
Abstract
Study Design
Narrative review.
Objective
Our objective was to provide an evidence-based summary of how symptoms (severity/duration) impact timing of surgery for adult spinal deformity (ASD).
Methods
The authors queried PubMed, MEDLINE, and Scopus to identify potentially relevant studies. Articles were included based on quality of design, methodology, assessment of symptoms (back/leg pain, neurological deficits) and other factors which could influence timing of surgery.
Results
Database query produced 138 potentially relevant studies. Review of these studies and relevant references generated 29 studies that were included. Back and leg pain were the most common assessed symptoms: NRS back pain (nonoperative 4.4-5.3, operative 6.3-7.1) and NRS leg pain (nonoperative 2.3-4.1, operative 4.2-5.4). Leg pain was an independent predictor of surgery. Back/leg pain positively correlated with disability and worse health status, which were important factors driving surgery. ODI ≥40 was identified as a potential disability threshold associated with surgery. Few studies (n = 2) provided assessment of neurological deficits, and development of weakness was associated with surgery. Symptom duration was assessed using post hoc analysis of nonoperative to operative crossover (n = 6; mean time to crossover 0.8-1.1 years).
Conclusions
Our results suggest at least moderate symptoms should be present prior to considering surgery. Less data exists for symptom duration and is from studies reporting nonoperative to operative treatment crossover. Future research is needed to determine clinically meaningful differences in validated outcome instruments for baseline comparisons prior to treatment, provide more detailed assessments of leg pain (radiculopathy vs claudication) and deficits, and include dynamic functional testing.
Keywords
Introduction
Early literature by Weinstein et al reported that untreated late-onset idiopathic scoliosis caused little physical impairment other than back pain and cosmetic concerns.1,2 Although these early studies had 50-year follow-up and represented a monumental effort at the time, an important limitation included lack of sagittal plane radiographic analysis. Since then, considerable progress has been made towards further understanding adult spinal deformity (ASD) and its impact on health status.3-7 Notably, a consistent finding has been that the late-onset idiopathic scoliosis patients investigated by Weinstein et al likely represented only a subset of ASD, which is now considered a more heterogenous and diverse pathological entity.5,6,8,9 Furthermore, substantial research has provided significant evidence demonstrating that symptomatic ASD patients report greater functional limitations, greater daily analgesic use, and worse health-related quality of life (HRQL) and disability compared to the general population and other chronic disease states.5-7,10,11 As such, determining the symptoms (e.g., back and/or leg pain) associated with ASD, both in terms of magnitude/severity and duration, as well as the degree of associated disability, which may impact treatment decision-making for both patients and healthcare providers, has emerged as an important topic of investigation.
Early studies by Smith et al demonstrated that symptomatic ASD patients often presented to surgical clinic with complaints of back pain, leg pain, weakness, and other neurological deficits.12-14 Assessing the severity of these preoperative symptoms using validated health outcome measures may provide benchmark scores to guide timing of surgical intervention. Moreover, analyzing the onset and duration of preoperative symptoms could also be useful to facilitate patient counseling and timing of surgery. Currently, limited literature exists for the severity and duration of symptoms reported by ASD patients, and even less is known about the progression of symptoms and how this may impact timing of surgical intervention.
Despite trials of nonoperative treatment, some ASD patients may experience refractory symptoms and ultimately transition from nonoperative to operative care.9,12,15 This transition is likely governed by multiple factors which may include progressive deformity, worsening symptoms of back/leg pain, and increasing disability with an associated decline in functional health status.9,12,15 Operative ASD treatment can provide significant benefits but is associated with high complication rates, and discussion of these risks may also impact the treatment decision-making process.16-26 In this narrative review, we focused on the symptoms (e.g., back/leg pain and associated disability) which may impact the timing and decision-making process to pursue operative treatment for ASD. Our objective was to review current concepts which may elucidate ASD symptomology in terms of both magnitude/severity and duration, and provide an evidence-based framework for potentially planning a future multicenter prospective investigation.
Methods
The current authors performed a narrative review of ASD thoracolumbar literature to investigate timing of operative treatment based on presenting and/or worsening symptomatology. We queried PubMed, MEDLINE, and Scopus using the search terms “operative,” “nonoperative,” “adult,” and “scoliosis” without applying specific exclusion criteria based on study publication date. This initial query generated 138 potentially relevant articles, which were then reviewed by assessing the title and/or abstract details. For some queried articles, further assessment of the full text was also performed. In these cases, additional referenced articles that were potentially relevant to the objective of this narrative review were also reviewed for possible study inclusion. Higher priority was assigned to studies that utilized prospective multicenter methodology, comprised larger patient cohorts (preferentially ≥100 ASD patients), and reported results (specific data values and not only figures/charts) with standardized patient-reported outcome measures (PROMs: Oswestry Disability Index [ODI], 27 36-Item Short Form Health Survey [SF-36] Physical/Mental Component Summary [PCS/MCS], 28 Scoliosis Research Society-22-r Patient Questionnaire [SRS-22]29,30). Also, preference was given to studies comprised mainly of ASD patients with diagnosis of adult idiopathic scoliosis, de novo degenerative scoliosis, and/or flatback deformity. Studies primarily focused on congenital or neuromuscular scoliosis were excluded. Studies without radiographic criteria for adult spinal deformity (e.g., scoliosis ≥20°, SVA ≥5 cm, pelvic tilt ≥25°, thoracic kyphosis ≥60°) were excluded. The present review focuses on thoracic, thoracolumbar, lumbar, or lumbosacral spinal deformity; therefore, any articles with primary focus on cervical spinal deformity were not included.
All relevant articles, as deemed so by the authors, were then studied in full detail. The goal of the present study was to provide evidence-based narrative review. As such, final inclusion of queried articles was not based on systematic process methodology, but instead was based on specific relevance to one of the following subcategories of interest: (1) articles assessing symptoms and/or other factors that could potentially influence ASD surgical decision-making and the conversion from nonoperative to operative treatment, (2) articles with primary objective to compare operative vs nonoperative treatment outcomes for ASD (these had to provide analysis of baseline PROMs for inclusion in the present review), (3) articles analyzing the results of dynamic functional testing between operative vs nonoperative ASD patients, and (4) articles presenting decision-making algorithms or appropriateness criteria for operative vs nonoperative treatment of ASD.
Results
Articles with Primary Focus to Analyze Presenting Symptoms in Operative vs Nonoperative Cohorts
Articles Assessing the Symptoms or Other Factors Which May Impact the Transition From Nonoperative to Operative Treatment.
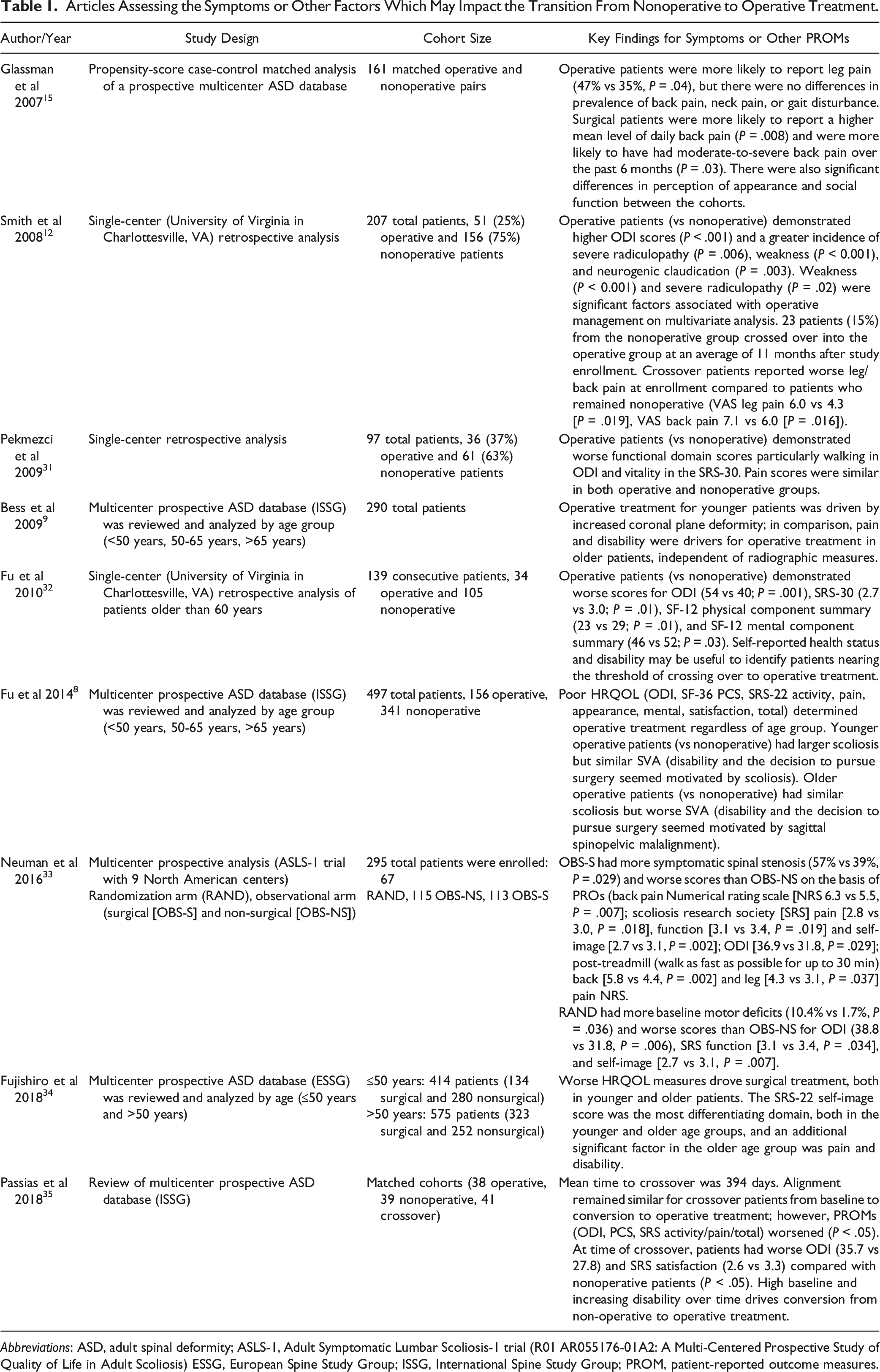
Abbreviations: ASD, adult spinal deformity; ASLS-1, Adult Symptomatic Lumbar Scoliosis-1 trial (R01 AR055176-01A2: A Multi-Centered Prospective Study of Quality of Life in Adult Scoliosis) ESSG, European Spine Study Group; ISSG, International Spine Study Group; PROM, patient-reported outcome measures.
Of these 9 studies (Table 1), 2 included neurological assessment with reports of presenting motor weakness/deficits (Smith et al and Neuman et al).12,33 Development of radicular weakness or neurogenic claudication were strongly associated with the decision to pursue operative treatment.12,33
Of these 9 studies (Table 1), 3 included data describing symptom duration.12,15,35 Glassman et al reported patients who underwent surgery were more likely to have had moderate-to-severe back pain in the past 6 months prior to presentation. 15 The remaining 2 articles (Smith et al and Passias et al) reported symptom duration by analyzing patients crossover from nonoperative to operative treatment during study follow-up.12,35 Smith et al reported 23 patients (15%) who had initially been classified into the nonoperative group crossed over into the operative group at a mean interval of 11 months after enrollment. 12 These crossover patients reported significantly higher Visual Analog Scale (VAS) scores for leg and back pain at enrollment compared to patients who remained in the nonoperative cohort (VAS leg pain: 6.0 vs 4.3, P = .019; VAS back pain: 7.1 vs 6.0, P = .016). 12 For the crossover patients, Smith et al reported that the principal symptom prompting surgery was radicular pain (n = 14), back pain (n = 5), and equivalent radicular and back pain (n = 4). Notably, progressive neurological deficits also developed in 3 patients. 12 Nearly a decade later (2018), Passias et al 35 also investigated the patient profile and risk factors for crossing over from nonoperative to operative care. The authors reported a mean time to crossover of 13 months for 41 patients (21.7%). 35 High baseline and increasing disability (ODI, PCS, SRS Activity, Pain, and Total scores) over time likely drove the conversion from nonoperative to operative ASD treatment. 35
Articles Comparing Operative vs Nonoperative Treatment Outcomes
Articles Comparing Operative vs Nonoperative Treatment Outcomes With Analysis of Baseline PROMs.
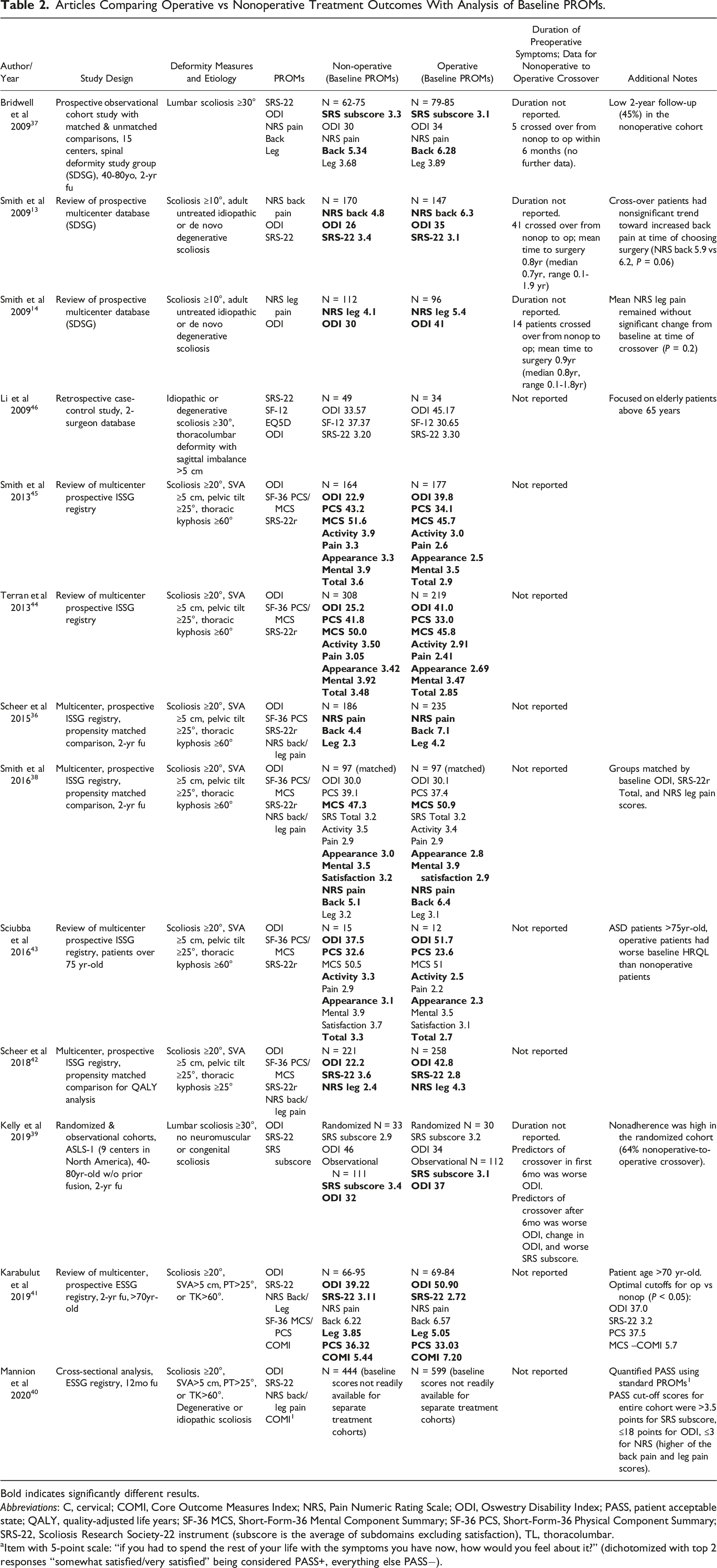
Bold indicates significantly different results.
Abbreviations: C, cervical; COMI, Core Outcome Measures Index; NRS, Pain Numeric Rating Scale; ODI, Oswestry Disability Index; PASS, patient acceptable state; QALY, quality-adjusted life years; SF-36 MCS, Short-Form-36 Mental Component Summary; SF-36 PCS, Short-Form-36 Physical Component Summary; SRS-22, Scoliosis Research Society-22 instrument (subscore is the average of subdomains excluding satisfaction), TL, thoracolumbar.
aItem with 5-point scale: “if you had to spend the rest of your life with the symptoms you have now, how would you feel about it?” (dichotomized with top 2 responses “somewhat satisfied/very satisfied” being considered PASS+, everything else PASS−).
Score Ranges for Baseline PROMs Extracted From Operative vs Nonoperative ASD Studies. 1
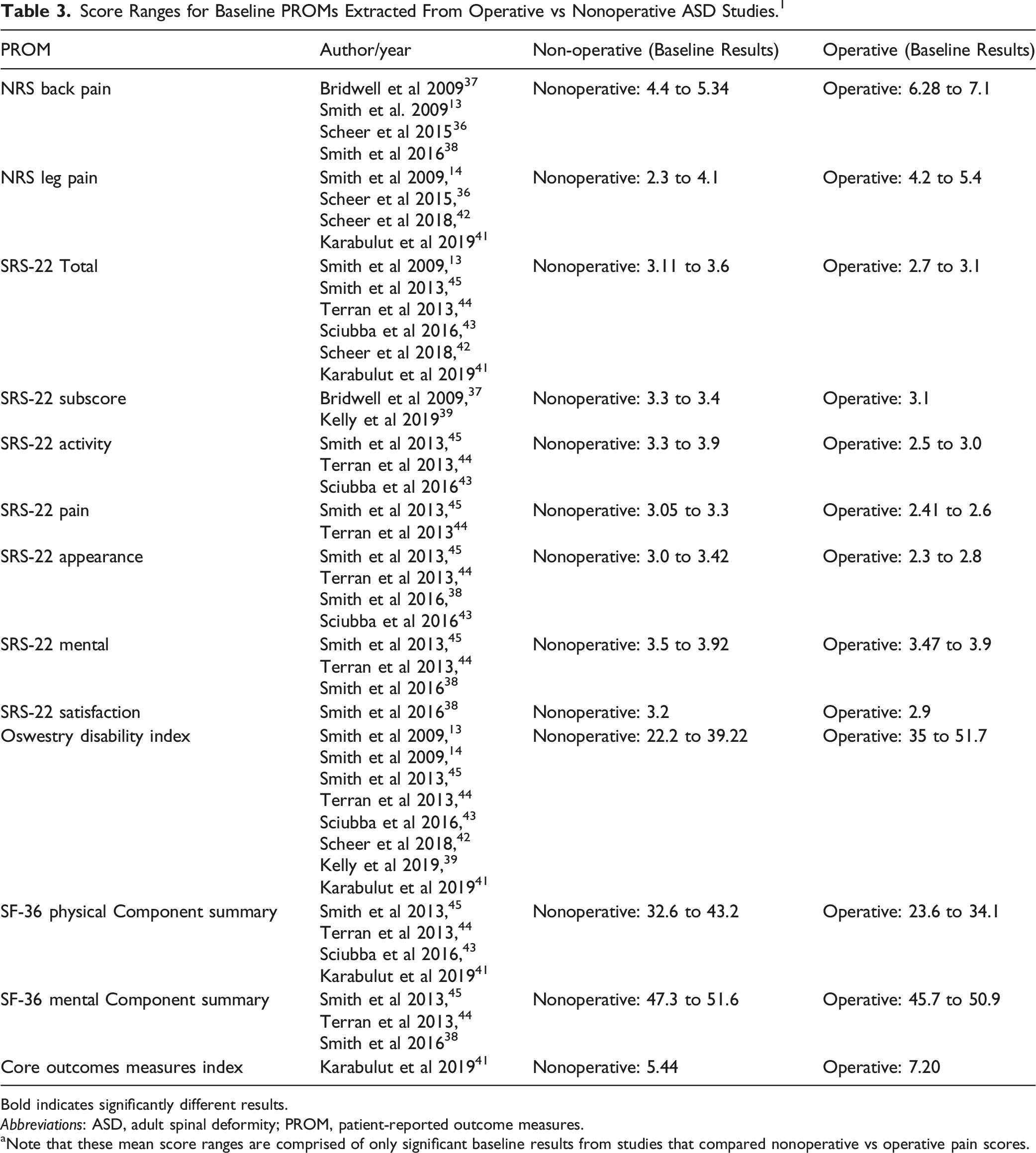
Bold indicates significantly different results.
Abbreviations: ASD, adult spinal deformity; PROM, patient-reported outcome measures.
aNote that these mean score ranges are comprised of only significant baseline results from studies that compared nonoperative vs operative pain scores.
Articles with Dynamic Functional Testing for Operative vs Nonoperative Patients
Articles With Dynamic Functional Testing for Operative vs Nonoperative Patients.
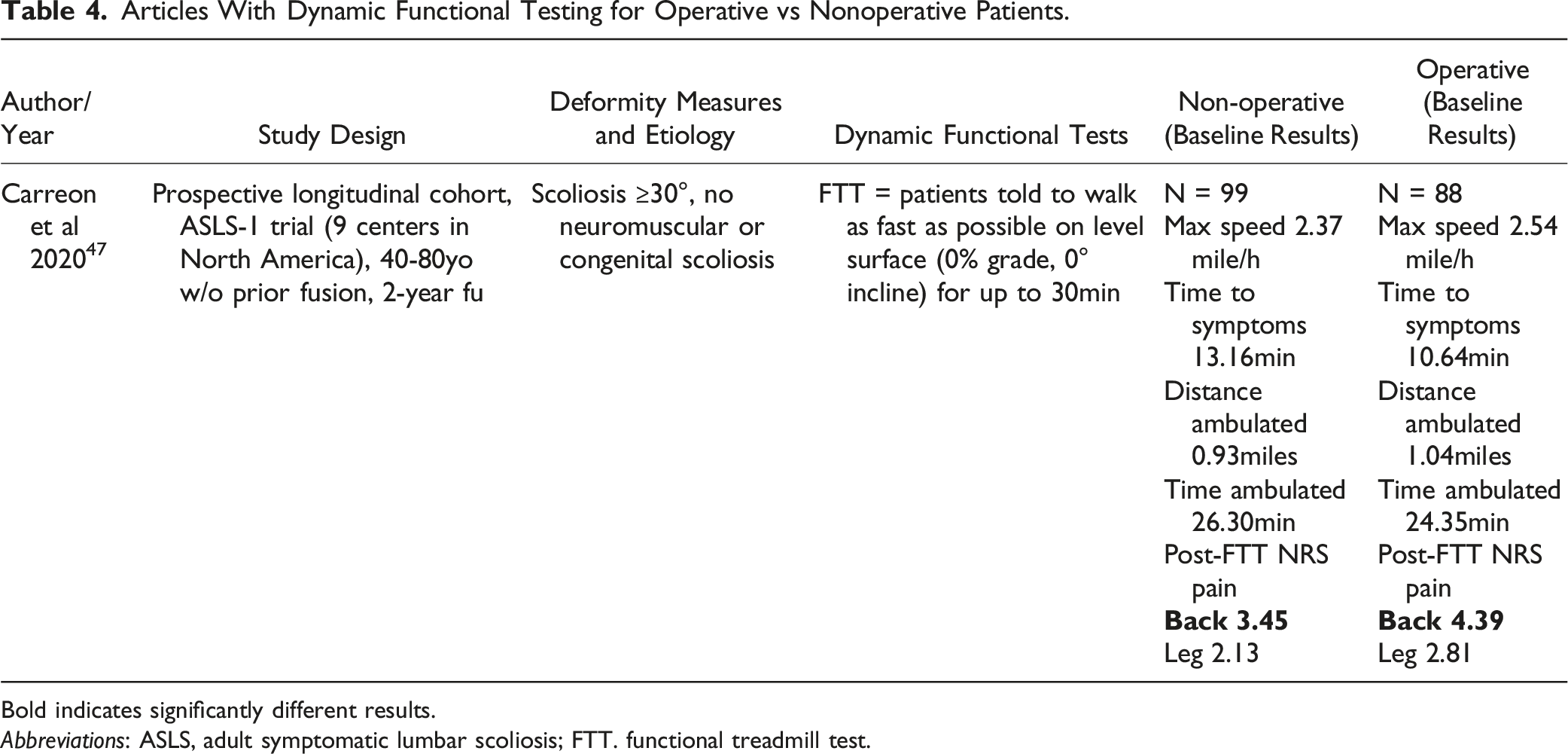
Bold indicates significantly different results.
Abbreviations: ASLS, adult symptomatic lumbar scoliosis; FTT. functional treadmill test.
Articles with Decision-Making Algorithms or Criteria for Operative vs Nonoperative Treatment
Articles With Decision-Making Algorithms or Appropriateness Criteria for Operative vs Nonoperative Treatment of ASD.
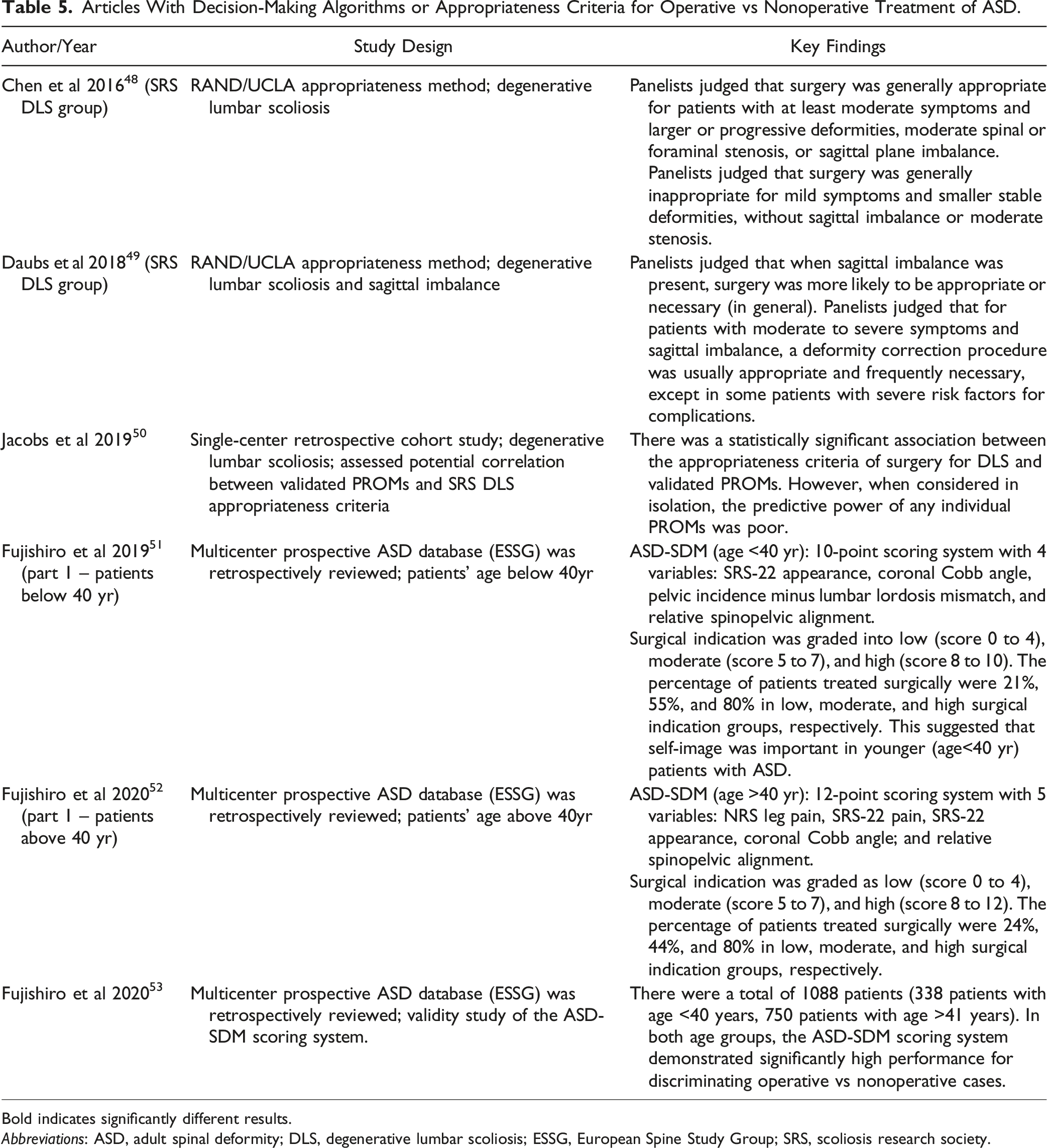
Bold indicates significantly different results.
Abbreviations: ASD, adult spinal deformity; DLS, degenerative lumbar scoliosis; ESSG, European Spine Study Group; SRS, scoliosis research society.
Discussion
Analyzing Baseline Symptoms and PROMs for Surgical Decision-Making
Few ASD studies rigorously investigated the baseline symptoms and PROMs which may influence both the patient and surgeon to proceed with operative treatment. The results of the present literature search produced 9 articles with publication dates spanning 2007 to 2018.8,9,12,15,31-35 Review of these studies demonstrated the relative paucity of literature that focused on symptom assessment and surgical decision-making for ASD. There was no clear consensus regarding operative vs nonoperative treatments and how this decision-making process may be impacted by severity of back/leg complaints, duration of symptoms, and degree of disability.
The first study we found was published in 2007 by Glassman and colleagues. 15 Notably, the authors provided evidence to suggest that leg pain (yes/no) and moderate-to-severe back pain in the past 6 months (or higher mean daily level of back pain) were more likely associated with patients who underwent operative treatment. 15 Then in 2008, Smith et al. also demonstrated that leg pain (severe radiculopathy) was a significant factor associated with operative treatment (on both uni- and multivariable analysis). 12 In addition, Smith et al reported that motor weakness was another significant factor that could potentially influence the decision to undergo operative management (note that the only other article to provide complete neurological assessment with data on motor deficits/weakness was by Neuman et al).12,33
In comparison to these previous studies, Pekmezci et al (2009) suggested that functional status evaluated through HRQL measures was more useful during the surgical decision-making process than assessments of back/leg pain severity. 31 Pekmezci and colleagues acknowledged that back/leg pain contributed to patient morbidity and may motivate afflicted patients to present to a surgical clinic; however, the authors argued that pain alone was not as important as the degree of functional compromise when deciding on operative treatment. 31 An important difference from the prior Glassman et al study 15 was that Pekmezci et al. did not include ODI as a matching covariate when comparing operative vs nonoperative patients. The authors explained that this decision was because they thought that the magnitude of disability assessed with ODI could be an important factor impacting patient decision-making. 31 Note that subsequent studies have demonstrated that ODI, SF-36 PCS, and SRS-22 Total and Sub-domain scores were significantly worse for operative vs nonoperative patients – and, these outcome measures were also worse for patients who crossed over from nonoperative to operative management.8,35
In parallel, Bess et al (2009) reported the importance of subgroup analysis by patient age when analyzing the variables that could impact operative decision-making. 9 The authors suggested that increased coronal plane deformity drove operative treatment in younger patients (<50 years), whereas pain and disability drove operative treatment in older patients regardless of deformity. 9 Their results demonstrated that older patients (≥50 years) who underwent operative treatment reported worse VAS pain and ODI scores. 9 Note that the Bess et al findings of worse disability in operative patients were different from the prior Glassman et al study. 15 Bess et al suggested that the reason for this discrepancy was potentially related to the older patient population compared to the Glassman et al study (mean age 54 vs 44 years, respectively).9,15 Another study by Fu et al (2010), which focused on elderly degenerative scoliosis patients (age >60 years), provided results consistent with Bess et al 9 and demonstrated worse disability and health status in patients undergoing operative treatment. 32 More recent studies (Fu et al [2014], 8 Neuman et al [2016], 33 Fujishiro et al [2018], 34 Passias et al [2018] 35 ) also demonstrated that operative patients reported worse PROMs and/or more severe back/leg pain scores in comparison to nonoperative patients. Notably, Neuman et al was the only study to utilize post-functional treadmill test back/pain scores, which were both significantly worse in operative patients. 33
In summary, there is an ongoing debate regarding optimal ASD surgical decision-making and how this process may be influenced by baseline factors such as severity of back/leg pain, duration of symptoms, and standardized disease-specific and general assessments of disability and health status. Although some studies have emphasized the importance of pain severity (especially presence of leg pain),12,15 other authors reported that pain alone should not be the main factor governing the transition from nonoperative to operative care. 31 Moreover, the importance of these factors may be age-specific, with younger vs older patients choosing operative management for different reasons. 9 Although it seems intuitive that patients presenting with motor deficits would be more likely to undergo operative treatment, only 2 of the previous studies provided complete neurological assessment with motor function.12,33
Collectively, these prior studies8,9,12,15,31-35 likely suggest that a multifactorial process governs the decisions, for both patients and practitioners, to transition from nonoperative to operative management. In this review, we intentionally focused just on symptoms and PROMs (and not radiographic measures, deformity, or comorbidities). The current evidence seems to suggest that the severity of back/leg pain is likely an important factor in surgical decision-making, especially when the pain is severe enough to negatively impact health status. For example, if the patient can no longer perform activities of daily living due to back/leg pain, then operative management could be considered. Also, duration of these symptoms is likely important, but is infrequently reported in the literature. We found an article from Glassman et al which reported that presence of moderate-to-severe back in the past 6 months (prior to study enrollment) may be associated with operative treatment. 15 Also, Smith et al 12 and Passias et al 35 reported mean time intervals of approximately 11 months and 13 months, respectively, for patients who crossed over from non-operative to operative treatment; however, the majority of studies did not include assessment of symptom duration.
Extracting Baseline PROMs from Operative vs Nonoperative Comparative Studies
Previous work by the Scoliosis Research Society (SRS) Degenerative Lumbar Scoliosis (DLS) Appropriateness Group suggested that, in general, self-reported symptoms (e.g., back and/or leg pain) should be at least moderate-to-severe before operative management is considered – especially in cases with progressive deformity, larger curves (>30°), moderate or severe central or foraminal stenosis, or sagittal imbalance.48-50 The first publication from the SRS DLS Appropriateness Group utilized the RAND/University of California at Los Angeles (UCLA) Appropriateness Method to develop the initial recommendations and criteria for assessing appropriateness of surgery. 48 The group found that surgery was generally inappropriate for patients with mild symptoms and smaller stable deformities, without sagittal imbalance or at least moderate stenosis, especially in patients with advanced age and multiple medical comorbidities. 48 A subsequent publication by Daubs et al. and the SRS DLS group further refined the surgical appropriateness criteria for DLS patients with sagittal imbalance. 49
The SRS DLS Appropriateness Group provided an initial framework for assessing appropriateness of surgery, but with regards to patient-reported symptoms, the criteria did not include specific PROMs or threshold criteria using validated pain scales (e.g., Numerical Rating Scale [NRS] or Visual Analog Scale [VAS]). Furthermore, the duration of patient symptomatology was not included in the appropriateness criteria for operative treatment of DLS. 48 As such, we reviewed ASD literature for operative vs nonoperative comparative studies and extracted baseline PROM data from relevant articles.13,14,36-46 We then included the baseline PROMs that were significantly different between operative and nonoperative cohorts, and then tabulated these values to generate optimal score ranges for each treatment modality (see Results section). These score ranges may provide a reference to assist patient counseling and can potentially facilitate future research focused on nonoperative vs operative decision-making. However, interpretation of these scores may be limited due to the broad radiographic definition of ASD and heterogenous study cohorts (e.g., patients with primary sagittal deformity vs scoliosis may report different pain and disability thresholds when deciding on surgery).
Optimal PROM Cutoffs for Surgical Decision-Making
Our PROM reference ranges for operative vs nonoperative treatment were consistent with the cutoff scores provided by other authors (Bridwell et al, 2009, 37 Karabulut et al, 2019, 41 Mannion et al 2020 40 ). Bridwell et al reported that the definition of “symptomatic” corresponded to ODI ≥20 and/or SRS domain scores ≤4.0 in pain, function, or self-image. 37 Next, Karabulut et al calculated the optimal cutoff values to diverge operative and nonoperative groups for elderly patients (age >70 years): ODI = 37.0, SF-36 PCS = 37.5, SRS-22 = 3.2, and COMI = 5.7. 41 More recently in 2020, Mannion et al utilized the concept of a “patient acceptable symptom state (PASS)” in patients with ASD. 40 The authors quantified the score equivalent to PASS for different outcome instruments as follows: ODI ≤18, SRS subscore >3.5, SRS subdomains >3.3-3.8, and NRS pain ≤3. 40
These previously defined PROM cutoffs for operative and nonoperative treatment, as well as the score ranges presented in the present review, could potentially facilitate the surgical decision-making process.37,40,41 In support of this, note that Jacobs et al demonstrated that there was a statistically significant association between validated PROMs and the SRS DLS surgical appropriateness criteria. 50 The same authors concluded that “future studies with larger patient cohorts should further validate the incorporation of PROMs into the appropriateness criteria and optimize thresholds when to opt for surgery or not.” 50 It is likely that multiple PROMs should be taken into consideration when deciding on treatment, and that interpreting a single PROM in isolation from the patient’s clinical presentation (e.g., age, comorbidities, radiographic findings, deformity correction goals) is generally not recommended.
Notably, commentary from Glassman and colleagues suggested that the SRS DLS surgical appropriateness criteria represented a significant step towards evidence-based uniform treatment of ASD, but it would likely require continued research for further validation and refinement. 54 Further research is also needed to overcome limitations due to heterogenous study cohorts and poorly defined outcomes, which represent barriers to developing standardized ASD treatment.
Symptom Duration and Patients Who Crossed Over from Nonoperative to Operative Treatment
Regarding timing of ASD surgery, few studies focused on the duration of symptoms which may warrant operative intervention. More specifically, there was no clear consensus regarding the duration of back and/or leg pain symptoms which should prompt the surgeon and patient to consider surgical management. As such, as part of this narrative review, we also compiled the articles which analyzed patients crossing over from nonoperative to operative treatment, and then analyzed the symptoms which may have impacted this transition. Note that this comprised 6 articles which are included in Tables 1 and 2.12-14,35,37,39 We hypothesized that analyzing these crossover patients may provide novel insight into the duration of back/leg pain associated with the transition from nonoperative to operative treatment.
In 2008, Smith and colleagues published the first article in a series of landmark studies which analyzed the subset of ASD patients crossing over from nonoperative to operative treatment during study follow-up. 12 The authors reported that 23 patients (15%) who had initially been classified in the nonoperative cohort crossed over into the operative cohort at a mean time interval of 11 months after study enrollment. 12 These patients reported significantly higher VAS scores for leg and back pain at enrollment compared with those who did not cross over. 12 Among patients who crossed over, the principal symptom prompting surgery was radicular leg pain in 14 patients, back pain in 5 patients, and equivalent radicular and back pain in 4 patients. 12
Then in 2009, Smith and colleagues published 2 articles focusing on back and leg pain, respectively, and outcomes after operative vs nonoperative treatment.13,14 In the study focused on back pain, the authors reported that 41 patients crossed over from nonoperative to operative management during study follow-up at mean time interval 0.8 years (median 0.7 years, range 0.1-1.9 years). 13 These crossover patients demonstrated a nonsignificant trend toward increased back pain at time of choosing surgery (P = .06). 13 Next, in the article focused on leg pain, Smith and colleagues reported that 14 patients crossed over from nonoperative to operative management at mean time interval 0.9 years (median 0.8 years, range 0.1-1.8 years). 14 For these crossover patients, the mean NRS scores for leg pain remained without significant change from baseline (P = .2). 14
Following the work by Smith and colleagues, subsequent studies have demonstrated that nonoperative to operative crossover patients reported significantly worse disability and health status both at the time of study enrollment (compared to nonoperative patients who did not cross over) and at the time of choosing surgery (in comparison to the crossover patients’ enrollment PROMs).35,39 Collectively, this may suggest that high baseline and increasing disability over time drives the conversion from nonoperative to operative ASD management.35,39 Finally, regarding duration of symptoms and timing of surgery, it seems reasonable to follow patients who initially opt for nonoperative treatment for up to approximately 2 years, since most patients who crossed over in these prior studies did so within this timeframe.12-14,35,37,39
Summary of Recommendations for Timing of ASD Surgery and Symptoms (Magnitude/Duration)
Regarding magnitude of symptoms and timing of surgery, the results of this narrative review suggest that at least moderate symptoms should be present prior to considering operative treatment of ASD. In many cases, patients will present with complaints of back and/or leg pain, which could be radicular and/or claudication-type leg pain. In this review, we found that many of the patients who underwent operative treatment reported moderate-to-severe back pain (mean NRS back pain scores 6-7). When following symptomatic ASD patients who initially opted for nonoperative treatment, worsening back pain (which is significantly and positively correlated with worse disability and health status13,36) may prompt conversion to operative care.
In comparison to back pain, we found that patients with leg pain who underwent operative treatment typically reported leg pain NRS scores that were lower than the averages for back pain (mean NRS leg pain scores 4 to 5). Also, 2 key studies identified presence of leg pain as an independent predictor for patients to undergo operative treatment for ASD (back pain was not identified as an independent predictor of operative treatment).12,15 When following symptomatic ASD patients who initially opted for nonoperative treatment, continued leg pain despite maximum conservative therapies may prompt conversion to operative care, but average NRS leg pain scores may not reflect worsening pain severity. Note that like back pain, leg pain is also significantly associated with worse disability and health status.14,36 As such, symptomatic patients with worsening back and leg pain may also demonstrate worsening scores on other health outcome metrics (ODI, SF-36 PCS, SRS-22), which may influence surgical decision-making.
Less is known about the duration of symptoms and its impact on the timing of surgery for ASD. We suspect that studies focused on assessing back/leg pain duration at the time of enrollment will likely be limited by potential recall bias. Asking ASD patients to report the exact timeframe and duration of their symptoms may lead to inconclusive results. However, after study enrollment, prospectively analyzing patients who cross over from nonoperative to operative treatment may provide novel insights to help address the issue. In this narrative review, we found that the vast majority of patients who initially opted for nonoperative care and then subsequently chose surgery, did so within approximately 2 years of study enrollment. As such, we suggest following symptomatic ASD patients undergoing nonoperative treatment for at least 2 years and assessing these patients for worsening symptoms or disability which may warrant surgical consideration.
Finally, when assessing symptom duration and its impact on surgical decision-making, it may help to understand the pathogenesis of ASD and its potential relationship with the typical chronological order of back/leg pain complaints (i.e., leg pain may appear later than back pain in the pathophysiology of ASD). In 2018, Cawley et al proposed a novel pain assessment (NRS20) comprised of summing both NRS scores for back and leg pain. 55 The authors proposed that the distribution of NRS20 pain scores demonstrated 3 clear patterns of pain for ASD: back pain only, moderate back pain with varying mild-moderate leg pain, and severe equivalent back and leg pain. 55 In their discussion, Cawley and colleagues suggested that patients who develop greater amounts of back pain are more likely to develop leg pain. 55 Also, the authors reported that when back pain reached approximately NRS score of 6, then leg pain tended to become more prevalent and more pronounced before back pain started becoming more severe. 55 Finally, Cawley et al suggested that patients with both severe back and leg pain likely reflected a state of “decompensation” – that is, early disc or facet degeneration could be initially offloaded with lumbar flexion with corresponding muscular fatigue. At this point, foraminal height of the affected segment may be preserved, but as compensatory measures fail (e.g., high pelvic tilt), then foraminal height becomes compromised, loss of sagittal balance ensues, and increasing pain and disability is the end result of this pathological process. 55
Future Directions and the Need for a Multicenter Prospective Study
Recent articles have proposed surgical appropriateness criteria and scoring systems for discriminating operative vs nonoperative cases. Both the SRS DLS Appropriateness Criteria48-50 and the ASD-SDM scoring system51-53 proposed by Fujishiro et al and the ESSG represented significant progress towards providing an evidence-based framework and algorithm to facilitate the surgical decision-making process. In commentary on the Surgical Appropriateness Criteria from Glassman and colleagues, 54 the authors acknowledged that this marked an important collaboration between spine societies and industry partners to support evidence development – and, although subsequent studies may validate and refine the initial recommendations, the most important result was that the standard for evidence-based treatment was raised. 54
Next, further investigation is needed to define the appropriate values for meaningful or important clinical differences in validated PROMs when assessing operative vs nonoperative patients at baseline. Note that prior studies have defined the values for minimal clinically important difference (MCID) or substantial clinical benefit (SCB) to provide clinical context when assessing HRQL outcome measures.56-59 However, these studies defined MCID and SCB for comparing treatment outcomes, and were not designed to detect clinically meaningful score differences in patients at baseline prior to treatment. If future prospective studies are designed to evaluate the differences in PROMs which may impact timing of surgery and the decision-making process, then it will likely be beneficial to have appropriate MCID values when comparing symptomatic patients prior to undergoing treatment.
This narrative review identified leg pain as an independent predictor of operative management for symptomatic ASD patients presenting to surgical clinic. 12 To our knowledge, Smith et al was one of the few investigators to differentiate radiculopathy vs claudication-type leg pain. 12 Future prospective studies may benefit from more rigorous assessment of leg pain, including data such as type of leg pain (radiculopathy vs claudication), which may help elucidate the different pain generators associated with the pathophysiology of ASD (i.e., foraminal stenosis, central canal stenosis, neural compression at the curve concavity, neural traction at the curve convexity). Furthermore, novel scoring assessments for pain may also be important when designing a prospective multicenter study aimed to help determine timing of ASD surgery. For example, Cawley et al proposed the novel NRS20 pain score, and demonstrated that this method had improved correlation to HRQL in comparison to individual NRS scores for back or leg pain. 55
Next, including dynamic functional testing in a new trial design would likely provide additional information to facilitate surgical decision-making. Currently, few ASD studies provide data to characterize back and leg pain after treadmill walk tests. 47 Prospective studies that analyze the development of back/leg pain after treadmill walking, including the severity of the pain, timing of pain onset, and maximum walking distance, could potentially help improve surgical decision-making. Finally, post hoc analysis of patients who crossed over from nonoperative to operative treatment has provided novel insights into the duration of symptoms which might prompt surgery. However, it may be helpful to prospectively follow larger multicenter cohorts of known symptomatic ASD patients to further validate these prior studies, which were often limited by smaller cohort size for the subset of patients who crossed over during follow-up.12-14,35,37,39 Asking patients to recall the duration of back/leg pain at the time of study enrollment may be prone to recall bias; therefore, post hoc analyses with large multicenter cohorts may be the most prudent step towards addressing the issue.
Conclusions
This narrative review identified articles which could help address the topic of timing of surgery for patients with adult spinal deformity. The present review focused on patient symptoms (both magnitude/severity and duration) which could impact the transition from nonoperative to operative treatment. In summary, back/leg pain should likely be at least moderate prior to consideration of surgery. For many studies comparing operative vs nonoperative treatment, back pain was typically reported as being more severe than leg pain. Some studies identified leg pain (and not back pain) as an independent predictor of surgery, which may suggest that the emergence of leg pain represents more severe spinal degeneration or decompensated deformity. Back and leg pain were consistently identified as being positively correlated with disability and worse functional health status, which are also significant drivers of surgery. These results may provide a reference or framework for designing a future prospective multicenter trial. Potential topics that need further investigation include defining meaningful or clinically important differences in validated outcome instruments to assess patients at baseline, more detailed assessments of leg pain (radiculopathy vs claudication), including dynamic functional testing when reporting baseline symptoms, and further analysis of symptom duration and/or progression. Both the Scoliosis Research Society Degenerative Lumbar Scoliosis Appropriateness Criteria and the Adult Spinal Deformity Surgical Decision-Making scoring system represent initial progress towards raising the quality of current evidence and provide algorithmic frameworks to facilitate operative timing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Deformity, a focused group of international Adult Spinal Deformity experts. AO Spine is a clinical division of the AO Foundation, which is an independent medically-guided not-for-profit organization. Support was provided directly through AO Network Clinical Research.