
Abstract
Background: Inclusion Body Myositis (IBM) is an inflammatory myopathy that commonly affects quadriceps strength, resulting in knee buckling and falls. Therefore, patients with IBM should be ideal candidates for stance control orthoses (SCOs).
Objectives: Evaluate the effectiveness of SCO use in patients with IBM who have functional deficits due to quadriceps weakness.
Study Design: Cohort study.
Methods: Nine subjects with IBM were provided a stance control orthosis and followed for six months of home use. All patients had objective testing of their strength and gait and completed a questionnaire at baseline and six months. Gait analysis was performed both with and without the orthosis.
Results: Velocity and cadence were lower and step width was higher when using the orthosis. Kinematic measures were largely unchanged with orthosis use. Subjects with less knee extensor weakness had a better outcome than weaker participants. Those who spent more time wearing the orthosis also had a more positive outcome. The participants felt that the SCO was helpful in safeguarding against falls and providing stability.
Conclusions: SCO use will benefit patients with IBM, but care should be taken to choose the SCO option that best suits their individual clinical presentation.
This is the first study to examine SCO use in the IBM population. Patients with IBM have quadriceps weakness and will potentially benefit from SCO use. This study suggests that successful SCO management of patients with IBM depends on severity of weakness.
Introduction
Affecting 10 people per million, inclusion body myositis (IBM) has a distinctive pattern of weakness. 1,2 Although IBM affects both proximal and distal muscles of the extremities, the disease almost universally involves the finger flexors, quadriceps, ankle dorsiflexors and swallowing muscles. Ventral muscle groups are more affected than dorsal and girdle muscles, which can help preserve postural stability and locomotion. Most IBM patients present with an initial complaint of weakness, predominantly in the proximal lower limbs. Strength usually decreases 5 to 10% per year, although progression rates can vary. 3 – 5 Most patients remain ambulatory for many years after diagnosis. However, because the quadriceps are among the most affected muscles, patients often complain of falls or buckling of the knees. Up to 75% of IBM patients use an assistive device such as a cane as the disease progresses, with some moving to a wheelchair because of a fear of falling. 3 Three-quarters of patients with IBM report frequent falls. Frequency of falls declines for a time after initial diagnosis before increasing again as the disease progresses. 3
Because of the unique weakness pattern and prominence of quadriceps, patients with IBM would, in theory, be ideal candidates for a stance control knee orthosis (SCO). SCOs work by providing a stable knee during the stance phase of gait but releasing to allow free knee flexion during swing. SCOs have been shown to be more energy efficient and provide a more natural looking gait with fewer compensatory motions than a locked knee orthosis. 6 – 15 These features would provide support against knee buckling in patients with IBM with minimal adverse affects. Currently, there is no published report of SCO use in patients with IBM. Therefore, the purpose of this study was to apply SCO technology to a group of patients with IBM. We hypothesized that there would be positive kinematic and temporal distance changes in IBM patients when using the SCO, and that patients with weaker quadriceps would show greater benefit from SCO use. We also hypothesized that patients with IBM would have positive subjective opinions of an SCO.
Methods
Nine subjects (7 male, 2 female, average age 61 ± 9, average BMI 27.2 ± 4.0) with IBM gave informed consent and were enrolled into the study after approval by the Mayo Clinic IRB. Time since onset of symptoms was 6.4 ± 4.3 years. Four of the nine subjects reported using a cane at times, and all subjects complained of knee buckling and falls. None had used an SCO in the past. Subjects were fitted with a SensorWalk (Otto Bock Health Care, Minneapolis, MN) SCO by a certified orthotist. The braced side was determined by the participants’ subjective evaluation of the weaker leg. All subjects were braced unilaterally and had sufficient hip strength to advance the braced limb. Subjects were allowed a six-month period to use the SCO before returning for laboratory measurements. The six-month period was chosen because previous work 8 demonstrated that gait changes in brace users may require a six-month timeframe. Return measurements were done both with and without the SCO.
Gait was assessed using a 10-camera motion analysis system (Motion Analysis Corporation, Santa Rosa, CA) and four force platforms (2 AMTI model BP400600, Advance Mechanical Technology, Inc., Watertown, MA and 2 Kistler model 9281B, Kistler Instrument Corp., Amherst, NY). All subjects walked without aids for the gait analysis. Marker trajectory and force platform data were used as inputs to Visual3D (C-Motion, Germantown, MD) to calculate kinematics and kinetics. Three left and right force plate strikes were included for analysis. Trials were averaged and strides normalized to 100% gait cycle, with 0% being foot-strike and 100% indicating ipsilateral foot-strike. An SCO questionnaire covering donning and doffing, brace cosmesis and weight, as well as stability during standing, walking and postural transitions was administered. 16 Because a strength decline during the trial could affect the success of brace use, the strength of hip flexors, hip extensors, hip abductors, knee flexors, knee extensors, ankle plantarflexors and ankle dorsiflexors on the braced limb were measured at baseline and follow-up using a QMA testing system (Aeverl Medical, LLC, Gainesville, GA). Values were recorded as % body weight × or times height and unitless (torque (Nm) normalized to subject height (m) and weight (N)). The data were tested for normal distribution using an Anderson-Darling test. If normally distributed, comparisons were made between the braced and unbraced conditions using a paired t-test, and between the two strength groups using a two-sample two-sided t-test. When not normally distributed, comparisons were made with the Wilcoxon Signed-Rank test for paired data. Statistical significance was set at p = 0.05.
Results
Six of nine subjects returned for testing after the six month trial. Three did not return for various reasons: one had moved and was lost to follow up; one had suffered a heart attack and was unable to return; one had a decline in ambulatory function due to a fall while not wearing the brace and did not wish to travel. Because of the three dropouts, an on-treatment analysis was performed. Of the six who completed the study, there were four males and two females with an average age of 60 ± 9, average BMI of 26.6 ± 4.5, and time since symptom onset of 4.4 ± 2.6 years. Use of the brace over the trial period varied, ranging from a couple of hours per day to all day, every day.
Objective gait analysis and strength characteristics
There was a range of abilities within the subject group as evidenced by strength variability. There were two apparent baseline knee extensor strength groups when comparing to age- and gender-matched normals. 17 Subjects 1 through 4 ranged from 30 to 40% of normal, while subjects 5 and 6 were <15% of normal knee extensor strength. Although IBM is a disease of progressive weakness, there was no statistically significant strength decrease in any of the muscles tested. Thus, any gait differences between the braced and unbraced walking conditions at the six-month visit were due to the brace, not a decline in functional status that would necessitate adjustment to the device.
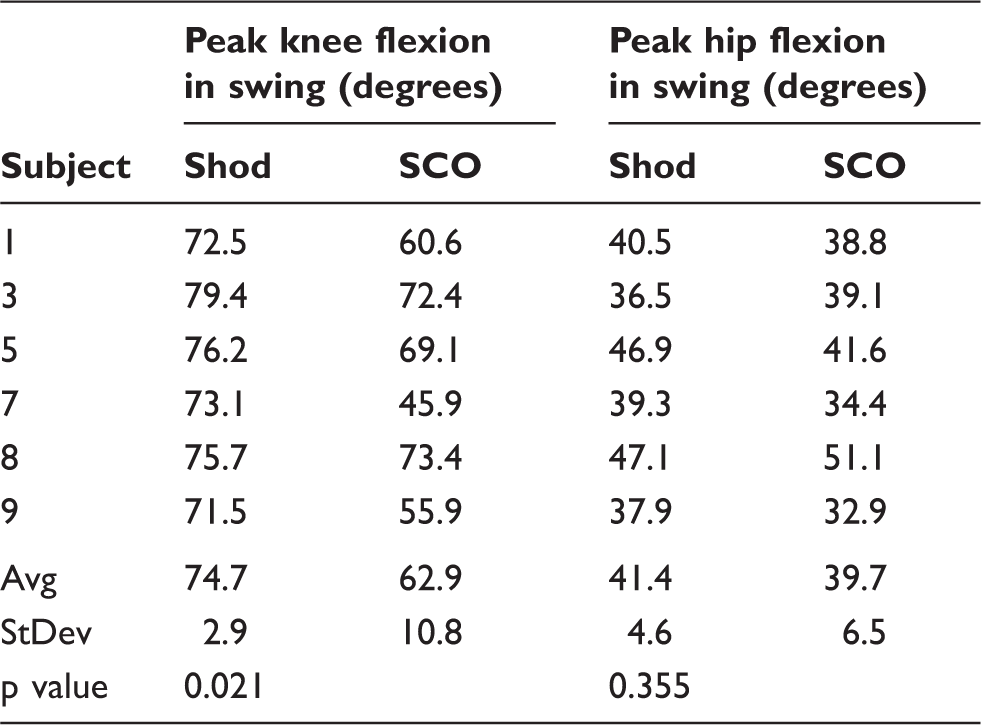
For the group, differences between the braced and unbraced conditions were most pronounced in the temporal distance factors (Figure 1). Subjects walked slower (p = 0.025) and with a lower cadence (p = 0.007) with the SCO, and with a lower velocity and cadence than laboratory norms. Stride length with the SCO was shorter although not significantly different. Subjects adopted a wider step width with the brace (p = 0.035). Subjects also had a shorter and wider stride than laboratory norms. There were no statistically significant differences between the subjects with less weakness (subjects 1 through 4) and the weaker subjects (subjects 5 and 6) while walking shod. However, when wearing the SCO, the weaker subjects walked slower (p = 0.022), had a lower cadence (p = 0.019) and a shorter stride length (p = 0.048) when compared to the subjects with less weakness. There were few differences in kinematics. Peak knee flexion during swing decreased when using the SCO (p = 0.021), however, this value would still be considered normal (Table 1). There was no difference in peak hip flexion during swing. Overall, gait changes were greatest in the weaker subjects.
Temporal distance parameters for shod and SCO conditions at the 6-month follow-up. Peak knee and hip flexion during swing for unbraced and SCO conditions at the 6 month follow up.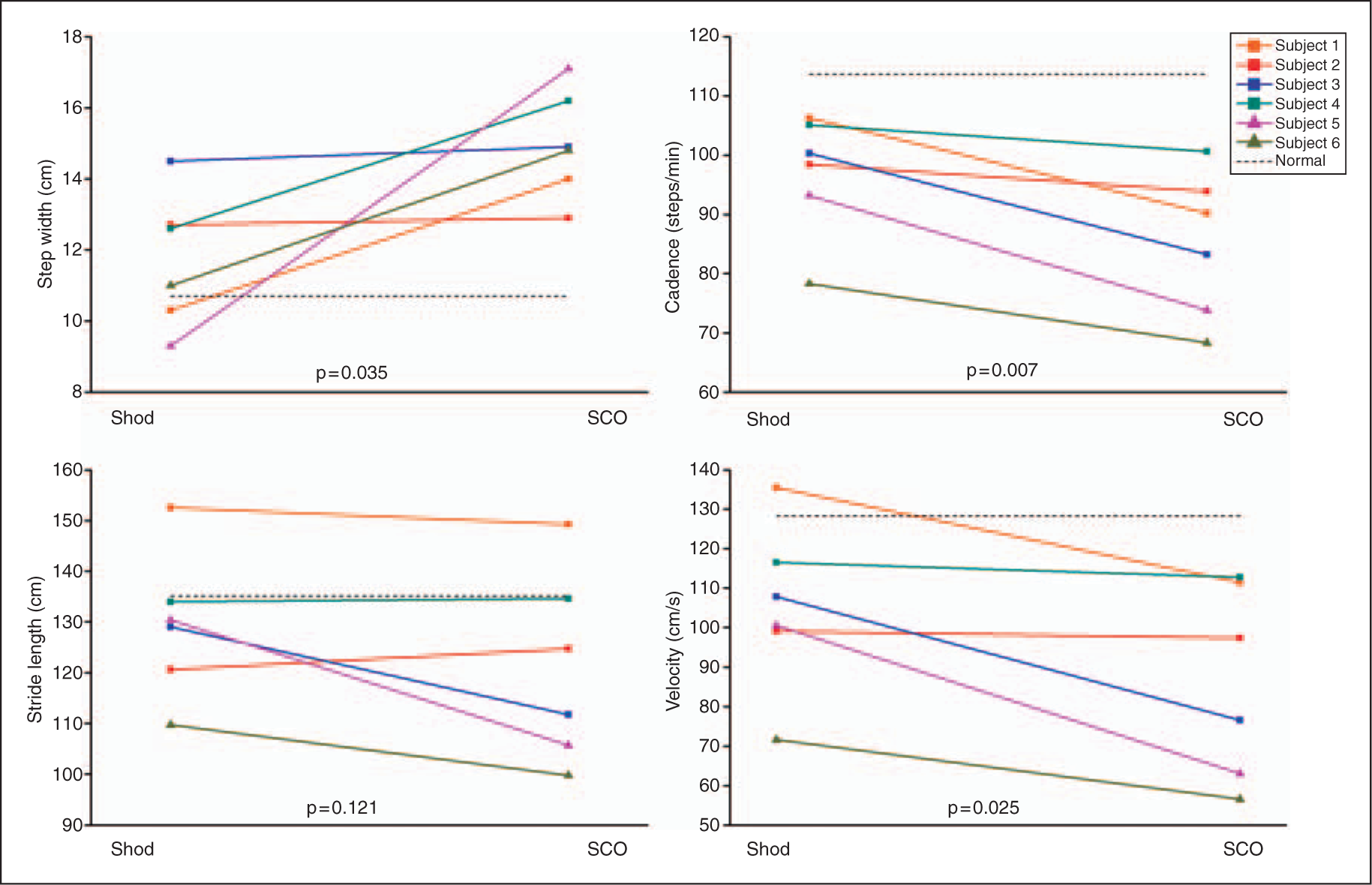
Subjective patient reported changes
Subjectively, the participants felt the SCO was helpful in safeguarding against falls and providing stability. However, all participants had complaints about the size, bulk, cosmesis and noise of the SCO, as well as difficulty donning and doffing the brace, since IBM can also affect finger flexors. Most participants noted they would prefer a less intrusive assistive device.
Users’ experiences differed by their amount of weakness. The subjects with less weakness tended to have positive feedback regarding the SCO. Subject 1 had the strongest knee extensors of the group and reported fewer falls while wearing the device, and generally liked the brace and wore it often. Subject 2 had the second best knee extensor strength and felt the brace was helpful, wore it often, and reported fewer falls. The participants in the middle of the group for knee extensor strength had more mixed opinions. Subject 4 noted fewer falls while wearing the device, wore it daily, and had very positive feedback. Subject 3 felt the brace made her less stable and lopsided because of the weight.
The weakest participants also had mixed feelings regarding the device, with their initial opinions resulting in less use of the brace. Subject 5, the second weakest, liked the added stability of the SCO but was unsure if it reduced his number of falls. He felt lopsided because of the added weight and did not wear it very often. Subject 6 had the weakest knee extensors and did not care for the device nor report fewer falls with the brace on, although she also felt she was simply more careful while walking and did not fall during the trial because of this. In fact, this subject felt less stable with the brace because it was heavy for her small frame, and did not wear it often.
Discussion and Conclusion
This is the first known study to apply an SCO to patients with IBM. The participants in this study exhibited a range of abilities and a range of outcomes. Past SCO studies have shown better gait mechanics, fewer falls, fewer compensatory movements and less energy expenditure with an SCO versus a locked knee orthosis. 6 – 15 Because of the unique weakness pattern and quadriceps weakness in IBM patients, knee buckling and falls being common complaints in this population, an SCO may be especially helpful. The effects might be especially positive in this group as most IBM patients are new to orthotics and novice users can quickly adapt without needing to unlearn compensatory motions needed for a locked KAFO. 8
Grouped data shows that the SCO may not be helpful because of slower velocity, slower cadence, shorter and wider steps, more stance time asymmetry and less knee flexion in swing with the SCO than without. Subjects with less weakness had a more positive outcome than weaker participants. This may be because IBM patients with less weakness also have a more normal gait pattern. 18 Furthermore, individual data provides greater insight into the effects of orthotic applications in this population. One subject with less weakness of the knee extensors did not show much difference in gait, while another with similar strength showed more pronounced differences between conditions. Both of these subjects subjectively thought the brace was helpful, so perhaps objective differences were due to the amount of time spent wearing the brace. One of the subjects with less weakness showed a greater step length with the brace, indicating greater confidence and less fear of falling. Subjects with mid-range strength also showed mixed results, again with increased usage linked to better results or smaller differences between walking conditions. The weakest subjects had the biggest differences in temporal distance factors between braced and unbraced conditions, but both wore the brace very little, perhaps indicating insufficient time spent using the brace to show a positive effect. Differences between conditions for the weakest two subjects were statistically different from the subjects with less weakness, indicating that stronger subjects had a more positive result from the SCO, regardless of the amount of time spent using it.
All subjects showed less knee flexion during swing when using the SCO; however, as knee flexion was still within normal limits this may not be a detrimental finding. IBM is known to affect the ankle musculature. Weak dorsiflexors can force more flexion at the knee and hip to ensure adequate toe clearance during swing. Because the SCO also supported the foot and ankle, decreased knee flexion during swing may simply show that subjects were relying on the ankle support from the brace for toe clearance. Since none of the subjects complained of foot clearance issues, the reduced swing phase knee flexion had no clinical effect. Further, less knee flexion is needed for foot clearance when walking with a lower velocity, as all subjects did with the SCO compared to without.
Although objective gait data were mixed, subjective survey results were positive and similar to previous studies. 16 Subjects reported fewer falls and an increased feeling of stability while walking. All patients complained of the weight and size of the SCO. There are many SCO options currently available, and the device used in this study, the SensorWalk, is the largest and heaviest of the designs on the market. This has been touted as an advantage because of the ability to handle larger patient weight and abnormal frontal and sagittal plane knee alignment, but these features may not be necessary for this population. Further, all participants had sufficient hip strength to advance the braced limb. Stride length did decrease with the SCO as compared to without, but not significantly. All subjects were able to advance the limb even with the additional weight. Because of the positive feelings of stability and fewer falls with this particular SCO, choosing a different device may cause IBM patients to use the brace more and yield more positive objective measures.
The SCO devices currently on the market have a range of inclusion criteria and features such as minimum strength and knee position at foot-strike. For example, the SensorWalk can release at toe off even with a load across the knee joint. This has been shown to be an advantage
8
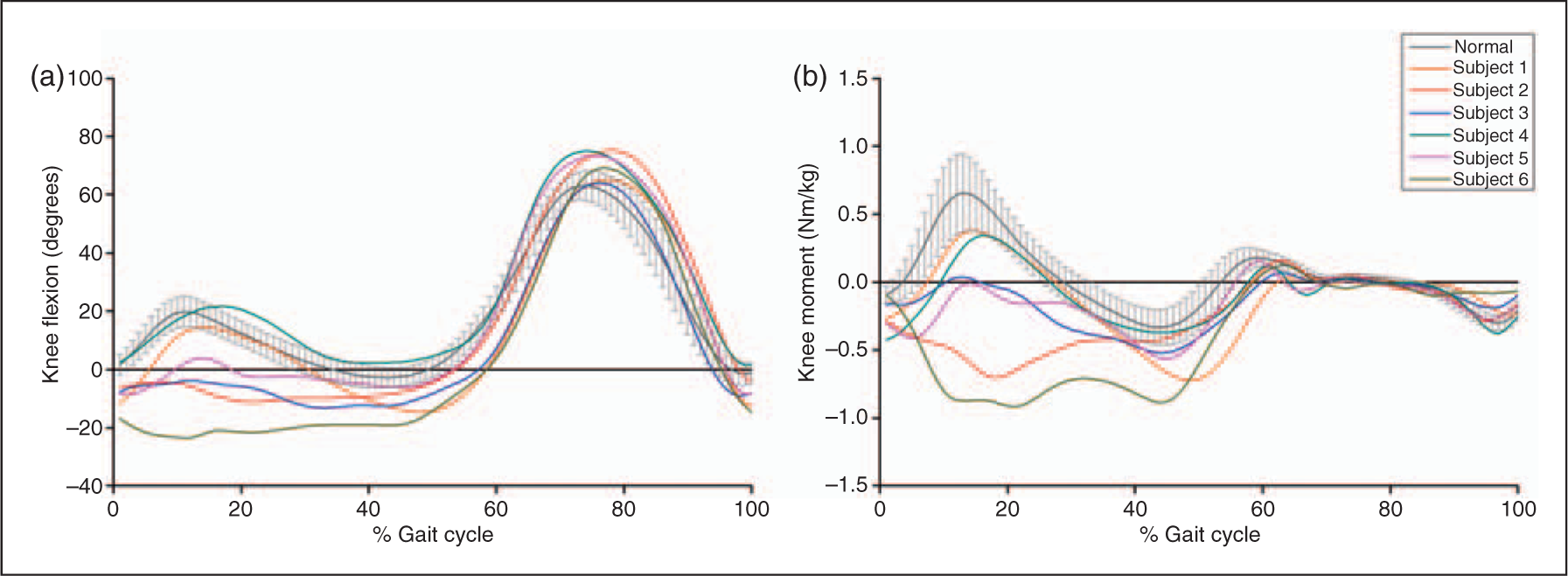
compared to other SCO designs that require the joint to be unloaded before the orthosis will release. In SCO designs that require an external knee extension moment to release, the unloading motion can be unnatural and difficult to learn, especially for patients with a knee flexion contracture or very poor knee extensor strength. Many patients in this study had adequate knee extension in stance and the ability to unload the brace before swing, as shown by the internal flexion moment while shod (Figure 2). Hence, the ability to release under load may be unnecessary. If so, patients may consider other devices. This population provides a prime example of the importance of choosing the appropriate device for your patient, looking at their unique clinical presentation and physical abilities, as well as the operation method and indications for a particular device.
This study revealed a range of success with a particular SCO device. While this group may not have had total success with this SCO, there was enough positive subjective feedback to warrant trying a different device with those patients who did not have the best outcome. This data shows that the amount of time spent using the device has a direct impact on the success a subject experiences. The magnitude of knee extensor weakness was not the sole determinant of success.
Although this is the first study to investigate SCO use in a patient group with a single disease, it has several limitations. First, the sample was small and three of the nine subjects did not return for final testing. Had these additional subjects returned, grouped results may have been slightly different. However, individual results proved to be more informative for those who returned, and this is likely to have held true for any additional subjects. Although IBM is thought to be underdiagnosed, 1,19 it remains a rare disease. This led to recruiting from a large geographic area for a small sample size. Travel for testing was difficult for some subjects. While all participants in this study complained of weakness and knee instability, a range in strength capabilities existed, indicating different stages in the disease process. While this accurately reflects the range of IBM patients who may be interested in a brace for ambulation, it made drawing global conclusions more difficult. When examining only grouped data, the SCO seemed to have a negative impact. However, there was variability among the participants and some subjects had positive objective and subjective outcomes, so it is important to look at each individual’s results. Second, only one SCO design was tested. SCOs are a relatively new technology in orthotics and prescription guidelines are still evolving. Applying a different SCO may yield different results. An individual patient’s benefit will be based on the strength profile, body habitus, functional demand and specific brace fitting criteria. Future work should be aimed at developing patient-specific brace prescription guidelines. By tailoring SCO prescription to fit the individual, greater benefits to the group as a whole may be achieved. In conclusion, this study has shown that SCO use in the IBM patient population has potential benefit for individuals who have knee extensor strength greater than 30–40% of normal.
Footnotes
Funding
We are grateful to the Myositis Association for funding this research study and Ross Terman of Prosthetic Laboratories of Rochester, MN for orthotic fitting.
Conflict of interest
Kenton Kaufman is an inventor of the technology used in this research and holds two US patents on the device.