
Abstract
Background and Objectives: The prevalence of back pain and its effect on function and health-related quality of life across three levels of lower limb amputation secondary to trauma or tumour was studied.
Study design: Cross-sectional survey.
Methods: Forty-six lower limb amputees, aged 19–78 years, participated. The Roland Morris disability questionnaire (RMDQ) and the short form 36 health survey (SF-36) were used.
Results: Participants reported more back pain after amputation than before (p < 0.001). There was a significant association between back pain daily or several times/week and severe or moderate disability reporting on the RMDQ (p = 0.003). On the SF-36, the group as a whole scored significantly lower in health-related quality of life with regard to physical functioning, role physical, bodily pain, general health, social functioning and the physical component summary (PCS), and significantly higher in the mental component summary (MCS) compared to normative Swedish data. When all three levels of amputation were compared, no statistically significant differences were found in the RMDQ or SF-36 results.
Conclusions: There was a high prevalence of back pain after amputation. Almost all participants having back pain daily or several times per week reported severe or moderate disability on the RMDQ. The group as a whole scored significantly lower for health-related quality of life in the PCS and significantly higher in the MCS compared to normative Swedish data.
The high prevalence of back pain, and the significant association between back pain daily or several times per week and severe or moderate disability on the RMDQ, and the negative correlation between RMDQ and SF-36, may have clinical relevance with regard to rehabilitation and follow-up of lower limb amputation.
Introduction
Leg amputations are the most common of all amputations and are mainly caused by vascular disease with or without diabetes. 1,2 In Sweden these illnesses cause 90% of all leg amputations. 3 From 1998 to 2006, 719 persons were amputated due to trauma or tumour. Of these, 278 were transfemoral, 149 were knee disarticulation and 292 were transtibial amputations. 4,5
Transfemoral amputees are functionally the most limited. The muscles directly controlling the knee joint are lacking and functional restrictions of the prosthetic knee joint may also contribute to a higher energy cost. 6 The use of an increased pelvic tilt and Trendelenburg gait to maintain knee stability and reduce the lever arm of the hip abductors 7 often leads to back pain. 8 Transtibial amputees have better biomechanical prerequisites compared to transfemoral and knee disarticulation amputees. 6,9,10 There is evidence that distal and unilateral amputees have better walking ability 11 and walk faster 12 than transfemoral amputees. Amputees use more energy whilst walking than healthy individuals and the amount of energy used increases with higher levels of amputation. 13,14
Phantom and stump pain are usually associated with amputations and it appears that back pain has not been studied to the same extent. 15 We have not found any studies examining the prevalence of back pain among lower limb amputees in Sweden. Back pain has, however, been shown to occur frequently among lower extremity amputees, and has been reported as persistent and chronic by 52–72% of participants with different levels of amputation caused either by trauma or other illnesses (tumour/dysvascular). 8,15 In yet another study, prevalence of low back pain among transfemoral amputees was frequent to permanent in 26.3% of the sample. 16
Back pain even at a moderate level has been shown to interfere with daily activities, 17 which may lead to the perception of low health-related quality of life. 18 Of two previous studies that examined pain and pain interference with physical function and daily activities, one reported no difference among three levels of amputation in lower limb amputees 15 and the other found that knee disarticulation amputees reported less interference with physical function from back pain than transtibial or transfemoral amputees. 19 In these studies several diagnoses were included, e.g. diabetes, vascular disease, trauma and tumour. 15,19 Amputation due to trauma or tumour affects mainly persons who are younger and in other respects healthy. 1,20 They are therefore more able to readjust and return to their normal life than dysvascular amputees. We chose to examine the prevalence of back pain and its effect on function and health-related quality of life in lower limb amputees secondary to trauma or tumour. We have not found any study using RMDQ to investigate the influence of back pain on function in lower limb amputees. We found one study that examined health-related quality of life among Swedish lower limb amputees secondary to trauma or tumour as measured by the SF-36, 18 and none comparing perceived health-related quality of life across three levels of lower limb amputation.
The aim of our study was to investigate the prevalence of back pain and its influence on function, and to examine the self-reported health-related quality of life among Swedish lower limb amputees secondary to trauma or tumour across three levels of lower limb amputation.
Subjects
The ethical committee recommended that participants first be contacted by the person who was their main care-giver, for example, the orthopaedic surgeon, physiotherapist or prosthetist. This procedure would ensure that patients felt free to refrain from participating. All orthopaedic and prosthetic clinics in the southern region of Sweden (Lund, Helsingborg, Malmö, Kristianstad and Ängelholm) were contacted by a letter addressed to the whole team inquiring whether they would consider participating. They all accepted and agreed to contact patients who met the inclusion criteria. To our knowledge none of the patients who were asked to participate declined. Patients who agreed to participate received both written and oral information stating the aim of the study and how it would be carried out. The inclusion criteria were (a) having had a transfemoral, knee disarticulation or transtibial amputation due to trauma or tumour, (b) above 18 years of age, (c) continuous prosthetic user, (d) fitted with a prosthesis, (e) rehabilitation completed at least two years earlier and (f) able to understand written and spoken Swedish.
Description of the participants (n = 46), level of amputation, age, years since amputation, cause of amputation, use of the prosthesis days/week and hours/day and use of walking aids indoors and out of doors. Age and years since amputation in mean and range within brackets.
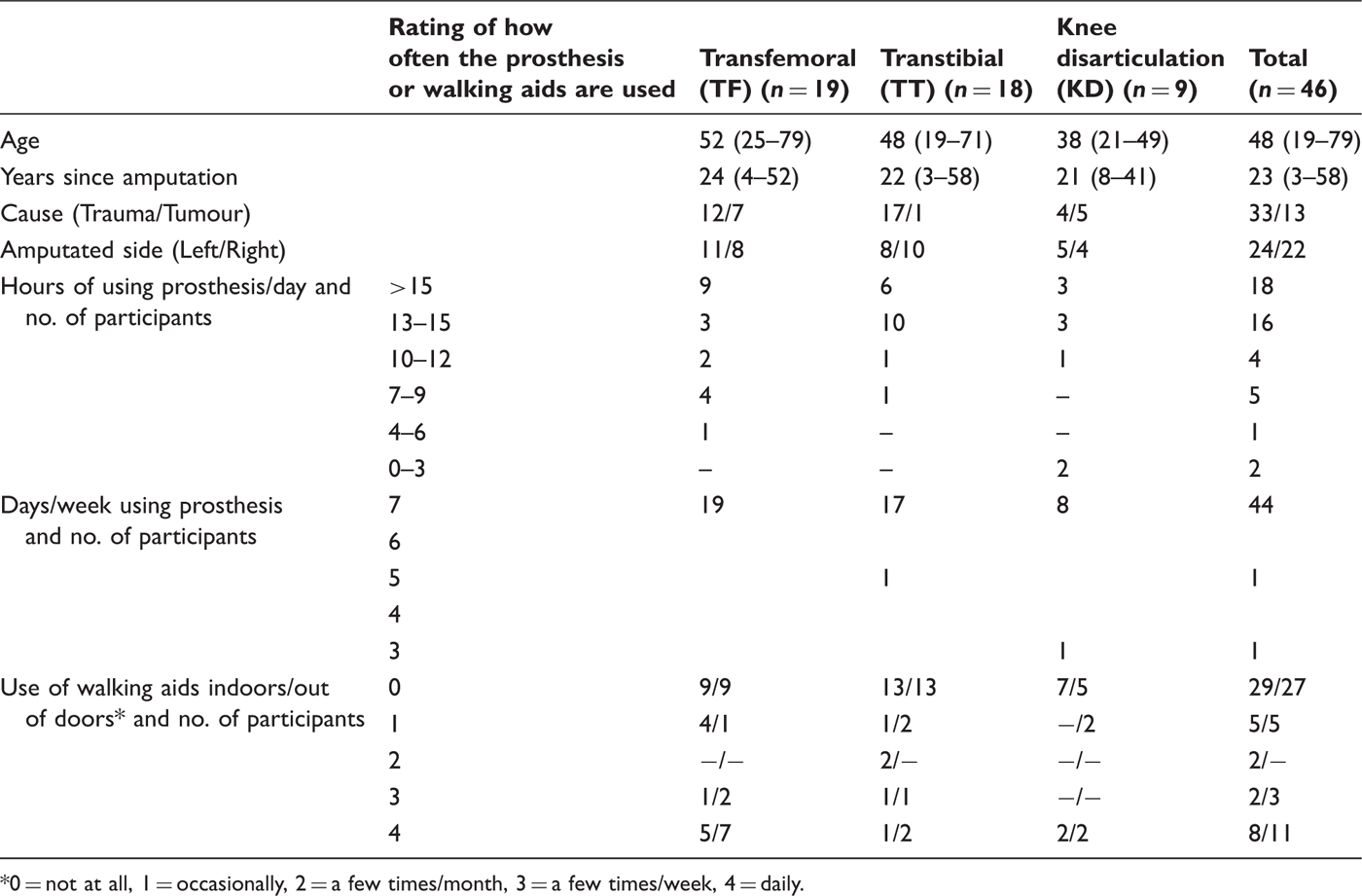
0 = not at all, 1 = occasionally, 2 = a few times/month, 3 = a few times/week, 4 = daily.
The majority (n = 44) used their prosthesis seven days per week, and two used their prosthesis 5 and 3 days per week, respectively. The prosthesis was used more than 9 hours per day by 38 participants (83%). More than half managed without walking aids indoors (n = 29, 63%) and outdoors (n = 27, 59%) (Table 1).
Those who did not participate were 17 men and 5 women with a mean age of 48 years (31–72). No other information could be accessed regarding demographic or medical data.
Ethics
The Ethics Committee for Caring Sciences at Lund University approved the study (VEN A45-07). All patients who agreed to participate received both written and oral information stating the aim of the study and how it would be carried out. All signed informed consent for participation and publication.
Method
Three questionnaires were sent simultaneously by mail to all participants: (1) a questionnaire investigating demographic data and prevalence of back pain, (2) the Roland Morris disability questionnaire and (3) the short form 36 health survey (SF-36).
Demographic data and prevalence of back pain
In addition to demographic data such as age, gender and years since amputation, questions were asked regarding extent of prosthetic use, walking aids and prevalence of back pain. The participants were asked (1) ‘Did you ever suffer from back pain before the amputation?’ and (2) ‘Have you ever had back pain after the amputation?’. Five alternatives were allotted to each question: (a) no; (b) yes, occasionally; (c) yes, a few times a month; (d) yes, several times a week; (e) yes, daily. The questionnaire was first tested on seven amputees at the Department of Rehabilitation for Amputees at Lund University Hospital. These amputees did not participate in the study.
Roland Morris Disability Questionnaire
The Roland Morris Disability Questionnaire (RMDQ) was used to investigate functional capacity in relation to perceived back pain. The RMDQ and the Oswestry disability questionnaire were found to be best suited to detect back pain when compared to nine different self-reporting questionnaires. 21 The RMDQ was chosen as it is well tested for reliability and validity and used internationally for research and in clinical settings. 22,23,24 The questionnaire consists of 24 statements with the alternatives yes or no, and is especially designed for people with back pain. It focuses on functional ability, i.e. the ability to sit, stand and manage everyday activities. The sum of all yes answers is calculated. The more yes answers, the greater the influence of back pain on functional ability. Roland and Morris suggest that 14 points and above should be interpreted as severe disability. 22 The Swedish version was published and tested in 1998 for test–retest reliability and concurrent validity, though not on amputees 23 but on patients with chronic and sub-acute low back pain. The result was a mean score of 9.3 (SD 5.0). 23
Short Form 36 Health Survey
To measure health-related quality of life the short form 36 health survey (SF-36) was chosen. The SF-36 has been used in more than a thousand publications including more than 130 diagnoses, and has frequently been used when studying back pain. 25 The SF-36 has been tested for reliability and validity 26,27,28 and aims to measure self-reported physical and psychological health. It consists of 36 statements that can be subdivided into eight health-related concepts: (1) physical functioning, (2) role physical: role limitations due to physical health problems, (3) bodily pain, (4) general health, (5) vitality: energy levels/fatigue, (6) social functioning, (7) role emotional: role limitations due to emotional problems, and (8) mental health: psychological distress. These eight concepts may also be grouped into two summary measures, the physical component summary (PCS) and the mental component summary (MCS), 29 each of which summarises four scales. The PCS includes physical functioning, role physical, bodily pain and general health. The MCS includes vitality, social functioning, role emotional and mental health.
Data analysis
Results were analysed in SPSS 15.0 and Microsoft Excel 2003. The Wilcoxon signed-ranks test was used to calculate the prevalence of back pain before and after amputation, and the high/low scores on the RMDQ and prevalence of back pain. The Kruskal-Wallis H and the Mann Whitney U tests were used to analyse the results of the SF-36. The Spearman’s rank correlation coefficient was used for analysis of correlation between the RMDQ and the SF-36. All results from the SF-36 were exploratively calculated using the one-sample t-test to investigate the difference between all participants and each subgroup compared to the Swedish normative data. All values were calculated using the Bonferroni method, which can be applied in two ways. We chose to multiply the observed significance value (P) by the number of independent significance tests (k). If any kP is less than or equal to 0.05 the result is regarded as significant at the 0.05 level. 30
Results
Prevalence of back pain
There were 33 trauma and 13 tumour amputees. Of these, there were about twice as many transfemoral and transtibial amputees as knee disarticulation amputees (Table 1). In order to make the representation of each subgroup clearer to the reader, results are therefore presented as both the number of persons (n) and as a percentage (%).
Self-reported prevalence of pain in lower limb amputees secondary to trauma or tumour before and after amputation (n = 46). Rating of how often pain occurs (0 = not at all, 1 = occasionally, 2 = a few times/month, 3 = several times/week, 4 = daily).
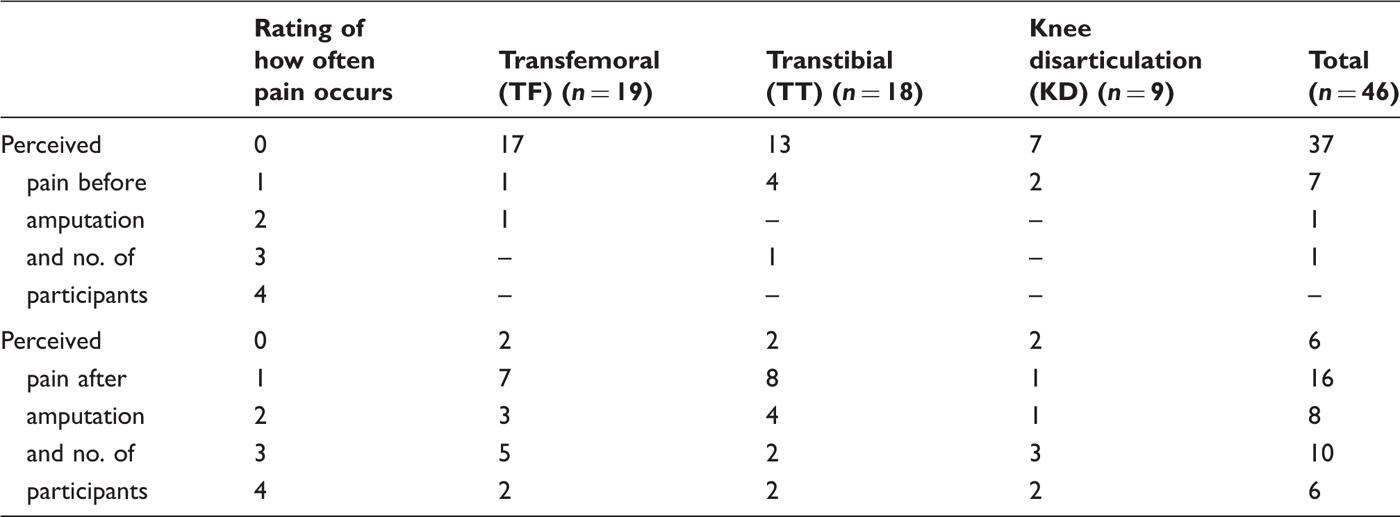
Regarding the prevalence of back pain after amputation, 16 participants (35%) reported having back pain ‘daily’ or ‘several times a week’, distributed over transfemoral (n = 7, 37%), knee disarticulation (n = 5, 56%) and transtibial (n = 4, 22%) amputations (Table 2). No group had significantly higher perception of back pain before amputation, when comparing level of amputation (transfemoral, knee disarticular, transtibial) or cause of amputation (trauma/tumour).
Roland Morris Disability Questionnaire
There was no significant difference when comparing the RMDQ scores among transfemoral, knee disarticulation and transtibial amputees.
Severe disability, 14–16 points, was reported by three participants (7%) and moderate disability, 8–13 points, was reported by nine participants (20%). Twenty-seven participants (59%) scored 0–3 points. Of these, some indicated some problems caused by back pain during their daily activities.
There was a significant association between participants who reported having back pain daily or several times per week and those who reported severe or moderate disability on the RMDQ (p = 0.003).
Short Form 36 Health Survey
Results from SF-36 in the scales Physical Functioning, Role Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role Emotional, Mental Health and the two summary scores Physical Component Summary (PCS) and Mental Component Summary (MCS), for all participants (n = 46) and for the different subgroups: the amputation level (transfemoral (TF), transtibial (TT), knee disarticulation (KD)), cause (trauma and tumour) and compared to normative Swedish data. High scores indicate better functioning and more positive assessment of health-related quality of life. Standard deviation (sd) in brackets. One-sample t-testing was used to explore the difference between each subgroup and all participants compared to normative Swedish data.
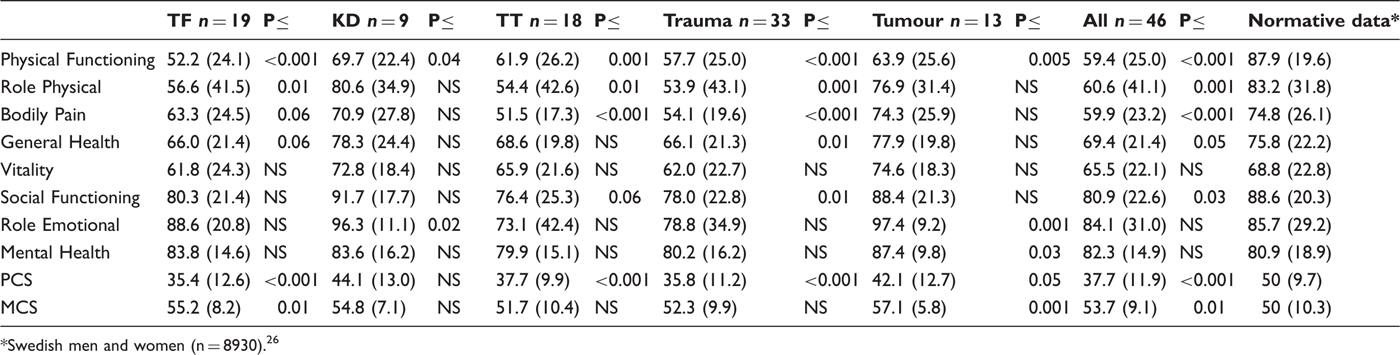
Swedish men and women (n = 8930). 26
In the PCS and MCS scores, all subgroups, with the exception of the knee disarticulation amputees, reported a significantly lower perception of health-related quality of life in PCS compared to normative Swedish data (Table 3). All reported a higher health-related quality of life in the MCS, which was significant for the transfemoral amputees secondary to tumour and also for the group as a whole compared to the normative Swedish data (Table 3).
Compared to the Swedish normative data, physical functioning and role physical were significantly lower among the transfemoral amputees (Table 3).The transtibial amputees had significantly lower physical functioning, role physical and bodily pain when compared to the normative Swedish data. In the knee disarticulation amputees, physical functioning was significantly lower and role emotional was significantly higher than the normative Swedish data (Table 3). When all three levels of amputation were compared, no statistically significant differences were found in the results of the SF-36.
When comparing cause of amputation, the participants with an amputation secondary to tumour scored significantly lower compared to the normative Swedish data regarding physical functioning, and significantly higher for role emotional and mental health (Table 3). Participants with an amputation due to trauma scored significantly lower compared to the normative Swedish data regarding physical functioning, role physical, bodily pain, general health and social functioning (Table 3). The differences between trauma and tumour amputees were statistically significant in the dimension of bodily pain (p = 0.01).
Correlation between RMDQ and SF-36
Negative correlation between the results on Roland Morris Disability Questionnaire (RMDQ) and Short Form 36 Health Survey (SF-36) calculated by use of Spearman’s rank correlation coefficient in three levels of amputation secondary to trauma or tumour (n = 46). High values on RMDQ indicate functional disability and reduced functional capacity in relation to perceived back pain and low values on SF-36 indicate negative assessment of health-related quality of life.
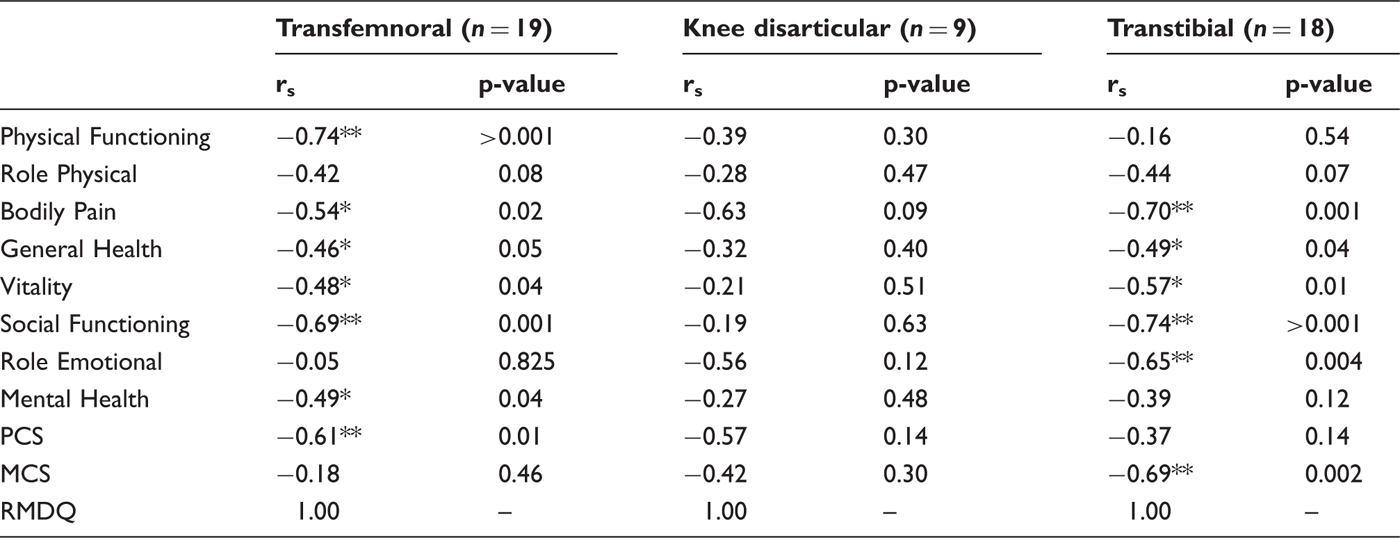
This correlation was significant among the transfemoral amputees regarding physical functioning, bodily pain, general health, vitality, social functioning, mental health and the PCS score (Table 4). Among transtibial amputees this correlation was significant regarding bodily pain, general health, vitality, social functioning, role emotional and the MCS score (Table 4). There was no statistically significant correlation between the RMDQ and the SF-36 for the knee disarticulation amputees. Values for bodily pain (rs −0.63), role emotional (rs −0.56) and the PCS score (rs −0.57) show a moderate negative correlation, though not statistically significant (Table 4).
Discussion
The participants reported significantly more back pain after amputation than before (p < 0.001). They had been amputated for 23 years on average and had been prosthetic users for a long time. They were regarded as active prosthetic users as 44/46 used their prosthesis 7 days per week and the majority (n = 38, 83%) used their prosthesis more than 9 hours per day. This study excluded dysvascular amputees because they are usually limited physically due to disease-related symptoms and therefore less active prosthetic users. 1,19,31
Low back pain has been shown to be more common among transfemoral amputees than transtibial amputees. 32,33 In the present study, however, the prevalence of back pain did not differ between the three levels of amputation. This has also been supported by another study. 15
Participants rated the prevalence of back pain retrospectively, and as many years had elapsed since amputation this may have caused some unreliability in the data. However, 35% reported having back pain daily or several times per week after amputation, which may indicate a prevalence of chronic back pain after amputation, compared to 18.9% prevalence in the Swedish population. 34
Using questionnaires may have had some disadvantages as it is unclear why people chose not to participate. Those with little or no pain may have felt that the questionnaires did not concern them and therefore did not answer. The number of respondents might have increased had patients been given clearer and more explicit information as to the importance of participating even if no physical or psychological problems were perceived.
Although the participants reported increased back pain after amputation, the majority (59%) reported some or no reduction in functional capacity due to back pain. One explanation of this result may be the wording of the items in the questionnaire examining prevalence of back pain. Another explanation may be that the RMDQ offers only two alternatives, yes or no. The situation of amputees is complex as they may perceive pain related to the stump or phantom pain. 20,35 It is therefore possible that other causes were more prominent than perceived back pain at the time of filling in the questionnaire, as participants are requested to give an account of how they perceive the pain on that day. Although every statement in the RMDQ includes the words ‘because of my back pain’, we cannot be sure if the back pain among this group of amputees was related only to the amputation or to other causes.
Three persons scored 14–16 points, which, according to Roland and Morris, should be interpreted as having a severe disability. 22 Johansson and Lindberg tested the RMDQ on 72 patients with chronic and sub-acute low back pain. 23 The result was a mean score of 9.3 (SD 5.0), leading the authors to suggest that the level of 14 points may be set too high for this group of patients. 23 In another study with patients suffering from chronic back pain the result of the RMDQ was divided into two scores, where 0–12 was interpreted as minimal disability and 13–24 as significant disability. 36 Based on these results, the nine participants (20%) who scored 8–13 points were classified as having moderate disability.
There was a significant association between participants reporting back pain daily or several times per week and those who reported severe or moderate disability on the RMDQ (p = 0.003). When comparing the RMDQ scores across the three levels of amputation, no significant differences were found in any of the subgroups. This may be due to the groups being small and unequal in size and the back pain being evenly distributed across the subgroups. In another study, knee disarticulation amputees reported less interference of back pain with physical function than did the transtibial or transfemoral amputees. 19
In general, the health-related quality of life regarding physical functioning was rated poorer than psychological functioning, which was in turn significantly better than the Swedish normative data, with the exception of the knee disarticulation amputees. The rating of perceived pain was in agreement with other studies showing that amputees may feel stump, phantom and back pain. 32,33,37
The low scores for physical functioning among the transfemoral amputees were in line with previous research. 38 The transtibial amputees reported the lowest scores on health-related quality of life compared to other levels of amputation for role physical, bodily pain, social functioning and role emotional as well as the MCS score.
The tumour amputees reported higher scores on all eight scale profiles and the summary scores, indicating that they perceived better physical and mental health than trauma amputees. This has also been observed by others. 39 One explanation may be the use of appropriate coping strategies, e.g. downward comparisons, 40 or having found a way to make sense of the amputation, as has been found in cancer patients. 40,41 This may explain why health-related quality of life was higher for participants amputated due to tumour than those amputated due to trauma.
A significant negative correlation was shown between the RMDQ and the SF-36 regarding bodily pain, general health, vitality and social functioning in transfemoral and transtibial amputees. In knee disarticulation amputees there was a moderate negative correlation regarding bodily pain (rs −0.63), role emotional (rs −0.56) and the PCS score (rs −0.57), which might have been significant had the number of participants been comparable to those in the other two groups.
Although the Spearman’s rank correlation assesses a general association 42 and is not usually influenced by skewed data, 43 we chose to report both the correlation coefficient and the p-value. One reason for this choice was that the groups were small and unequal in size, and the knee disarticulation amputees were represented by only nine participants.
These results are not conclusive, however, as the study has several limitations. The sample is small and the subgroups of unequal size, which means that the results may not be generalizable. Also, the recollection of perceived back pain before amputation was backdated several years, which may have introduced unreliable data.
Further controlled studies are needed to evaluate the relationships between pain, perceived health-related quality of life, psychological aspects and functional capacity.
Conclusion
There was a high prevalence of back pain after amputation. Almost all participants having back pain daily or several times per week reported severe or moderate disability on the RMDQ. When all three levels of amputation were compared, no statistically significant differences were found in the RMDQ or SF-36 results. The group as a whole reported health-related quality of life as significantly lower in the PCS score and significantly higher in the MCS score compared to the normative Swedish data.
Footnotes
Funding
This study was supported by grants from the Gyllenstiernska Krapperups Foundation and the Medical Faculty of Lund University.