
Abstract
It has been reported that adult adoptees with histories of maltreatment face particular challenges when they become parents. Here we explore this issue using a qualitative analysis of the views of 14 adoptee mothers, who suffered severe institutional deprivation in the Romanian orphanages of the late 1980s before being adopted into the UK, and their adoptive parents. Following a thematic analysis, we report several perceived benefits of becoming a parent, as well as co-occurring difficulties and challenges. Benefits included a sense of accomplishment and fulfilment, feeling more motivated personally and professionally and the positive experience of having a relationship with a biological relative. Challenges related, in particular, to some adoptee parents’ abilities to appraise risk relating to their children and to difficulties in organising day-to-day activities. Practical and emotional support from adoptive grandparents was very often crucial for adoptee parents’ success and wellbeing. Implications for research and practice are discussed, emphasising that deprivation-related difficulties expand into adulthood and for some can impact their ability to parent.
Plain Language Summary
Care-experienced individuals are at an increased risk of having their own children taken into care. The reasons for this are currently not clear, but questions have been raised about the importance of early adversity versus a continuation of adversity, unfortunately commonly experienced by care leavers. The English and Romanian Adoptees (ERA) study has followed the progress of individuals who were adopted into high functioning homes following a period of early deprivation. Last assessed in young adulthood, 20% have become parents and in the current study, these parents, and their adoptive (grand)parents, were interviewed. Most parents reported no areas of difficulty and for them, becoming a parent had been a globally positive experience, which included a closer sense of connectivity, a sense of fulfilment and a greater sense of motivation. However, significant difficulties in providing childcare were experienced by around a fifth of the group, often resulting in care proceedings. Areas of difficulties appeared to revolve around appraising and responding to risk. Consequently, the adoptive grandparents were an important source of day-to-day support. Implications for practice and future research are discussed.
Introduction
Although adoption is considered a lifelong process, research has primarily focused on childhood and adolescence and consequently, pivotal transitions to and within adulthood, such as becoming a parent, remain largely unexplored (Greco, Rosnati and Ferrari, 2015; Field and Pond, 2018). New childcare responsibilities and associated challenges often require a fundamental re-orientation of a person’s life, involving a change in an individual’s outlook and lifestyle (Kluwer, 2010). Taking on this caring role requires a range of interpersonal, domestic and life skills (Lévesque et al., 2020). Individuals differ in the extent to which they possess these skills and/or in their ability to acquire them. However, with the appropriate support and guidance most people can become effective parents (Cowan and Cowan, 1995).
Since the 1990s there has been an increased focus on adversity experienced in out-of-home care and its consequences (Sköld, 2013). Register-based follow-up investigations suggest that a history of being adopted or growing up in foster care (referred to here as looked after people) can negatively affect a person’s ability to thrive in a parenting role and increase the risk that their own children are placed in the care system (Mendes, 2009; Fernandez and Lee, 2017). Official figures indicate that this risk increases with age; Winterburn (2015) suggests that at least one in 10 young looked after people (aged 16–21 years old) in England experience having a child being taken into care. In a study of older participants, Roberts and colleagues (2017) found that in Wales, 27% of mothers and 19% of fathers (n=374) who had their children taken into care had themselves been adopted or fostered. These findings are consistent with studies conducted in the USA (Courtney et al., 2007). While not focused on establishing causality, these studies implicate a potential role of historical exposure to adversity (i.e., abuse or neglect) and associated elevated mental health difficulties.
Mental health impacts of early adversity commonly experienced by looked after people are complex and can include elevated levels of conduct problems and/or emotional disorders. In severe cases these may extend to neurodevelopmental conditions such as attention-deficit/hyperactivity disorder (ADHD; Meltzer et al., 2003) and symptoms of autism spectrum disorder (ASD; Sonuga-Barke et al., 2017). These may be responsible for some of the parenting difficulties adoptees face when becoming parents. There is some evidence that adoptee depression may mediate difficulties providing childcare via higher rates of neglect and physical punishment (Banyard, Williams and Siegel, 2003). The role of elevated neurodevelopmental problems, in this regard has not been explored to date. However, there is a literature on non-looked after parents with neurodevelopmental disorders. A recent review of parents with ADHD identified several areas of difficulty (Friedrich et al., 2017). These include lower rates of family cohesion and higher rates of parent–child hostility (e.g., Agha et al., 2013), lower rates of parental satisfaction, higher rates of intrusiveness (Watkins and Mash, 2009) and inconsistent discipline (Chen and Johnston, 2007). To date, very little research has focused on the experiences of autistic parents (Murphy, 2021). Discursive papers published on this topic have highlighted that there are concerns that qualitative differences in parenting may be perceived negatively and that there is a lack of specialist support (Murphy, 2021). However, these studies also highlight that autistic parents may be able to support their children more effectively, if they also have a diagnosis of autism (Crane et al., 2021; Murphy, 2021).
Larger-scale studies help to highlight a general risk among looked after people, but they can only play a limited role in shedding light on the precise nature of the parenting problems faced by these parents and consequently what sorts of specific support are needed. Smaller-scale qualitative studies with an experiential focus are a better way to provide this more granular analysis. As reflected in recent reviews (Field and Pond, 2018; Despax and Bouteyre, 2019), these studies have focused on the experiential reflections of becoming a parent. In doing so, such studies have highlighted several positive and negative experiences related to becoming a parent. On the positive side, becoming a parent as an adoptee can provide an opportunity to reflect on one’s own identity (e.g., Conrick, 2020). In particular, this transition can evoke a new interest in one’s own genealogy (e.g., Pinkerton, 2010) and can provide a deeper layer of meaning whereby adopted parents integrate their biological and adopted origins (Pinkerton, 2010; Battalen et al., 2019). Having a child can also foster a greater sense of belonging (Grotevant, 1997; Hampton, 1997; Grotevant et al., 2000; Greco, Rosnati and Ferrari, 2015). More negative experiences can include doubt about one’s own perceived parenting ability (Horowitz, 2011) and concerns about being judged too harshly by support services due to stigma (Chase et al., 2006). This study supplements this existing literature on parenting by adoptees by extending the range of adversity experienced by adoptees to early, profound deprivation.
The Current Study
In the current study we interviewed young adoptees who had become parents (mothers), and their own adoptive parents (the adoptees’ child’s grandparents), about their experiences of becoming a parent, the day-to-day challenges and difficulties entailed, as well as the positive and negative impacts on the adoptee themselves. The adoptees had all suffered up to 20 months of severe deprivation as young children in Romanian residential childcare institutions prior to the fall of the communist regime in 1989 and were then adopted by families living in the UK. All are participants in the English and Romanian Adoptees (ERA) study (Sonuga-Barke et al., 2017). In the institutions, care varied from poor to appalling with severely inadequate levels of nutrition and hygiene, little or no cognitive stimulation and no opportunity to form attachment with carers.
Our interviews focused on perceived benefits and challenges of parenting and not broader, more abstract issues such as the adoptees’ own experiences in the institution and how this may have impacted caregiving. Our investigation employed an inductive qualitative thematic approach, given the limited amount of prior research in this area and so that our findings would not be constrained by any prior conceptions. In addition, we interviewed the adoptee mothers and their adoptive parents (referred to from now on as grandparents) – the latter providing an insightful additional perspective. The research questions which motivated our study were:
How do adoptees with a history of extreme early deprivation describe the transition to parenthood? What are the perceived challenges and positive and negative impacts of taking on the parenting role? Do adoptee parents and their adoptive parents describe similar, or different, positives and difficulties?
Method
Recruitment And Sample
The study was part of the ‘Young Adult Follow-up' phase of the longitudinal ERA investigation and was an opportunity to conduct an in-depth, small-scale investigation of the needs and experiences of the adoptee parents. As with previous waves, both young adults and their parents were invited to take part, and both were aware of the others' participation. Of the 15 Romanian adoptee mothers in the full sample, 14 (9% of the full ERA sample) participated in the current study. At the time of interview, all participants were resident in the UK. The length of time in the institutions before adoption ranged from 0 to 20 months. In adolescence, four mothers met the criteria for ADHD, one mother met the criteria for ASD and six mothers had cognitive impairment (IQ < 80). Two mothers met the criteria for ADHD and cognitive impairment; two mothers met the criteria for ADHD and autism. At the time of interview, they were on average 24.1 years old (age range 22–25 years). Also, at the time of interview, all the mothers lived with, and provided care for, their children. Nine of the mothers had one child, four of the mothers had two children and one had three children. Twelve of the 14 mothers were living with partners and eight were married. Two mothers were living with their own parents at the time of study. Seven of the mothers had undertaken a college or university course and six of them were employed. The adoptee mothers’ children were between nought and six years of age. There was one father in the cohort, whose data were not included out of concerns around disclosure.
Parents of all 14 mothers (the grandparents) took part in the current study and were 61.1 years old on average (age range 51–75 years). Of the 14 families, 11 were high socio-economic status, based on parents’ profession during the age-15 wave of the study. The grandparents’ nationality was British in all but two cases, with the remaining two coded as ‘Other’.
Procedure
Participants from the cohort and their parents were contacted by a researcher and gave consent to participate. Semi-structured interviews were recorded and were part of the ‘Young Adult Follow Up’ of the ERA investigation. Transcripts were made of the data. Most participants were interviewed in their own homes, although four interviews were conducted online (two grandparents and two mothers). Given the neurodevelopmental issues experienced by the adoptees in this sample, interviewers were instructed to provide prompts where necessary and to allow for breaks and opportunities to reflect upon and revisit previous questions. Interviewers were also instructed to halt interviews should a participant become upset or uncomfortable. The mean interview length of the adoptee mother interviews was 32 minutes (range 5–67 minutes), the mean length of interviews with grandparents was 38 minutes (range 19–52 minutes). In each case, both adoptee mothers and grandparents were interviewed separately. Six of the grandparent interviews included both grandparents, eight were conducted with the grandmother only and one was conducted with the grandfather only.
Interviews focused upon the adoptee mothers’ needs, experiences, achievements and relationships from the ages of 15–25 years (reflecting the point at which they were last interviewed and the emerging adulthood phase of life (Arnett, 2000)) – both in general and relating to their parenting role in particular (see Appendix). Mothers were asked to describe their experience of the transition and were prompted to recount what had gone well, whether they had experienced any difficulties, what support they had received and how helpful this support had been. Transcription was ‘intelligent verbatim’, whereby verbal utterances (e.g., ‘uhm’ and ‘ah’) were retained but non-verbal (e.g., sighs and laughter) were not. Also, abbreviated words in the interview were presented as formal, complete words in the transcripts. Following that, all data were anonymised to protect the identities of the participants. As part of the anonymisation process, cases were numbered and names were removed. The study was approved by the ethics committees at King’s College London, UK (5447) and the University of Southampton, UK (14308).
Data Analysis
Thematic analysis on a sematic level was undertaken, from an essentialist/realist perspective (Braun and Clarke, 2006; 2019), as the aim was to directly present participants’ own perceptions and experiences. The six-step method of Braun and Clarke (2006; 2019) was used:
Familiarisation with the data Transcripts of the interviews were read repeatedly. Initial case notes were made using the young adult and parent transcripts, including summaries of events and experiences which mothers or grandparents described in the interviews. Generation of initial codes Interview transcripts were read repeatedly. Notes were made regarding possibilities for theme development. Mother and grandparent interview transcripts were analysed separately. Generating themes Mother and grandparent interview transcripts and preliminary notes on potential themes were read and cross-referenced. Notes were expanded to include more detail of the effects of parenthood on the adoptees’ self-concepts, and also on perceptions about the nature of their parenting. Tables presenting candidate theme titles, explanations of the candidate theme titles and exemplars were formed in this stage of the process. Direct coding of transcripts was conducted using NVivo. Reviewing themes Candidate themes, explanations of themes and exemplars were discussed at team meetings. The most apt and salient candidate themes were selected and developed. Defining themes Themes were discussed and evaluated in review meetings. Relevant and concise thematic titles were formed. Coding in the case notes was amended accordingly. Producing the report Data from the transcripts were anonymised. Appropriate quotes were selected for explanations of themes.
Findings
Two overarching themes were developed. Theme 1 captured a range of positive consequences of taking on the parenting role, while Theme 2 outlined the challenges associated with the role. See Table 1 for an overview of themes and their sub-themes.
Themes and sub-themes.
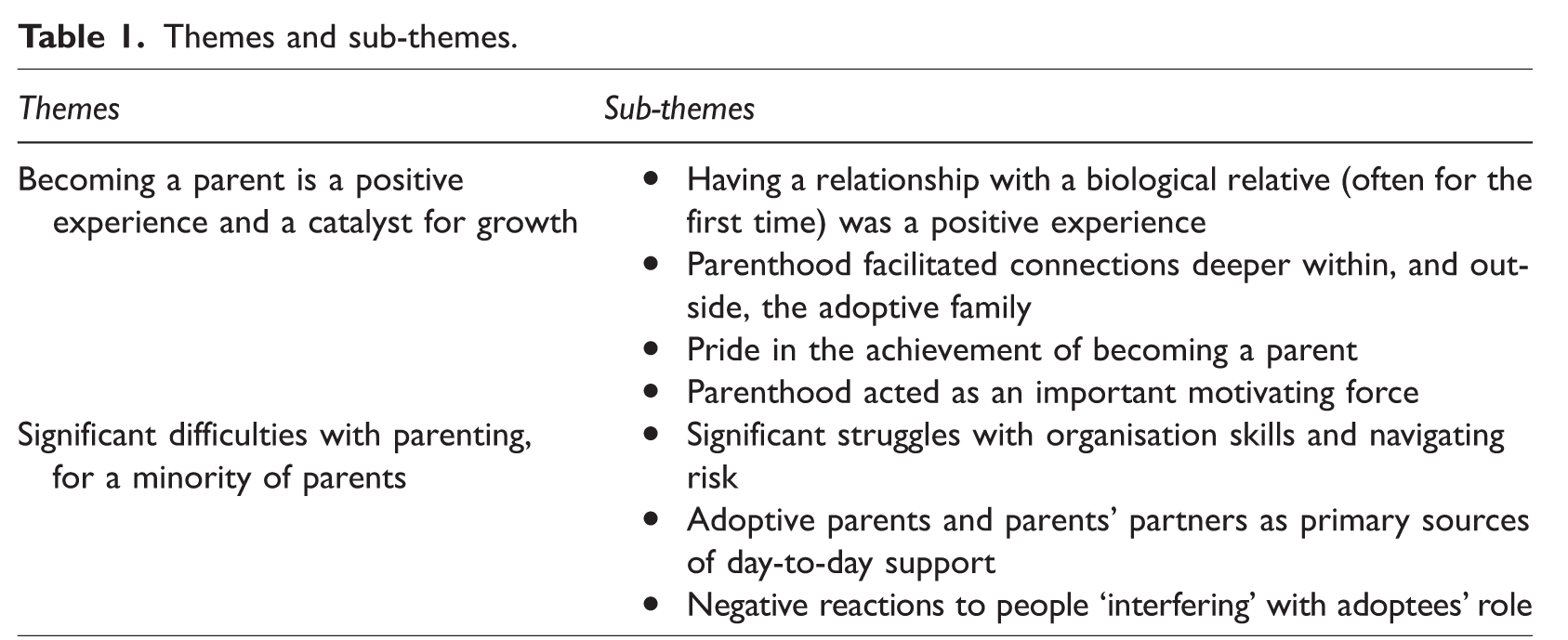
Theme 1: Becoming A Parent Is A Positive Experience And A Catalyst For Growth
Adoptee mothers and grandparents believed that a series of positive changes had occurred during the transition to parenthood. Within this overarching theme, four sub-themes were developed. First, mothers experienced additional benefits of having a new biological relative – especially where they had not been in contact with their birth families. Second, having a child reinforced connections within and outside their adoptive family for mothers. Third, mothers took pride in the sense of achievement of becoming a parent. Finally, parenthood was described as a motivator, which had led mothers to change various aspects of their lives.
Having A Relationship With A Biological Relative (Often For The First Time) Was A Positive Experience
For many mothers, having a child of their own meant that, often for the first time, they had a relationship with a biological relative. This promoted a sense of connectedness that helped them make sense of their own life experiences. In one particularly illustrative account, a mother described this positive impact: Because of things happening as I became a young adult to my adult age now, I didn’t understand why things were going … things happened and why things were how they were, or I felt how I did or I did things. But now, having [a child], everything makes sense. It’s kind of ‘Uh, I was like that because I was missing this in my life’ or I was missing feeling like that, or missing closeness or a connection with somebody and having that. (P14) I personally feel I am much better and much happier, and my relationships are better and my feelings are better and I think now I’ve got her [my child] everything is brilliant, on top of the world. I feel happy. No matter how bad or financial or…you know, or any little anxieties, nothing matters anymore because I feel … you know, she’s mini … you know, she’s me. (P14) I also feel complete. I think that’s what it is. I feel complete in myself that, you know, if I … I think it would have been very hard. If I couldn’t ever have children, I think it would be … well, I think it would be a very difficult and emotional life I would have. (P14)
Parenthood Facilitated Deeper Connections Within, And Outside, The Adoptive Family
Both mothers and grandparents perceived that having a child led to greater social connectivity for the adoptees. Me and my mum and dad have only kind of just really, well, me and my mum and dad have only just kind of got really close since my daughter was born. (P1) I think that’s a huge achievement for them, that what they are doing is they are trying to forge a relationship with my grandchild’s father so that they can both co-parent and I think that’s huge. Really enormous. (GP1) And when she’s met new friends in shops or with nursery schools and toddler groups, and she’s made some friends …. She’s actually made friends in [the local area] – well, you do when you’ve got a baby. (GP14)
Pride In The Achievement Of Becoming A Parent
For some mothers, especially those with neurodevelopmental problems (deprivation-related ADHD and ASD), finding and retaining employment and maintaining social relationships had proved difficult. Consequently, some mothers had developed a sense of low self-worth regarding what they could achieve in life: I didn’t think I would get married, have a house, a baby in one year. I didn’t think I’d ever have that. I just thought I’d be stuck at home all the time, getting into trouble. No, it’s [my situation in life] turned around completely. (P11) … my child is one of those good things.…I don’t know, that’s kind of the only thing that I feel that I’ve been really successful at … being a parent. (P14) … because they are so capable, you see, I don’t worry about her being able to look after themselves and their family. (GP2).
Parenthood Acted As An Important Motivating Force
Mothers and grandparents noted that parenthood had resulted in a change in lifestyle, which for some took the form of a more positive outlook on life: Life, I think, is positive because I’ve got [my child]. I don’t see … maybe, probably before I had her, I would see lots of negatives, lots of … but now I’ve got her, everything is positive to me. Or I certainly try and find the positive in everything. (P14) Yeah, I am a lot more [independent] since I’ve had children…I don’t know, just realised that you have to be, you know, strong and there for them. They rely on you; they’re dependent on you, so, yeah. (P13) I’ve had to. I’ve become a mum. You can’t be immature. You’ve got to grow up and let them be immature now. You’ve got to be the mature one. I’ve grown up a lot, but I’ve grown up very quickly. I think that’s the shock of it; I’ve had to grow up. I’ve had to grow up quickly. Yeah, I’d like to be going out, you know, what you do in your early 20s. But I’ve had to grow up very quickly. But I’ve done it. I’ve managed it. (P6) I’ve got things that are important to me now. I’ve got, you know, my family and my children, my husband erm, my house and all that kind of stuff. So, I just want to sort of get my career on track now. (P3) I mean I just take my hat off, because from, yeah, okay it’s helped having quite a bit of money……but I’m not saying that without that, they couldn’t possibly be where they are exactly now without the financial help, but even without that, they were determined to, you know, look after their child, their children and make something of her life. (GP13)
Theme 2: Significant Difficulties With Parenting, For A Minority Of Parents
This second theme encompassed three sub-themes. First, in addition to the general challenges of becoming a parent, a minority of mothers in the study (20%) experienced more substantial difficulties which had led to intervention by social services, with children being placed into care arrangements with grandparents. Second and more broadly, where difficulties had arisen, the grandparents had taken on responsibility for most of the day-to-day support for their grandchild. Third, mothers described reacting negatively to people who they felt were ‘interfering’ with their role as parents – often leading them to reject advice. However, it is important to note that the positives identified in the first theme and the challenges discussed were often experienced by the same participants. In other words, despite caring deeply for their children and taking pride in becoming a parent, challenges were nevertheless experienced.
Significant Struggles With Organisation Skills And Navigating Risk
In addition to experiences described as typical of becoming a new parent, this second theme depicts a range of specific challenges experienced by this group of mothers.
An example raised by a grandparent of the more typical challenges faced when becoming a parent is: But she’ll always be on the phone, you know erm, oh ‘How do I make a cheese sauce, Mum? What number on the machine should I put sweaters at?’. You know, not now but sort of over the time, just all sorts of stuff like that…then of course when she had the baby, you know, ‘He’s been crying for an hour. What shall I do?’ and just … yeah. (GP8) The baby was allowed to crawl around on the floor and put erm, anything in its mouth. And we took [an object] out once when we were round there, pulled it out of her mouth. You know, very … very serious. (GP4) Grandparent 1: Because you know, just little things to us perhaps but big things to a child. You know, a parents’ evening she has forgotten, or supposed to dress him up in some particular outfit … Grandparent 2: She doesn’t read the letters that come home from school. They have never had the skills … I mean she probably could fill the form in, [they] just don’t have the confidence to do it. So, we have to fill the form in, go through it with [them] and then get [her] to sign it. That sort of thing is happening all the time. (GP5) Grandparent 2: Which is not to say, they’re a bad parent. Grandparent 1: Oh no, they love them dearly. Yes, [I’m] very proud of [the parent]. Grandparent 2: They love [their child] dearly. But it’s just, they have always had real difficulty in organisational skills, and that goes back a long way. That was one of their problems at school – they can’t organise themselves. I wouldn’t call her a great mum er by any means [but], erm I don’t think she deserves to have her children taken away. (GP4) [They’re] really up against it with [themselves] though. [They], you know, [they] find it very hard. It would be like me going around with a 100-pound pack on my back. You know, it makes everything very difficult for [them]. (GP4) There’s no doubt about it that they’re very, very proud of their child and, and I’ve got absolutely no qualms in saying this to you, that they do their absolute best for them. It’s just sometimes their best isn’t quite good enough. But you know, they are learning and it is very difficult for them. (GP1)
Adoptive Parents And Parents’ Partners As Primary Sources Of Day-To-Day Support
This sub-theme also had two components: first, it was perceived that day-to-day support was provided by grandparents to grandchildren; second, in a minority of cases, grandparents described taking on the primary caregiver responsibility.
In these cases, mothers described examples of support from grandparents, such as advice in certain situations: …because my mum’s my mum, you know, and she’s been a mum, she’s helped me a lot be the mum I have to be for my daughter…like if I, if my [child] is having a two-minute tantrum, as they do, like how to deal with it or, you know, like erm the best, healthy options for a kid, food, everything. Everything and anything. (P1) Grandparent 1: And we still ask her, you know, [have you] got enough clean clothes for school next week? You know those sorts of things. Grandparent 2: Yeah, yeah. And in fact … I was doing the washing of the uniform, initially, in order to make sure that she was coping. (GP5) Well, most of our friends tell us, ‘You know, if you didn’t support them in that way…. they would have to or they would have to do it,’ but we know them and we know full well that wouldn’t happen. (GP5)
Negative Reactions To People ‘Interfering’ With Adoptees’ Parenting Role
Mothers described difficulties accepting advice and support from others, including their own adoptive parents. Sometimes, advice was dismissed by mothers as interfering: They do struggle to allow me to be independent. Erm, they have always got their views about things and, you know, childcare and things like that and have sort of quite often pushed them on me. But we are doing alright. (P3) I’m not allowed to take her children out because it’s so long since I’ve brought up a child that I might not know how to do it, and silly things like that. (GP4)
Other times, parenting advice from grandparents was seen by parents as questioning their parenting abilities in an unfounded way: They didn’t think I could cope. I can, I do have hard times, don’t get me wrong. And I do think there’s times when I can’t cope. But I have strong people around me to put me back together and say, ‘You can do this,’ you know. But she always questions my parenting which really upsets me. (P6) My parents decided because they are geniuses and doctors themselves – which they’re not – erm that it wasn’t right and that I wasn’t taking [the child] to the doctor…and that was awful because I’m trying my best and I was a new mum and I had done nothing wrong. (P4) She said to me one day, ‘I couldn’t have coped with a baby if it hadn’t of been for you and Mum’. So I was quite surprised. (GP11) Basically, she lost her cool and hit the social worker … the police…took her [and the child] away…into care. (GP3) Grandmother 3: They are still against [the parent], even up to this day. You know, they have to do a report now and again, you know, when they go round to see them and they don’t put a very good report, even now. You know, like [they’ve] got a very basic house, there’s toys everywhere, you know, the house is chaotic, you know, and … so they still don’t praise [them], do they? Grandfather 3: They seem as though they want to put everything negative regarding [the parent], but they never put a positive thing in at all. The fact that [they’re] in [their] own home with [their partner and child], feed them well, what more would you expect there to be in a home than toys about, you know?
Discussion
Previous research has highlighted the challenges of parenting faced by looked after people, possibly resulting from early maltreatment. In some cases, this led to the children of adoptees themselves being taken into care, due to child protection concerns (Roberts et al., 2017). Past research has also highlighted some positive benefits of taking on the parenting role for these parents. In keeping with this mixed and complex picture, our thematic analysis of the text from interviews about parenting with 14 mothers who had experienced severe deprivation in early life and their adoptive parents (the children’s grandparents), identified a range of positive experiences and outcomes, as well as areas of difficulty. There were several findings of note.
First, the overall message from the interviews reflected a positive experience of parenting. For the majority of adoptee mothers, becoming a parent had been an overwhelmingly positive experience and no substantial challenges were described. Positive impacts included a sense of pride and achievement, closer feelings of connectivity with their adoptive family, feeling more motivated and a greater sense of personal fulfilment.
Second, as in prior research (e.g., Conrick, 2020) our study suggests that that when people with a history of care become parents, they enter into a period of life review about their past experiences and a re-evaluation and updating of their sense of self. For example, the mothers in our sample described how having a biological relative in their lives engendered a greater sense of ‘completeness’. In doing so, this study adds to the literature that suggests adopted individuals ‘must cope with additional challenges regarding the integration of their personal history into a sense of identity’ (Greco, Rosnati and Ferrari, 2015: 39).
Third, becoming a parent also affected personal relationships and social networks. Their relationships with their own adoptive parents, while already often positive (Sonuga-Barke et al., 2017), were seen by both the mothers and grandparents as having improved since the birth of the child. This relationship strengthening effect also applied to that between the mother and the child’s other parent, an area which less is known about (Despax, Bouteyre and Guiller, 2022). More generally, social difficulties have been identified as an issue in some adoptees with a history of adversity (Golm et al., 2020) and again, becoming a parent seemed to improve matters here too. It was believed that some mothers had developed more friendships and/or strengthened pre-existing friendships, for example with other mothers.
Fourth, the perceived benefits of parenting extended beyond the emotional and inter-personal and included a desire to become more practically and financially independent. Indeed, many of the mothers and their adoptive parents reflected on how having a child had been an essential driver of their newfound successes, such as obtaining employment and a desire to live more independently. This finding both corroborates those of previous work (e.g., Maxwell, Proctor and Hammond, 2011) and expands upon them. Specifically, where previous research has highlighted more positive views of the self, we show here that these can also translate into a variety of day-to-day benefits with an overall effect on wellbeing.
Fifth, unfortunately around a fifth of the sample described specific difficulties with becoming a parent and providing childcare, a similar proportion to that seen in previous studies in this area (e.g., Chase et al., 2006). These difficulties appeared to revolve around a lack of recognition and response to child-related risk and difficulties with organisational skills. These were sometimes sufficiently impairing to attract the attention of social services. In contrast to samples of adoptee parents with depression and non-deprived parents with ADHD, we did not find evidence of harsh/physical parenting, or hostile parenting environments (Agha et al., 2013). Nor did we find evidence of neglect in terms of wilfully leaving children unattended, but there may be some parallels with a broader sense which includes struggling to meet basic needs due to a lack of organisation/attention (Banyard, Williams and Siegel, 2003). It is important to note that the positive and negative experiences we identified were not mutually exclusive and the group who described the difficulties also described having experienced the above range of positives.
Sixth, in adopting the somewhat novel approach of including multiple informants, in this case, both the adoptee mothers and their adoptive parents, we were able to highlight either similarities or differences in their respective reports. An example of this related to the sense of disagreement highlighted by adoptive parental support being seen as necessary by the grandparent, or intrusive by the mothers themselves. This underlines the additional depth of understanding one can gain from having multiple viewpoints. From the mothers’ perspective, unsolicited advice was sometimes seen as unnecessary, arbitrary and intrusive, whereas from the adoptive parents’ perspective, the advice was necessary due to the child being at risk of harm. Given the level of state intervention in many cases, while there was often value in the adoptive parent’s perspectives the problems may have been in how concerns were raised and framed.
Seventh, and a further benefit of including both mothers and their adoptive parents (grandparents), was that we were able to gain an understanding of the ongoing childcare support provided by the original adoptive parents. Grandparents often provide vital support. Interestingly, adoption support agencies were seldom mentioned and while not reported here due to the focus on adulthood, they were often seen as solely related to difficulties in childhood. This finding also relates to an important difference between our findings and those of previous work (e.g., Roberts, 2017; Roberts et al., 2017); the custody arrangements in our study were only temporary and involved the grandparents having custody, as opposed to the children being placed into foster care outside of the family. This may be due to our focus on adopted individuals who were exposed to early adversity rather than adoptees/people who grew up in foster care in general, and also the very high quality of the adoptive caregiving environments in our cohort (Sonuga-Barke et al., 2017).
Similar to other work, our findings suggest that support needs in this group could be better met, both in terms of what support is available and when it is deliverable. Where adoption support services were mentioned, it was in the context of historical support in childhood and was not raised in the context of difficulties providing childcare. It was not clear whether the support either did not exist or whether the participants were unaware of its existence. In addition, and again consistent with previous work, is the finding that general support services were perceived as more ‘unhelpful and punitive’ rather than supportive (Roberts, 2017: 14).
Limitations And Future Research
The current study presents a unique insight into the parenting experiences of adoptees with a history of extreme adversity and institutional deprivation, followed by adoption into relatively affluent UK families. There is an important difference between our participants and those described elsewhere. This involves the nature (institutional deprivation) and extent (unusually severe) of childhood adversity to which they were exposed. Another possible difference is that we have found no evidence of maltreatment within the adoptive homes, whereas the risk of this in more typical looked after cohorts is elevated (e.g., George and Harden, 2008). In addition to the day-to-day experiences that we highlight here, there may be other experiences in this group that were not addressed in this study, which nevertheless may impact upon parenting. For example, being an international adoptee in and of itself, and any challenges this may cause when searching for biological relatives. These issues could be raised in future, more reflective studies. A further limitation is that the current study used an ‘intelligent verbatim’ approach to transcribing, which does not include non-verbal content (e.g., laughter), which can aid understanding quotes (McMullin, 2021).
Other limitations to consider include that our focus here was solely on adoptee mothers, as there were too few fathers to include for analysis, likely due to the age at which the interviews took place. Thus, within this already under-researched topic, almost nothing is known about fathers’ experiences. Adoption and social services differ both over time and by region and so it is difficult to generalise the negative experiences of service contact to other groups of more recent adoptees or adoptees from different countries. Third, the small-scale, qualitative nature of our study means that this approach does not allow us to explore individual differences in experience of deprivation and/or adoption in a systematic way. For instance, it is plausible that some of the difficulties experienced by adoptees are related to the neurodevelopmental problems noted in the group, such as ADHD (Johnston et al., 2012). As more of the ERA sample, and similar cohorts, become parents, it would be useful to assess the nature of adoptees’ parenting with standardised measures to help identify specific areas in which the adoptees could be helped with the complex task of parenting. There could also be an examination of cognitive mediators, for example prospective thinking where we know there is impairment in the ERA adoptees to test whether these partially mediate the association between early adversity and later parenting difficulties. Such work should also endeavour to include fathers. Also, given that we have identified a range of putative protective factors associated with becoming a parent, a potential avenue for future work in this field is to use quantitative methods to see whether these might mitigate some of the poorer outcomes identified elsewhere in the study (e.g., lower employment rates, poorer mental health identified in Kennedy et al., 2016).
Finally, it must also be noted that the adoptees’ children were very young at the time of the interview. It is possible that as their children mature and gain more independence, the parent–child relationship could change and have a different impact upon the self-concepts of the adoptees in this study; therefore, a comprehensive, mixed-method follow-up study which can assess the impact of the developing parent–child relationships upon the adoptees (and any impact upon the child) would be beneficial.
Implications
There are four main implications of the current study. First, it adds to the literature suggesting that difficulties with parenting in looked after people may result from early adversity, rather than later adversity. Second, our findings suggest that these difficulties may take the form of difficulty predicting/navigating risk and organisational skills, which represent potential targets for support. Third, our paper adds to the literature suggesting that if the aim is to reduce the numbers of children requiring state care, those with a history of early adversity represent a key group to support. Fourth, our findings and similar work clearly suggest that adoption services (and awareness of such services) should extend beyond childhood and into adulthood and should also include ongoing support for the adoptive parents, where necessary.
Conclusion
Research on adoptees as parents remains relatively sparse. This study is the first to explore this issue in relation to adoptees who have experienced severe deprivation as children. We identified both positive and negative elements relating to the parenting role. Despite being adopted into high quality family environments, in a minority of cases difficulties with parenting were deemed severe enough to warrant temporary state intervention. Clearly for some, organised and professional support is needed to supplement that already provided by adoptive (grand)parents.
Footnotes
Data Availability Statement
Due to the disclosive nature of the data, it is not openly available. Upon request, anonymised, selected data may be made available.
Declaration Of Conflicts Of Interests
Professor Sonuga-Barke reports funding from Shire, Medice, grants from QBTech, personal fees from Neurotech Solutions. All other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper represents independent research part funded by the NIHR Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
The funders (The ESRC: ES/I037970/1 and The Waterloo Foundation: 686-4339) had no role in study design, data collection, data analysis, data interpretation, or writing of the report.