
Abstract
Stance control knee orthoses (SCOs) have become very popular recently. However, there is little information regarding opinions of actual orthosis users. The purpose of this study was to quantify the users' opinions of a SCO, and see whether factors found important for knee orthoses in past studies hold true for a stance control orthosis as well. A standardized survey was employed as part of a larger field trial study of the Dynamic Knee Brace System, a SCO developed by the authors. The Dynamic Knee Brace System scored well in areas of effectiveness, operability, and dependability, but areas in need of improvement included weight, cosmesis, and donning and doffing. These findings match well with previous knee orthosis studies. This study shows that wearing a stance control knee orthosis can be a positive experience for an orthosis user.
Introduction
Knee-ankle-foot orthoses (KAFOs) historically have had a high rejection rate. Authors have stated that between 58 and 79% of KAFO users stop using their orthosis (Phillips and Zhao 1993; Kaplan et al. 1996) and that over 40% of users state they are ‘dissatisfied’ with their orthosis (Fisher and McLellan 1989). Reasons for rejection or dissatisfaction generally include brace weight and material volume, cosmesis, fit or comfort, or difficulty in donning and doffing the orthosis (Batavia and Hammer 1990). Interestingly, many people who continue to use their KAFOs also have similar complaints about the orthosis (Fisher and McLellan 1989). The frequency of use statistics mirror satisfaction levels with the device. Many users develop opinions on the device during the first 2 weeks, and up to half of braces will be rejected during this same period (Fisher and McLellan 1989; Butler et al. 1983).
Predictors of assistive technology abandonment were formulated by Phillips and Zhao (1993). In a survey of 227 adults with a physical disability, they found that device performance was strongly associated with device abandonment. If a device met a user's expectations for effectiveness, reliability, durability, comfort, safety, and ease of use, the user was more likely to keep the device. Factors such as convenience, energy demand, and the need for assistance were not related to device abandonment.
Batavia and Hammer (1990) investigated the factors consumers consider in determining the value of a given assistive device. A panel of six consumer experts with mobility impairments ranked 15 factors related to assistive devices in general. The three most important factors were effectiveness, operability, and dependability. Effectiveness was defined as the device doing what was claimed or enhancing functional capabilities. Operability meant the device was easy to operate and responded adequately to commands. Dependability was a measure of the device operating with reasonable accuracy under all conditions. Factors covering the aesthetics of the device and the need for special training were not ranked as highly, ending up in the bottom half of ranked factors.
The field of knee orthoses had gone without a significant technological advance since braces changed from metal and leather fabrication to thermoplastics in the 1970s. Recently, however, interest in knee orthoses has been renewed by the advent of stance control orthoses. A stance control orthosis (SCO) keeps the leg locked and rigid during the stance portion of the gait cycle, but lets the limb flex and extend freely during swing. This is generally considered an improvement over the conventional locked KAFO because it provides for a more energy-efficient gait pattern by allowing knee flexion during swing. Several studies have documented that walking with an SCO is a more energy-efficient way to ambulate than with a stiff leg (Kaufman et al. 1996; McMillan et al. 2004; Mattsson and Brostrom 1990). This is because the orthosis user does not have to compensate biomechanically for the functionally lengthened leg that results from keeping the knee locked during swing.
Since 2002, four orthopedic appliance companies have introduced five versions of a stance control knee orthosis (Otto Bock Health Care 2004; Becker Orthopedic 2002 Basko Healthcare 2004; Horton Technology Inc. 2004). All five orthoses try to accomplish the goal of stability during stance yet obtain free knee motion during swing, but use different mechanisms to achieve this goal. Despite the excitement in the orthotics industry over these new knee joints and the claimed benefits to those who rely on a knee orthosis, little evidence exists regarding the biomechanical benefits or opinions of actual KAFO users. Therefore, the primary goal of this study was to subjectively quantify the user's opinions of a stance control orthosis. Further, this study assessed whether the factors found important by the studies of Batavia and Hammer (1990) and Phillips and Zhao (1993) apply to SCOs as well.
Methods
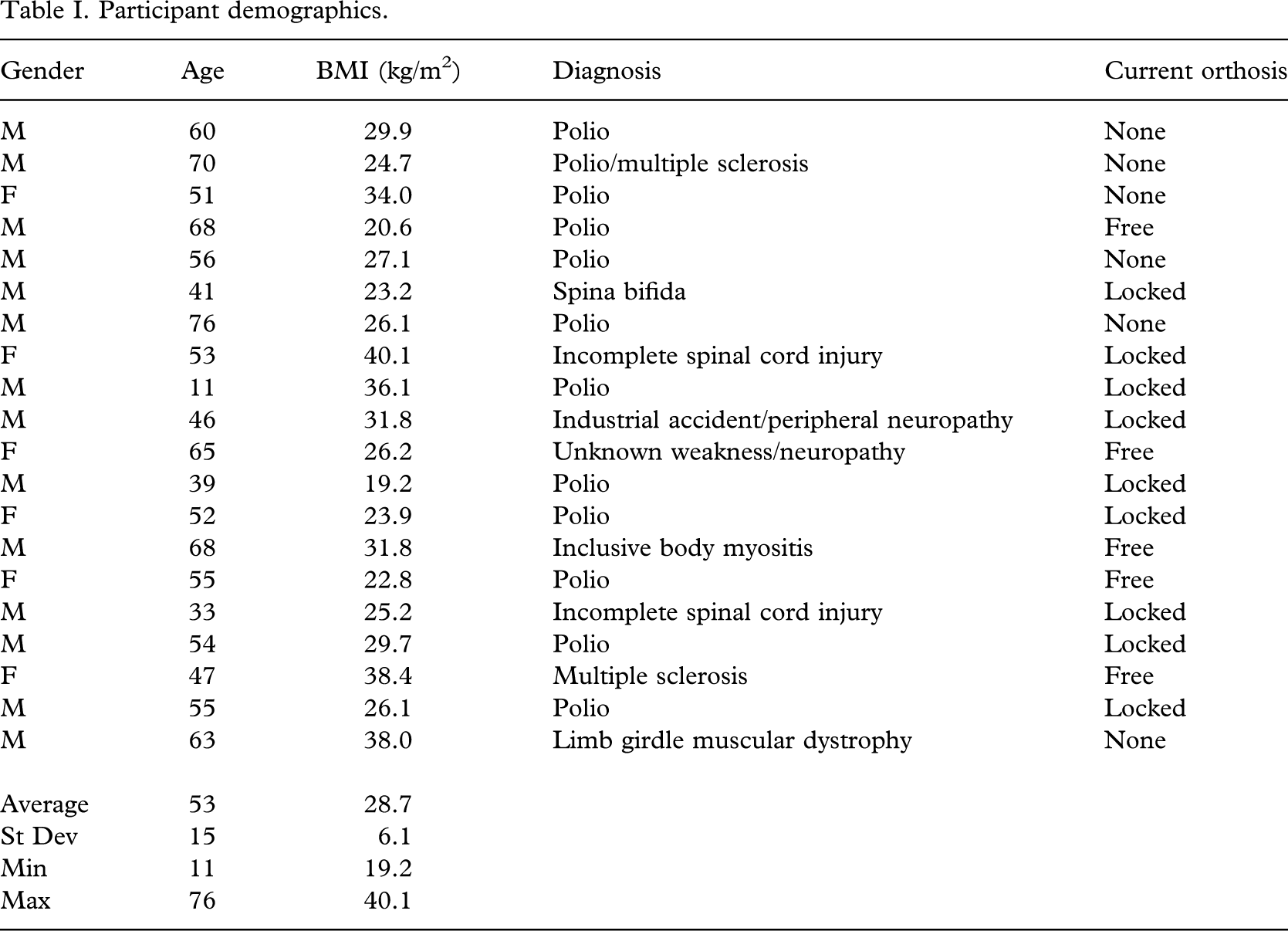
Twenty subjects (Table I) were enrolled into the protocol after giving informed consent according to the institution's guidelines. Fourteen were male, six were female. The age of the research participants was 53.2 ± 14.8 (range 11 – 76) years, with a BMI of 28.7 ± 6.1 (range 19.2 – 40.1, weighed with orthosis on). The majority of the participants were affected by polio (12/20), but diagnoses also included incomplete spinal cord injury, multiple sclerosis, industrial or other injury, spina bifida, muscular dystrophy, inclusive body myositis, and weakness of unknown origin. Fourteen out of the 20 participants were currently using a knee orthosis, while the remainder were not wearing an orthosis on the affected side. Nine of these current orthosis users wore a locked KAFO, and the remaining five used a free motion knee orthosis of some type.
Participant demographics.
The SCO used in this study was the Dynamic Knee Brace System (DKBS) developed by the investigators, as described in detail elsewhere (Kaufman et al. 1996; Irby et al. 1999a, 1999b). In short, the device is a small, relatively lightweight, electronically controlled knee joint that can be installed on a conventional KAFO shell, customized for each user. The mechanical hardware consists of a wrap spring clutch and a clutch release actuator. The electronic control system uses a programmable integrated circuit to monitor control inputs and produce output commands for clutch release. Power for the unit is provided by a battery pack carried in a pouch worn around the waist (Figure 1).
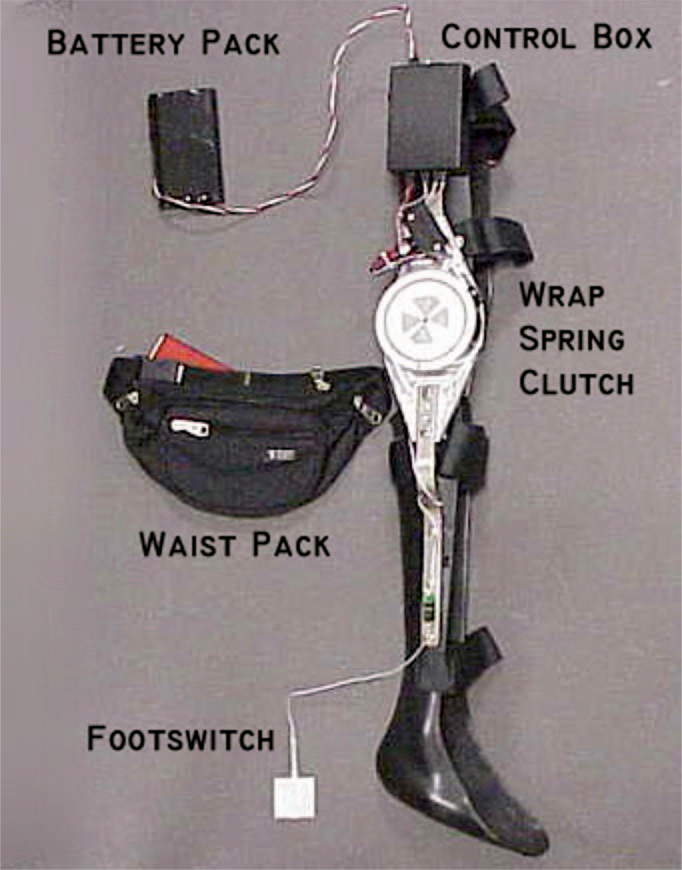
Example of the Dynamic Knee Brace System, the investigational stance control orthosis used in this study. The Dynamic Knee Brace System is comprised of a custom designed wrap spring clutch, an electromechanical release, a control box, and sensors at the knee (not shown), all fit to a conventional KAFO. A rechargeable lithium-ion battery pack is typically carried using a waist pack.
This study was a component of an overall project design including a 6-month at home field trial of the DKBS, with laboratory testing at times 0, 3, and 6 months. During the 6 months of home use, the investigators as well as a licensed orthotist were available to answer questions and make any necessary fit adjustments to the orthosis. Frequency and duration of DKBS use was not directed by the investigators. Participants were free to choose between the DKBS and their personal orthosis during the trial. Therefore, use varied widely among participants depending on comfort with various ground and environmental conditions and the participant's desire to not limit their activities of daily living. Laboratory tests included instrumented gait analysis, physical examination including bilateral lower limb strength and range of motion, and a functional 6-min walk test. Besides these objective measures, a standardized KAFO user survey was conducted while the participant was in the laboratory for testing for 0 and 3-month testing.
The subjective survey (Appendix A) was administered by the same investigator (KB) at the end of the first two laboratory data collections. The survey concentrated on orthosis activities such as donning and doffing the orthosis, assuming a sitting or standing position, use of assistive devices, orthosis aesthetics, stability during walking and standing, walking ability over distance and various terrain, and self-reported daily use of the orthosis. When applicable, these activities using the DKBS were compared to the participant's own brace. If a participant was currently wearing an orthosis of any kind or had worn a brace in the past, they were invited to compare the DKBS to those orthoses. The interview session was videotaped and later scored in order to perform descriptive statistics (SAS Institute Inc., Cary, NC, USA: Version 8.2). Only the questions where all participants used a consistent scoring range were analysed. The numbers of responses to questions vary because not every participant chose one of the options or gave a single answer to each question. Furthermore, not all participants had completed the 3-month testing at the time of analysis. A one-sample student's t-test was used if responses were normally distributed as determined using a Shapiro-Wilk test; otherwise a non-parametric sign test was employed. A p-value less than 0.05 was considered significant. Data were analysed as a whole and also stratified by current orthosis use (none, locked, or free knee).
Results
The opinions of the research participants were collected immediately after the completion of visit 1 (0-month) testing (Table II). All participants currently wearing an orthosis said that donning and doffing the DKBS was more difficult than their own orthosis. Stability while standing and walking with the DKBS was rated as acceptable to excellent and slightly better than other braces. All participants considered the orthosis heavy, and it was deemed heavier than the other knee orthoses used by the participants. Participants noted the cosmesis of the orthosis was worse than with other orthoses they had used. It was slightly more difficult to sit down and stand up with the DKBS. The subset of individuals who used a locked brace had similar opinions; locked KAFO users rated their stability while standing when using the DKBS as acceptable to excellent, although slightly less stable than with other orthoses. For free knee orthoses wearers, after visit 1 the only statistically significant comment was that cosmesis was worse than other orthoses that they had used. For persons not wearing another brace at visit 1, only the weight was an issue, with these participants finding that the DKBS was heavy.
Consumer opinions of DKBS at initial fitting.
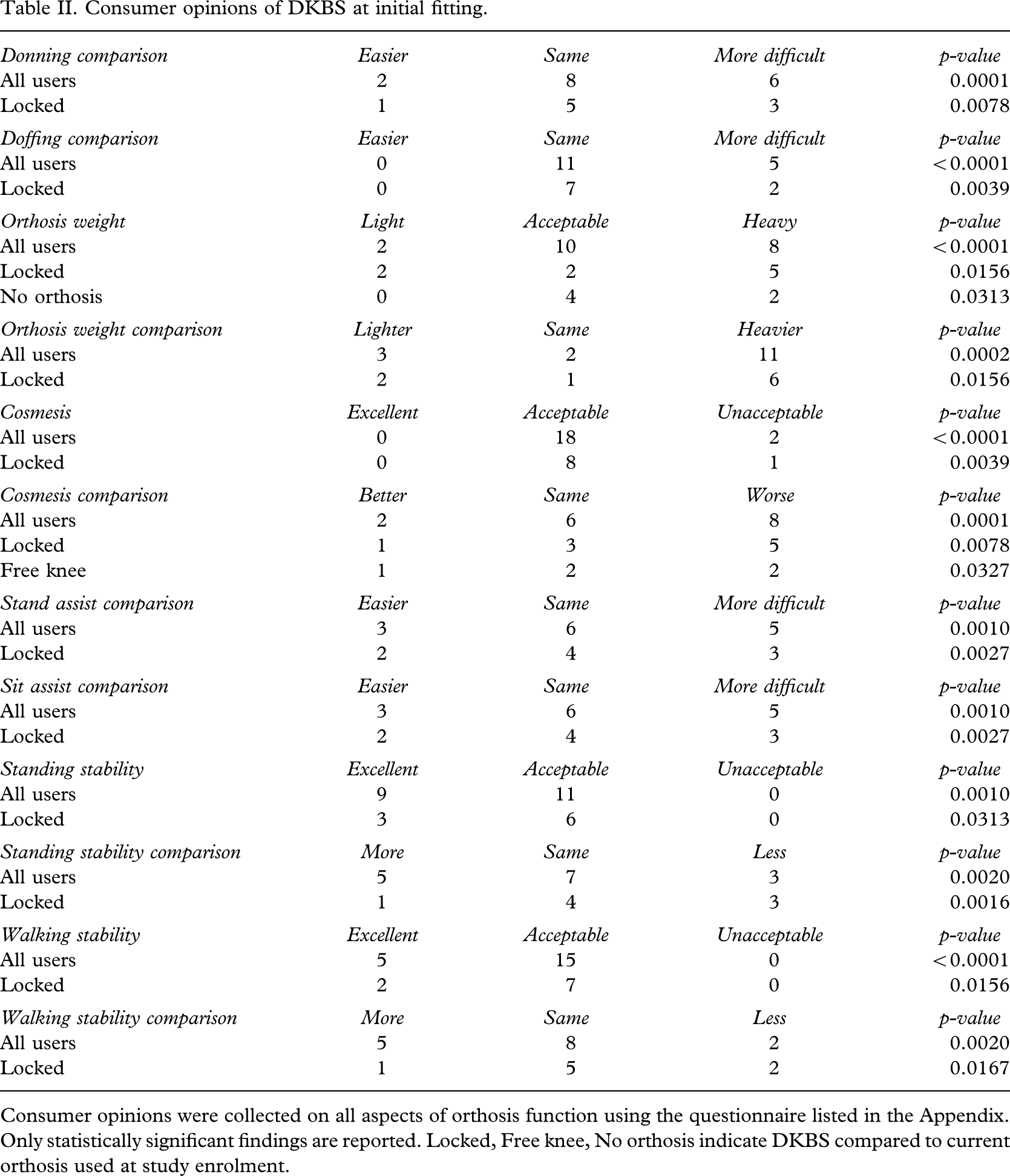
Consumer opinions were collected on all aspects of orthosis function using the questionnaire listed in the Appendix. Only statistically significant findings are reported. Locked, Free knee, No orthosis indicate DKBS compared to current orthosis used at study enrolment.
The consumer opinions were collected again after they had been given some time to accommodate to the orthosis (Table III). After visit 2 (3-month), participants once again said the DKBS was more difficult to don and doff than other orthoses. Standing and walking stability with the DKBS was rated as acceptable to excellent, and slightly better than other orthoses. The DKBS was considered heavy, and participants with previous orthosis use said it was heavier than their others. Users stated that the cosmesis of the orthosis was again slightly less than acceptable and worse than in other orthoses. Participants currently wearing an orthosis said that their ability to stand up was the same as with past orthoses, but it was slightly more difficult to sit down with the DKBS. Those who had been wearing a locked knee orthosis considered donning and doffing more difficult than with a standard KAFO. Locked KAFO users said their standing stability was slightly better than in a locked orthosis. Walking stability was rated acceptable to excellent, although slightly less stable than with past orthoses. Sitting down was found to be the same with the DKBS when compared to a locked KAFO. For free knee orthosis wearers and those participants not wearing an orthosis, no items were statistically significant.
Consumer opinions of DKBS at follow-up (3-month) visit.
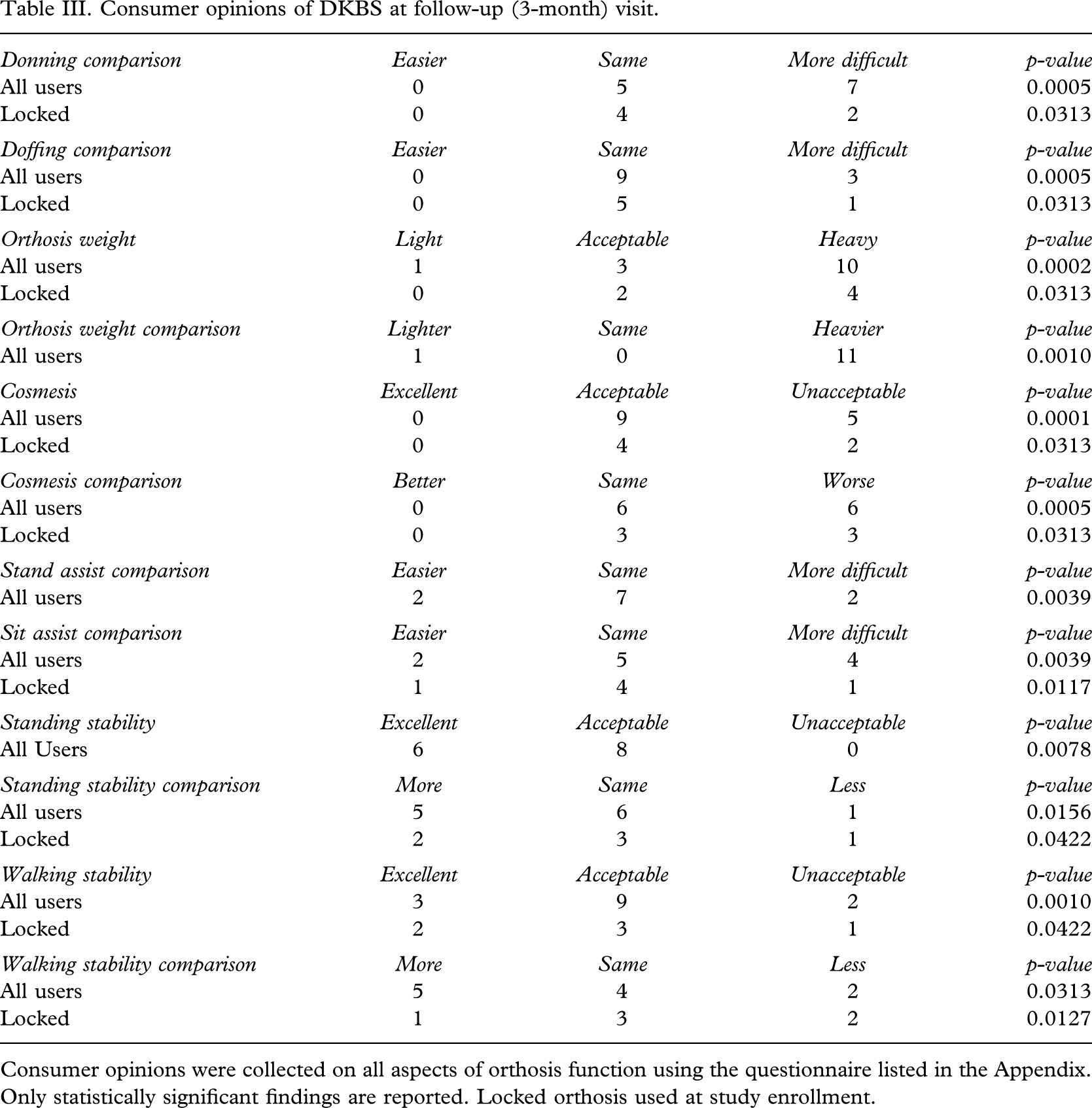
Consumer opinions were collected on all aspects of orthosis function using the questionnaire listed in the Appendix. Only statistically significant findings are reported. Locked orthosis used at study enrollment.
When combining data from all participants over multiple visits, opinions of the DKBS did not change significantly over time. Opinions on all questions at the beginning and at the 3-month point of the home trial period were roughly the same. For that reason the consumer opinions at the 6-month period are not reported since there were no changes reported.
As a whole, the participants were satisfied with the stability of the DKBS during both walking and standing, even rating it slightly better than the ones worn in the past. The only exception was with the locked KAFO user group. At the first visit, they had a little less confidence in their standing stability, yet slightly more confidence in their walking stability as compared to their locked orthosis. After the second visit, their opinions had switched, with these participants noting the DKBS had better standing stability and slightly worse walking stability than a locked KAFO.
Discussion
Overall opinions of the DKBS were positive, and the results of this study suggest that the work by Batavia and Hammer (1990) and Phillips and Zhao (1993) hold true for a stance control orthosis as well. The survey questions that can be equated to effectiveness, reliability, and durability (factors found important by Phillips and Zhao 1993) had favourable outcomes. The DKBS scored well on its own and in comparison to the alternatives of a locked KAFO, free knee orthosis, or none at all. This study shows that using a SCO can be a positive experience for an orthosis wearer. Carefully matching a patient's physical capabilities to an appropriate knee joint mechanism can only further improve the experience. Very few concerns were raised over effectiveness, operability, and dependability of the DKBS; the factors deemed most important by Batavia and Hammer (1990). Many study participants went so far as to say that if a SCO was reliable and made it easier to walk, then some added weight or material volume at the knee would be acceptable. In fact, a number of the participants who considered the DKBS heavy also noted that it did not feel as heavy compared to a locked orthosis when the stance control mechanism was activated. The need for additional gait training with this orthosis, although a considerable time investment for both the user and the investigators, would not be enough of a concern to discourage SCO use, given the previous report by Batavia and Hammer (1990). The most common complaints (weight, cosmesis, and donning and doffing difficulty) match well with the concerns reported in previous studies (Fisher and McLellan 1989; Batavia and Hammer 1990). According to Phillips and Zhao (1993), the factors where the DKBS scored poorly would not lead to eventual abandonment of the SCO.
The statistically significant points regarding knee joint size and weight were not wholly unexpected. Throughout the course of the study, all participants mainly commented on the size, weight, and appearance of the knee joint. Because the DKBS joint was significantly larger than a typical KAFO hinge, there was some difficulty noted in clothing selection. However, weight or limb alignment restrictions were not placed on the study inclusion criteria, thereby allowing nearly all interested parties to be included. Using the CDC criteria for body mass index (CDC 2004) 35% of the research participants could be considered overweight, 30% obese, and 5% severely obese. Based on patient selection criteria for the five commercially available SCOs, nearly half of the participants in this study would not qualify for at least one of these models because of their weight, the presence of a flexion contracture, or poor varus-valgus alignment (Otto Bock Health Care 2004; Becker Orthopedic 2002 Basko Healthcare 2004; Horton Technology Inc. 2004). By placing more stringent restrictions on who could use such a KAFO, the size of the DKBS joint could be significantly reduced. In fact, limited early testing was successfully completed by the authors with a much smaller version of the DKBS (Kaufman et al. 1996). The electronic controller and battery unit could also be made smaller in the future, with size currently being limited mainly by the production cost for the research components.
Donning and doffing of the DKBS was generally considered difficult, especially in comparison to other orthoses. Most participants attributed this to the fact that there is the addition of a battery to connect and disconnect when using an electromechanical orthosis. Interestingly, over the course of the study, many of the participants came up with their own way of carrying the battery other than the waist pack provided in order to make donning and doffing the orthosis easier. Some of the DKBS users also noted some difficulty getting dressed when wearing the orthosis under investigation, since the battery cord needed to be routed from the carrying location to the control box.
Based on the results presented here, a few changes to the DKBS would improve overall consumer satisfaction. While the subject population was happy with the operation and stability of the DKBS, the size and weight of the knee joint will need to be addressed. Producing multiple sizes and load capacities of the DKBS joint will allow many KAFO wearers to use a much smaller, lighter in weight version of the SCO used in this study. Likewise, reducing the size of the electronic controller and battery pack will improve the consumer's opinion of its cosmesis. By making these relatively minor changes to the SCO joint which has otherwise made a favourable impression, satisfaction with the DKBS would hopefully increase.
Footnotes
Acknowledgements
This study was supported by NIH Grant R01 HD30150, the Muscular Dystrophy Association, and the Mayo Foundation. The authors also wish to thank Prosthetics Laboratories and Prosthetic Orthotic Center, both of Rochester, MN, USA for their assistance with participant recruitment and KAFO fabrication and fitting. Kaufman and Irby are the inventors of technology used in this research, the technology has been licensed, and they have received royalties on it.