.
Keywords
Background
Determining patient functional level is required when assessing whether any prosthetic intervention will actively make a difference to the prosthesis user. Questions often arise as to what the clinical team should test, what can they test and how they should test it. Hill et al. 1 discussed that some commonly used prosthetic assessment tools often have uncertain psychometric properties which makes it difficult to objectively understand a user’s ability, capacity and skill level when using a prosthesis. Some of these tools have been standardized with non-prosthesis user groups, which make it difficult to rely on these tools within the prosthetics field. 2 A review of prosthetic usage and abandonment underscored this point, and stressed that developing outcome measures with well-defined vocabulary that is easily understood internationally would allow for comparisons to be made across different centres around the world. 3
Promoting standardized outcome measures is the focus of efforts by an international community of healthcare professionals.1,4–7 Developing an upper limb assessment within the domains of the International Classification of Functioning, Disability and Health (ICF) from the World Health Organization has been discussed previously. 8 As clinicians view the prosthesis as an extension of the body, it is important to assess aspects of performance of the prosthetic hand in the Function domain. The Activity domain, however, is where many assessments fall under, as they involve the execution of a task with the prosthesis in a controlled environment. Self-reported measures (surveys and questionnaires) can provide further understanding of how the user works with their device and allow the user to provide a patient-reported outcome (Participation domain). This assists clinicians and prosthetics manufacturers by providing an indication of how a user feels about their device.
The Upper Limb Prosthetic Outcome Measures (ULPOM) group put forth recommendations for further validation of specific assessments,5,9–12 and newer ones continue to be developed, targeting the functional capacity of the user specifically. A study by Resnik et al. 13 detailed the development of the Activities Measure for Upper Limb Amputees, a series of tasks graded by a clinician and then amalgamated into a final score of patient functionality. The use of a single overall score provides a metric that is easily understood by healthcare professionals and researchers alike.
For the ICF’s Function domain, motion capture provides more comprehensive and objective data about the prosthesis user’s motion and has been used to this end,14–16 as it provides insight into the user’s compensatory motions to a further degree than a clinical observation. These motions compensate for reduced functionality and their effects have been discussed,17–21 but the expense of motion capture systems and time required to use them will prevent motion capture from being adopted routinely in the majority of prosthetic clinics. A less expensive but clinically viable solution is required.
An economical option for assessment employs the Rolyan Graded Pinch Exerciser and involves starting a timer, relocating three clothespins between a horizontal and vertical rod, and then stopping a timer. The use of these procedures was originally conceived as a training aid, as the use of the wrist, elbow and shoulder (anatomical/prosthetic) are required to complete the task. The potential as a measurement tool was recognized and has been used in previous prosthetics research.22–27 The procedures are simple to administer, and compensations are readily apparent to the observer. Hussaini’s work recognized the variation in the multiple procedures being used previously and the difficulty of comparisons between studies, 28 as different approach trajectories could be used to accomplish the same task of relocating the three clothespins. The refined clothespin relocation test (RCRT) was then developed and uses a self-timed procedure (user initiated timer) and specifies the start and end locations (demarcated on the rods) of where the clothespins are to be moved from and to, as well as the sequence. 22 These changes allowed for a more direct comparison of the kinematic trajectories between subjects (obtained through motion capture) as the protocol was further standardized, and the task was now being performed in a similar way by all the subjects.
Adapting the RCRT protocol and evaluation of score
The original protocol required a longer setup time (test instructions, marker placement), resource allocation (motion lab and post-processing), and it would likely not be used outside of a research setting because of these limitations. The updated RCRT requires the use of a single video camera, capturing the user’s motion in the frontal plane. In Hussaini’s work, a reduction in compensatory motions was seen in trunk lateral tilt, trunk flexion, trunk rotation and humeral elevation when a powered wrist rotator was used in conjunction with a single degree of freedom hand, as compared with a prosthesis with a friction wrist. 28 In this simplified protocol, only trunk lateral tilt and shoulder abduction were used. In the previous study, increased trunk lateral tilt was observed in conjunction with increased trunk flexion and trunk rotation in the prosthesis user. Therefore, analysing trunk lateral tilt and shoulder abduction were judged to be sufficient for evaluation, which could be graded by observation rather than motion capture.
Comparing the two groups using the RCRT score will determine whether or not the score can become a viable outcome measure for prosthetic assessment. There is currently no single metric used for assessing overall user functional level that combines the results of task execution (time to complete) with the quality of execution (compensatory motion). Therefore, the need exists to establish a statistical basis to prove that the score can distinguish between two groups that are known to be different.
The purpose of this study was to adapt the previous protocol for a clinic and evaluate whether the new protocol could distinguish between an able-bodied and a prosthesis user group.
Methods
Study participants
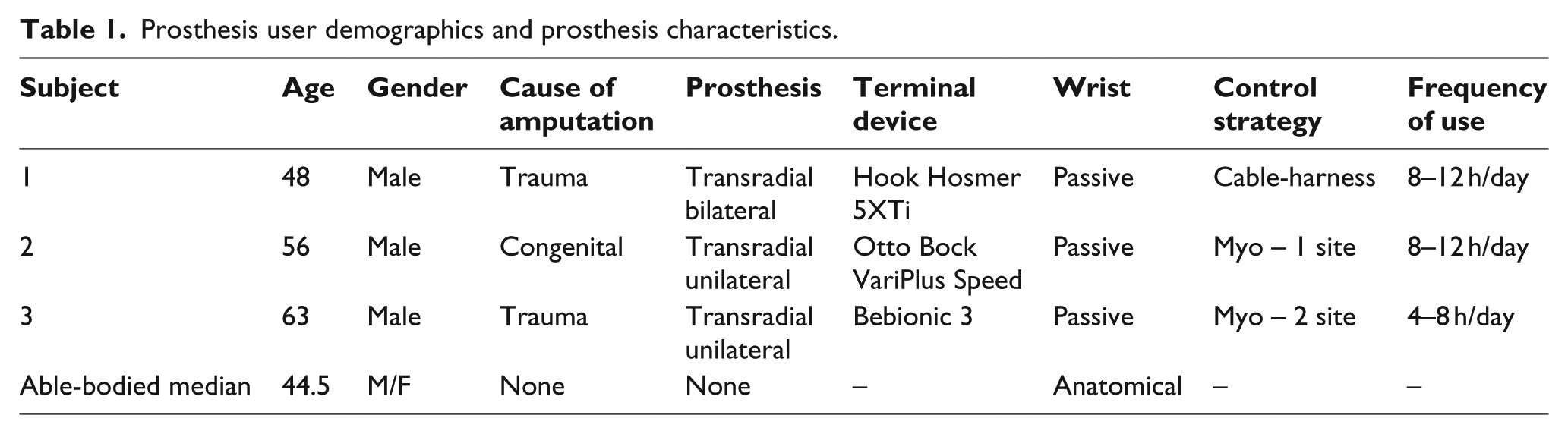
A total of 42 able-bodied subjects were recruited through an online university notice board. Ten of these subjects were left-hand dominant and performed a left-handed assessment. A convenience sample of four prosthesis users, recruited by a clinician during prosthetic treatment at a local prosthetic clinic, completed the test (all right-hand dominant). All prosthesis users were experienced with the device under assessment for at least 2 years. The type of prosthesis, terminal device and control strategy employed are listed in Table 1.
Prosthesis user demographics and prosthesis characteristics.
This study was approved by the Research Ethics Board (REB 2015-080) at the University of New Brunswick. Subjects provided written consent before participation.
Performing the RCRT
At the commencement of the trial, participants were instructed that they were allowed to rotate their hand (passive wrist) into position to be able to grasp the clothespins. They were not allowed to change the orientation of the prosthetic hand under assessment (with their contralateral hand) after the testing began. All subjects were allowed to practice a single upwards and a single downwards trial before the test began.
The pinch exerciser rested on a table adjusted to the height of the subject’s anterior superior iliac spine (Figure 1). Visual aids depicting the directions of the upwards and downwards clothespins trajectory (A4 paper size photos of diagrams in Figure 2) were in clear view behind the camera recording the trial. The direction and order of clothespin movement were described as inside-out for the upwards direction and outside-in for the downwards direction. Complete instructions are provided in Appendix 1. The subject started a timer positioned on the side under assessment, moved the clothespins in the prescribed order and finished by stopping the timer. The time was then recorded for that trial, and the clothespins were positioned for the downwards trial. The subject started the timer, moved the clothespins downwards and stopped the timer. The time was recorded and clothespins were repositioned for the second upwards trial. Five trials in both directions were recorded. The captured video was then observed and compensations were graded and the RCRT score was calculated. All sessions were videotaped and referred to when grading the compensations. A single rater graded all the subjects.
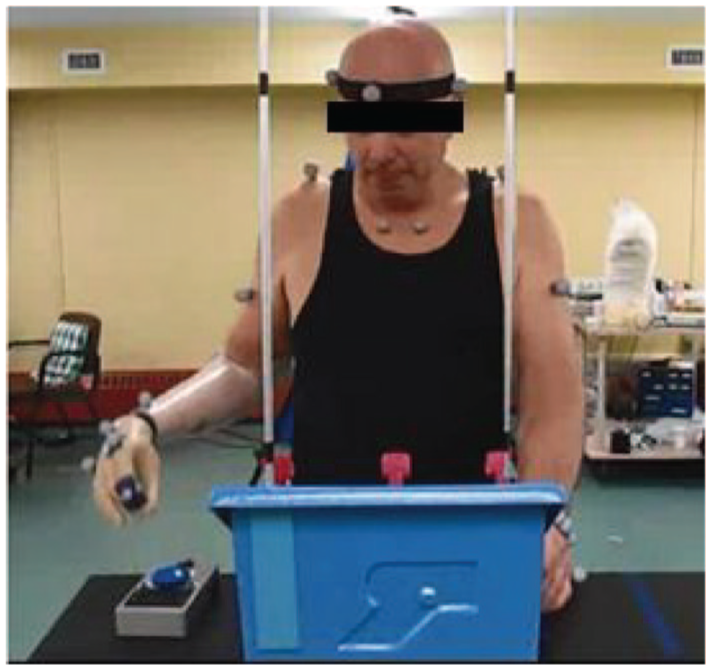
Pinch exerciser showing both vertical rods, though only one is used during any test.
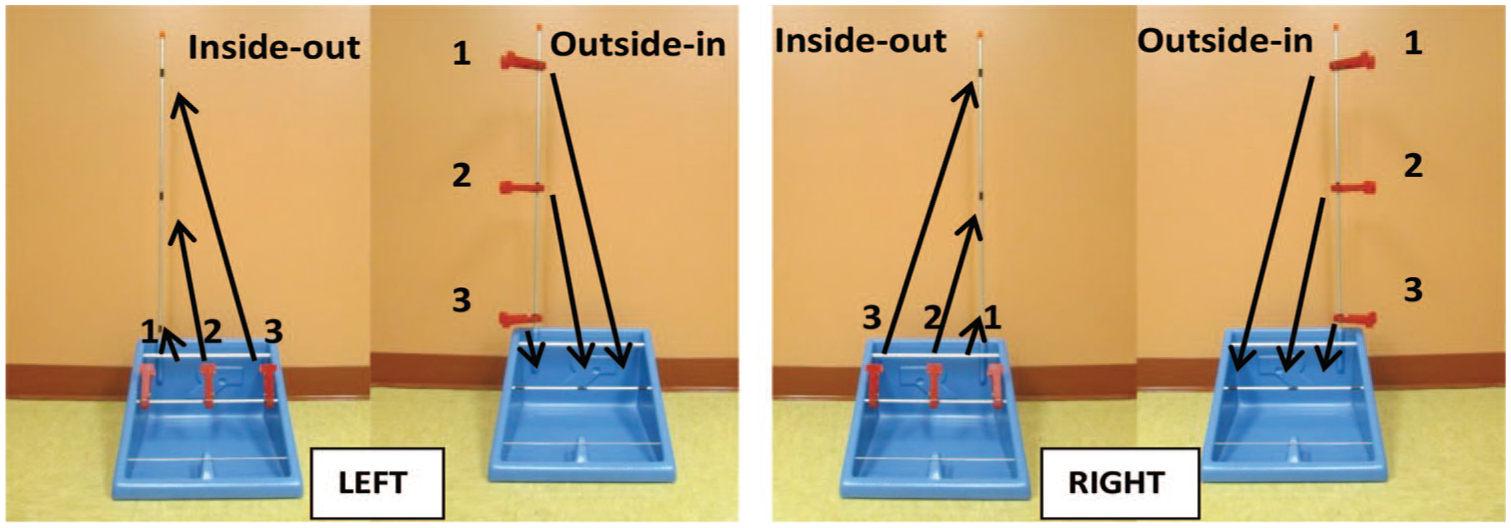
Upwards and downwards assessment order for right- and left-handed RCRT. Numbers indicate the order in which the clothespins are to be moved.
The compensations performed by the subject were assigned an integer grade between 1 and 4 (excessive to no compensation). On the upwards assessment, the trunk lateral tilt was viewed to assign a grade. Grading on the downwards assessment involved viewing the shoulder abduction to decide the grade. Movement of the feet and other motions were penalized by reducing the grade (Appendix 2). Only the first and second clothespin on the upwards direction and only the third clothespin on the downwards direction were used for grading as this is where the largest compensations occurred. 28 The lowest grade was retained. Both upwards and downwards compensatory motions were always assessed on a placement motion (not the grasping motion which was usually optimized by the user following the practice trial).
The RCRT score
The RCRT score combines the average time (five trials) to complete the upwards and downwards trials and the average grade of the compensations. Time was recorded to the 100th of a second and averaged. The average of the compensation grades trials was rounded to the nearest integer. The RCRT score was obtained using the following equation
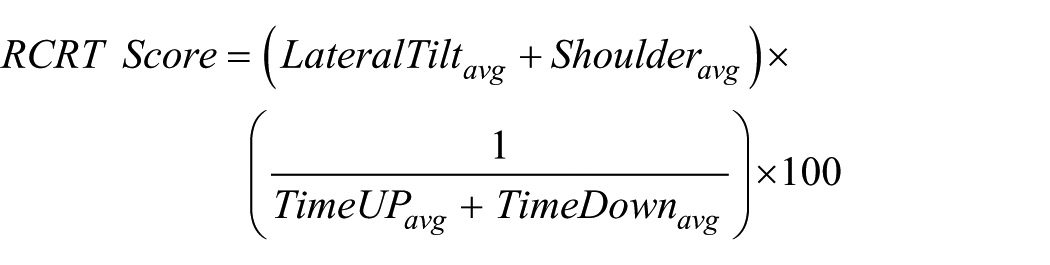
where
Statistical analyses of the data were performed using MS Excel 2010 (Redmond, WA, USA) and IBM SPSS 20 (Armonk, NY, USA). A Mann–Whitney U-test was used to compare the RCRT Score between the able-bodied group and the prosthesis user group (α = 0.05).
Results
The 42 able-bodied subjects (16 men, 26 women; mean age ± SD, 44.21 ± 16.5 years) performed 42 dominant side RCRT tests. Four prosthesis users (4 men; 54.24 ± 5.84 years) performed the test using their regular prosthesis. Subject 4 was not able to complete the RCRT. Therefore, the statistical analyses that follow are only concerned with three completed user RCRTs. The prosthesis user demographics, times, compensation grades assigned and calculated RCRT scores are shown in Tables 1 and 2.
Prosthesis user average times, compensations and scores.
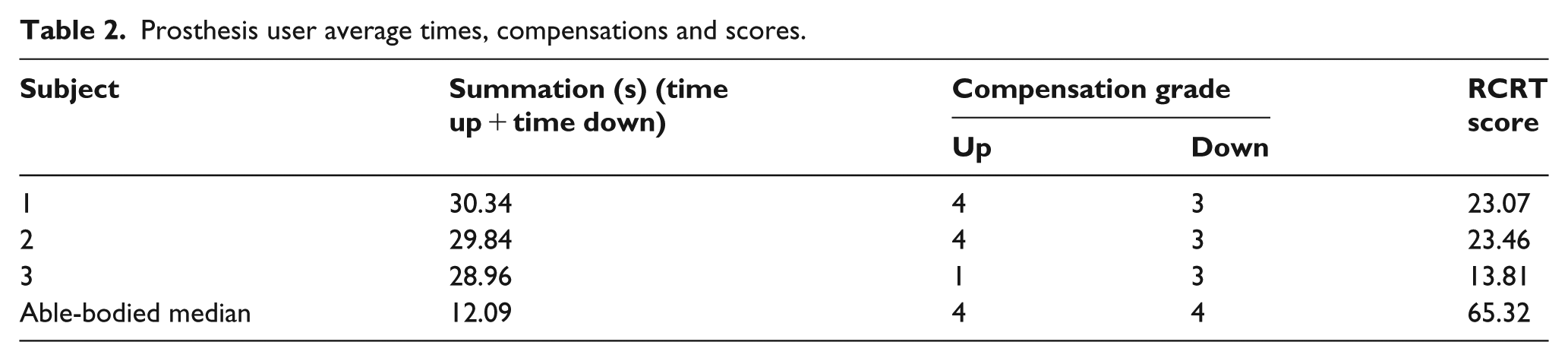
Time to complete
The time to complete the clothespin relocation is represented in Table 2. All three transradial users had times that were at least twice that of the median of the able-bodied subjects.
Compensation grades
The compensation grades for all the prosthesis users were the same in the downwards direction, which means that over the five trials their elbows were raised to the same degree when placing the clothespins on the horizontal rod. The median able-bodied subject grade was 4. This was expected as the ability to position the hand with the wrist, prevented the need to compensate with the shoulder, which caused the higher elbow elevation. In the upwards direction, there was a difference between Subject 3 and the other two users. This individual had a consistent lateral tilt towards his prosthesis and had to move onto his toes for the top clothespin placement, not to be able to reach higher, but to achieve the right position for the hand to approach and grasp the clothespin. Grasping and placement of clothespins required excessive trunk rotation, hip movement and lateral tilt, while moving the elbow inward towards the body, across the midline. He reported an annoying level of pain in the elbow and an uncomfortable pain in the shoulder, and he commented that similar pains are experienced at home when placing items on high shelves and in cupboards. The other users reported no discomfort in any of their joints.
Subject 2 also used a myoelectric hand for the testing and did not have nearly the same level of difficulty as Subject 3. The size and shape of the hand may be a factor (multi-articulating vs single degree of freedom), but a larger set of data would be needed to confirm this.
Regarding the distribution of the assigned compensatory grades, the majority of able-bodied subjects received a grade of 4 in both directions (average across five trials). Able-bodied subjects who moved relatively quickly were observed to over-rotate their shoulder (grade < 4). This was interesting as prosthesis users did this to obtain faster speeds as well, suggesting that minor shoulder compensations were acceptable to both groups if it reduced the time to complete. A biomechanically sound motion was compromised because the time to complete was judged by the subjects to be important. Only prosthesis users were assigned a grade of 1 and 2, reflecting the larger compensations.
RCRT score
The RCRT score resulted in a median value of 65.32 and 23.07 for the able-bodied subjects and prosthesis users that was significantly different (p < 0.001; Figure 3). There is a medium effect size (r = 0.43)
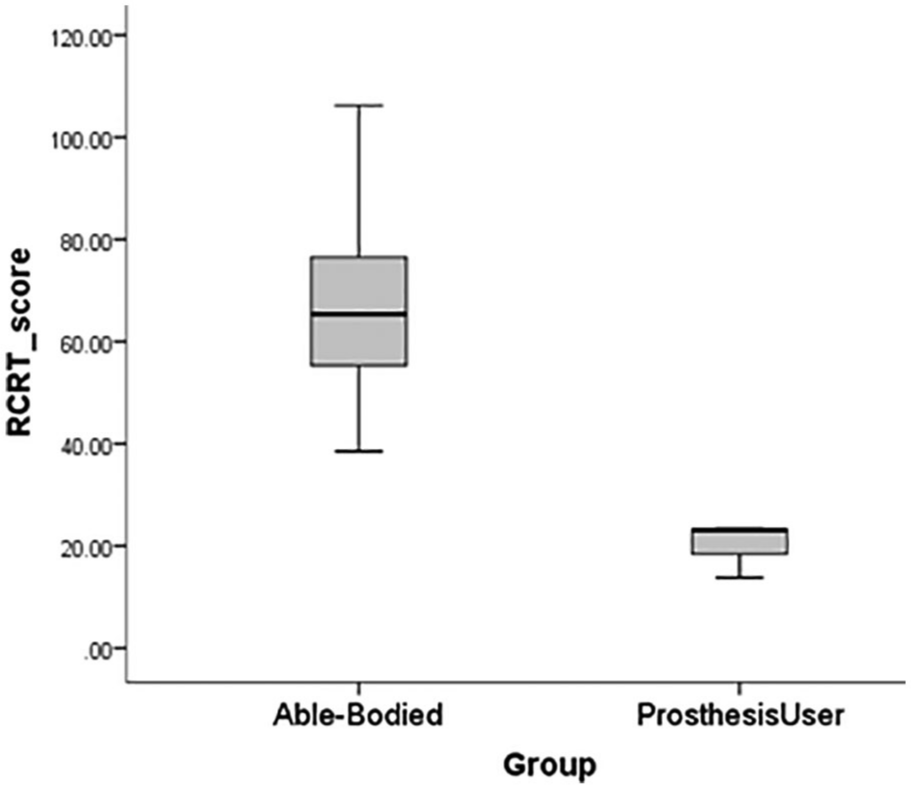
The adapted protocol results in RCRT scores between the transradial prosthesis users and the able-bodied group.
For the able-bodied group, the interquartile range (IQR) was 21.97 with a 95% confidence interval (CI) (61.9, 71.7). The IQR for the prosthesis user group was 4.83. A 95% CI was not calculated because of the small sample size. There is however a clear gap between the maximum prosthesis user score (23.46) and the minimum able-bodied score (38.51).
Discussion
The objective of the RCRT is to evaluate the performance of prosthesis users in their ability to grasp, move and place clothespins with their device. In many prosthetic assessments, the use of compensations to perform a task is not included in the metric used, the focus being on task execution. In a timed task, a subject prioritizes time over compensation reduction and therefore a measure of the quality of motion is not reflected. The RCRT, therefore, aimed to reflect these characteristics into the score. This necessitated adapting the previous protocol for a clinic setting, creating a new metric (RCRT Score) and performing a preliminary evaluation to see if this test could distinguish between prosthesis users and an able-bodied control group.
The RCRT score and the results obtained in this study show a distinct difference between the prosthesis users and the able-bodied subjects. No prosthesis user scored above 25 on this assessment. The medium effect size and the fact that there is no overlap between the groups reflect a gap in the RCRT score. It is anticipated that amputees using powered wrist units and partial hand prosthesis users (with an anatomical wrist) would perform better than subjects in this study. Transhumeral and higher-level involvements by the same logic should fall below the transradial group.
The use of the wrist with the able-bodied subjects resulted in a reduction of compensations of both the shoulder and trunk movements, as it allowed more optimal positioning of the hand. However, simply including a powered prosthetic wrist may not help the prosthesis user, if the control strategy employed (e.g. co-contraction) adds additional time to complete the task. This leads to the dilemma for the prosthesis user, in that the likelihood of employing a second degree of freedom (e.g. wrist or elbow) may be reduced if it is seen to compromise the terminal device’s function. Exploring the concept of how utilization of multiple degrees of freedom within a prosthesis can impact upon each other (and if utilization changes depending on the state of the terminal device), may be a future course of study. Prosthetic devices that use intuitive control strategies, offer simultaneous control, and advanced control strategies (e.g. Pattern Recognition) that provide more natural wrist and elbow activation, may be an advantage to the user, leading to a higher RCRT score. 26
There seemed to be a connection between discomfort and performance, in both the recorded metrics and how the user felt about their performance. Subject 3, whose lower score was more due to compensations on the upwards direction, also said he had a problem when reaching during the test and at home with similar pains in both scenarios. It may be that because the RCRT requires a user to lift their terminal device above the height of the shoulder, the test creates conditions that a user might experience in their daily life.
The small number of prosthesis users limited the study’s ability to see the effect that different prosthetic devices can have with different users and the effect of higher levels of involvement on the RCRT Score. A larger data set would also allow for exploring the potential correlations between the RCRT score and comfort, and increase the statistical confidence of the results presented.
The results from this study warrant further investigation. A repeated-measures study with multiple visits using the same prosthesis can establish whether or not there is a learning effect. A separate study where multiple raters rate the same individuals and the RCRT scores obtained from each rater are compared will expose if any further refinements need to be made to minimize variation in score. In both cases, a larger prosthesis group will be needed to explore the psychometrics of test–retest reliability and validation with prosthesis users, and the effect of inter-rater reliability to establish consistency between raters.
Comparisons with other assessments focused on daily usage would allow a connection between the RCRT results and the user’s usage patterns outside the clinic. A study by Ostlie showed that prosthesis skill displayed in clinic-based tasks may not be indicative of actual prosthesis usage outside the clinic after training, 29 though activities of daily living (ADL) are often employed to provide some semblance of the user’s everyday surroundings in a controlled research environment.14,15 Prosthetic skill in Ostlie’s study was defined as an amalgamated score based on a series of functional activities. The score considered the ability to perform the task, the strain involved and compensatory motions. Actual usage was an index based on whether the user actually performed the clinic-trained task in their daily life. The reduced degree of transfer of trained skills to the user’s life may be due to relevance of the particular ADL being tested, unilateral users using their opposite hand and other factors that will prevent the prosthesis from being employed as intended by the clinician – supporting the need for an updated clinical tool. Lindner et al. 30 discusses the ability to detect clinical change and emphasizes that an outcome from an assessment should assist in making a clinical decision.
Recent study in prosthesis and intact limb activity monitoring, 31 outside the clinic, may allow the clinic team to gain added insight into user performance with clinic-based assessment tools. The distinction between how the user is trained to do a task, whether or not they perform the task in their daily life as trained, and the contribution of an additional anatomical limb during task execution informs the discussions regarding compensation, discomfort and satisfaction that the RCRT investigates.
Conclusion
This study showed that the RCRT test readily distinguishes between users and able-bodied subjects, and that prosthesis users performed larger compensation in their trunk and shoulder to perform the RCRT, which was reflected in the scores. Future study to establish the psychometrics needed for validation and reliability will need to be performed before the RCRT can be introduced into a clinical environment where it may assist in establishing functional performance with a prosthetic device.
Supplemental Material
843779_A1_supp_mat – Supplemental material for Clinical evaluation of the refined clothespin relocation test: A pilot study
Supplemental material, 843779_A1_supp_mat for Clinical evaluation of the refined clothespin relocation test: A pilot study by Ali Hussaini, Wendy Hill and Peter Kyberd in Prosthetics and Orthotics International
Supplemental Material
843779_A3_supp_mat – Supplemental material for Clinical evaluation of the refined clothespin relocation test: A pilot study
Supplemental material, 843779_A3_supp_mat for Clinical evaluation of the refined clothespin relocation test: A pilot study by Ali Hussaini, Wendy Hill and Peter Kyberd in Prosthetics and Orthotics International
Supplemental Material
843779_Appendix_A2_RCRT_GradingCompensations_(2) – Supplemental material for Clinical evaluation of the refined clothespin relocation test: A pilot study
Supplemental material, 843779_Appendix_A2_RCRT_GradingCompensations_(2) for Clinical evaluation of the refined clothespin relocation test: A pilot study by Ali Hussaini, Wendy Hill and Peter Kyberd in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors would like to thank the
Authors’ Note
Peter Kyberd is now affiliated with Faculty of Technology, University of Portsmouth, Portsmouth, Hampshire, UK.
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Natural Sciences and Engineering Research Council of Canada and the New Brunswick Innovation Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.