
Abstract
Severe, prolonged early deprivation is associated with later neurodevelopmental difficulties. Despite elevated levels of contact with service providers, these problems often persist into adult life and are associated with impairment in adulthood (e.g., unemployment, higher rates of depression and anxiety symptoms and poorer subjective wellbeing). Here, we aimed to explore the ongoing service needs and experiences of adoptees and their parents from the English and Romanian Adoptees (ERA) study, in those with a history of early deprivation and neurodevelopmental problems. Our descriptive thematic analysis highlighted difficulties with independent living, particularly financial management and problems with decision-making. Where specific forms of support had been accessed (e.g., medication for attention-deficit/hyperactivity disorder) they were often helpful, although there was some ambivalence towards taking medication due to side effects. However, the neurodevelopmental problems were not well understood and were often overlooked by service providers. There is a need for greater awareness among frontline service providers of the neurodevelopmental impact of early adversity. Participants also identified that their support needs were largely unmet and that their parents were having to fill this gap. Similarities and differences between the experiences highlighted here and those identified with idiopathic neurodevelopmental disorders are discussed, as are several recommendations for educational improvements for service providers.
Plain Language Summary
People who have experienced severe, prolonged institutional deprivation are at increased risk of neurodevelopmental disorders. Despite spending many years in warm, loving families, the English and Romanian Adoptees (ERA) study has shown that these problems often persist into adulthood and are associated with a range of negative outcomes. Importantly, these poorer outcomes seem to occur despite contact with support/service providers. In this study, we interviewed the adoptees and their parents about their support needs, and experiences with trying to obtain support and communicate with service providers. Support needs included help with independent living and support with managing finances. Our participants described a range of difficulties with obtaining support, including a lack of understanding of the link between early adversity and later mental health, and that neurodevelopmental problems were often overlooked. Consequently, the adoptive parents had largely been left to fill this gap in unmet needs. However, where support had been accessed, it was often described as helpful.
Introduction
Many adopted children have suffered maltreatment prior to their placement in new families, which is a risk factor for poorer psychological health (Hjern et al., 2002; Lindblad et al., 2003). For children exposed to early prolonged and severe deprivation, mental health difficulties can be compounded by neurodevelopmental challenges and cognitive delay (van IJzendoorn et al., 2020), necessitating high levels of social, educational and mental health support post adoption (Goldman et al., 2020).
The English and Romanian Adoptees (ERA) study has prospectively tracked the development of children who spent their early years in the severely depriving Romanian orphanages of the 1980s and who were then adopted into relatively affluent and stable UK families (Rutter et al., 2010; Sonuga-Barke et al., 2017). The findings of the ERA study have documented an early emerging distinctive and persistent pattern of neurodevelopmental difficulties, marked by symptoms of autism spectrum disorder (ASD; Rutter et al., 2007), attention-deficit/hyperactivity disorder (ADHD; Kennedy et al., 2016), and disinhibited social engagement (DSE; Kennedy et al., 2017) in a significant minority of participants who experienced extended deprivation (over six months). Cognitive impairment (CI), which was elevated in childhood, had remitted to a degree by adulthood (Sonuga-Barke et al., 2017), while emotional problems emerged strongly during the late adolescent and adult years (Golm et al., 2020).
Of these difficulties, symptoms of ADHD (with frequently co-occurring symptoms of ASD) have been shown to be particularly elevated in those affected by early prolonged deprivation (in adulthood, those with over six months deprivation were almost eight times more likely to be affected than those with fewer than six months (Kennedy et al., 2016). These same quantitative analyses also showed that a significant portion (40%) had received clinical intervention (i.e., at least two visits to a service provider resulting in either a diagnosis and/or an intervention). However, despite this support, ADHD was still particularly impairing, with strong effects on unemployment (88%), lower educational attainment (77%), higher rates of depression and anxiety symptoms and lower perceived quality of life in adulthood. More generally, in similar cohorts, rates of ADHD have been shown to be consistently elevated following early adversity (van IJzendoorn et al., 2020).
The literature on adoptees’ service needs and experiences as a whole is limited to childhood and adolescence (Luke et al., 2014). Given that adoption, as an event, most frequently occurs in childhood, this is to be expected. However, adoption is increasingly understood as a lifelong process (Field and Pond, 2018). Nevertheless, studies in childhood have highlighted a range of service needs of adoptees following adoption, including support for early emerging internalising/externalising problems, bolstering of relationship quality/attachment bond formation with the adoptive family, help strengthening educational attainment, recognition of later emerging struggles with identity formation, and for international adoptees, addressing concerns around discrimination/stigma (Hartinger-Saunders and Trouteaud, 2015; Ryan and Nalavany, 2003; Zosky et al., 2005). The evidence base is broadly consistent in finding that there is usually an initial period of catch-up, provided that adequate care is put in place (e.g., Turner at al., 2022) and also that after this period, there remain elevated levels of difficulties for a significant minority of adoptees and that these problems can persist into adulthood (e.g., Sonuga-Barke et al., 2017). Experiential focused studies have shown that barriers to receiving appropriate support in childhood and adolescence include a deficit of specialised care provision, a lack of a ‘joined-up approach’ in service provision, an absence of awareness of what support is available, instability in the caregiving environment, variability in the extent to which caregivers are able to advocate on behalf of the young person, and disengagement from the young person themselves (Luke et al., 2014; Zosky et al., 2005). While these findings provide some direction, it cannot be assumed that these issues persist into adulthood, as they are often targeted for intervention, which are at least moderately effective (Luke at al., 2014). There is also evidence of remission in adolescence (Beckett et al., 2008) and the possibility that new issues may emerge.
The evidence base related to adoptees who have experienced early adversity is similarly limited to childhood. When the adoptees in the ERA sample were in early adolescence, there was some overlap between neurodevelopmental problems and identity issues, but on the whole, identity issues have shown signs of reducing over time. In terms of service use experiences, participants reported elevated contact with mental health services (primarily for neurodevelopmental problems) and high levels of special educational needs support, ranging from lesser provision, e.g., individual education plans (37.5% in the over six months group vs. 13% in the UK controls) to major provision, e.g., being educated in a special needs setting or being held back a year (39% in the over six months group vs. 10% in the UK controls). At the same time, parents reported concerns over the appropriateness and adequacy of professional service provision (Castle et al., 2006). One such concern raised at that time was a general lack of awareness of neurodevelopmental sequalae of early deprivation. However, this was not only in childhood but also was over two decades ago and consequently, almost nothing is known about the service use experiences of this cohort in adulthood. Accordingly, the current study sought to explain and expand upon our previous quantitative findings by adopting a qualitative design to help understand the service needs and experiences of those affected by environmentally mediated neurodevelopmental problems. To achieve this, we conducted a descriptive thematic analysis of a series of semi-structured interviews, conducted separately with the adoptees themselves and their parents, the latter providing a valuable additional perspective.
The research questions which motivated our study were:
What were the perceived service needs in the group and were they met? What were the barriers and facilitators of accessing support in this group? What role had the adoptees’ parents played in accessing and/or providing support?
Methods
Recruitment And Sample
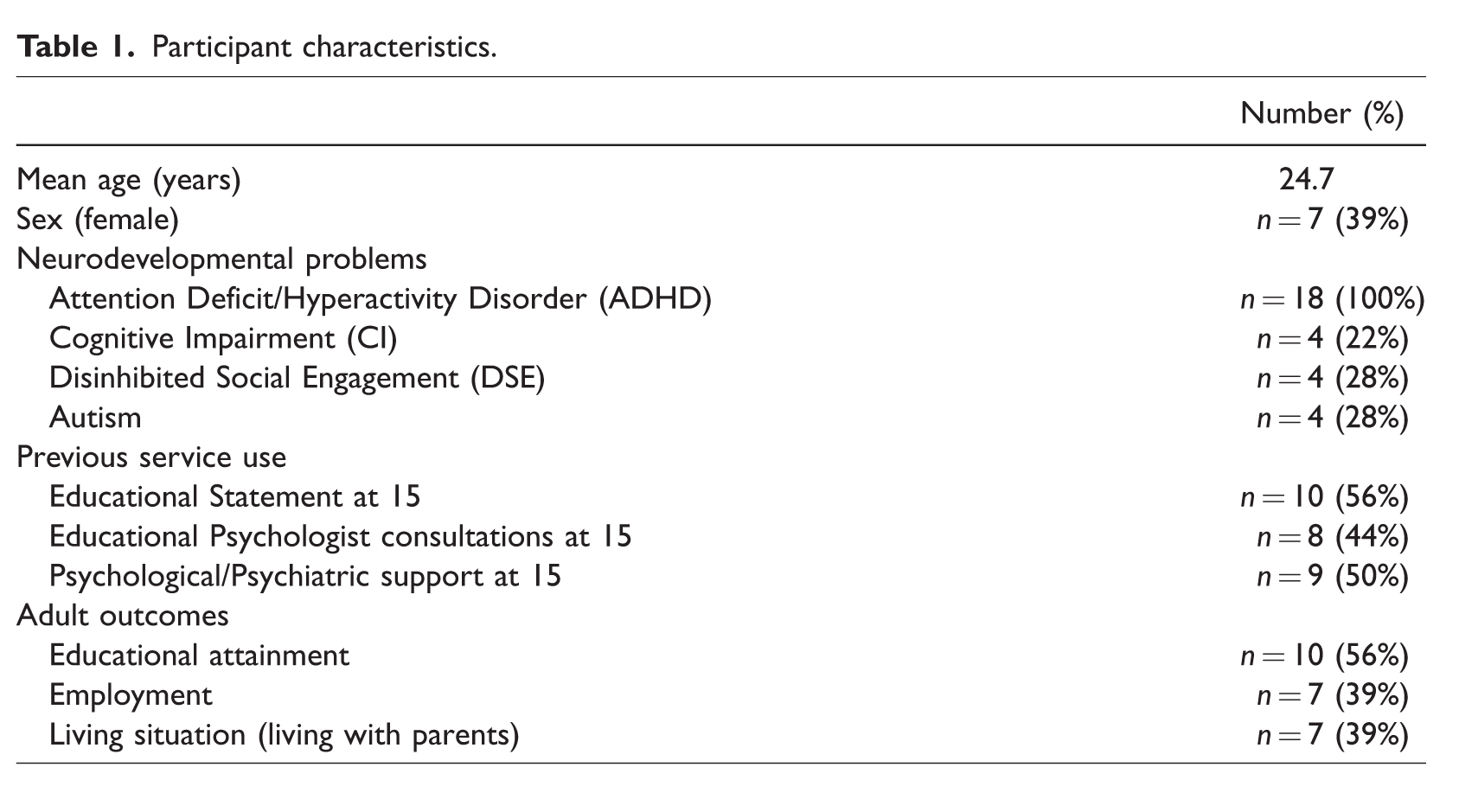
We focused on adoptees who had both spent more than six months in institutionalised care in Romanian orphanages and who also presented with a history of ADHD at age 15. Of the entire ERA cohort, 95 participants (n = 217) had spent six or more months in the Romanian orphanages following placement there at or shortly after birth. Of these, 18 met criteria for ADHD and were therefore included in the present study (11 young men and 7 young women). Our classification of elevated symptoms of ADHD was made based on the parent-report Strengths and Difficulties Questionnaire (Goodman, 1997) and required at least two domains to be endorsed (inattention, hyperactivity/impulsivity and distractibility), in line with DSM criteria (Sonuga-Barke et al., 2017). Of the 18, two adoptees opted out of the interview, so we interviewed 16 young adult adoptees and the parents of all 18 adoptees who met criteria for inclusion in the study. Interviews took place in participants’ homes between 2013 and 2015. In 10 cases, parent interviews were conducted with adoptive mothers and fathers at the same time. In seven cases, parent interviews were conducted only with mothers, and in one case an interview was conducted with only a father. Demographic data and historical service use for the 18 adoptees can be found in Table 1.
Participant characteristics.
Procedure
For this study, a qualitative design was chosen to gain a deeper understanding of the lived experiences of adoptees and their parents, as the former transitioned from adolescence to adulthood. Semi-structured interviews were used, following a standard topic guide. Interviews with young adults lasted on average 39 minutes (SD = 44 mins) and those with parents lasted on average 41 minutes (SD = 13 mins).
Interviews took place in the individuals’ homes and in accordance with good practice, were recorded and transcribed. Written informed consent was provided by participants. All data were anonymised during analysis. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008. All procedures involving human subjects/patients were approved by the ethics committees at King’s College London, UK (5447) and the University of Southampton, UK (14308).
Data Analysis
The transcripts were analysed via a Descriptive Thematic Analysis, following the six-step method outlined by Braun and Clarke (2006; 2019):
Familiarisation with the data (conducted by first author) Transcripts of the interviews were read repeatedly. Initial case notes were formed using the young adult and parent transcripts, including summaries of events and experiences which parents or adoptees described in the interviews. Generation of initial codes (conducted by first author) Adoptee and parent interview transcripts were analysed separately. Brief descriptions of some commonalities in participant perceptions of service support, adoptees’ functional and emotional difficulties and support needs were added to case notes. Generating themes (conducted by first and second author) Parent and adoptee transcripts were read and cross-referenced. Case notes were expanded to include more detail of the adoptee and parent perceptions of service needs and service use. Tables presenting candidate theme titles, explanations of the candidate theme titles and exemplars were formed. Reviewing themes (conducted by all authors) Candidate themes, explanations of themes and exemplars were discussed at team meetings, with all authors present. During these meetings, how codes fit into themes and how themes fit together was discussed. Defining themes (conducted by all authors) Following these meetings, themes were demarcated and final names were formed. Coding of transcripts was completed using Nvivo. Producing the report (conducted by all authors) Review of how the present findings related to previous studies within the ERA investigation, similar cohorts and the literature on adult ADHD was conducted. Data from the transcripts were anonymised. Appropriate quotes were selected for illustrations of themes.
To ensure that our approach was trustworthy and sufficiently rigorous, we applied Shenton’s (2004) four strategies (credibility, transferability, dependability and confirmability). Regarding credibility, we adopted a descriptive and inductive approach, which was in line with our research aims. What this meant was that the themes were generated from the data, as opposed to being decided beforehand, and that we aimed to reflect our participants’ meaning. Regarding transferability, we have reported on a range of participant demographics and provided relevant context amid the analysis. In addition, we discuss limitations to transferability in the discussion. Regarding dependability, the recruitment methods and study design have been described in detail both in this paper and in our previous publications. Furthermore, opting for a descriptive rather than interpretative analysis may strengthen this. Ensuring confirmability was a core aim of the regular whole authorship meetings, as described above, whereby the generation of initial codes/themes, the clustering into sub-themes and organisation of these into overall themes were discussed by the whole authorship team. Furthermore, the coder had not been involved in previous waves of the study, which may also reduce the possibility that findings were influenced by knowledge of prior issues the participants may have had.
Results
Three overarching themes were identified:
worries about the adoptees’ futures; concerns about difficulties in decision-making in everyday life; difficulties obtaining desired help and support and their sub-themes.
See Table 2 for an overview of themes.
Themes and sub-themes.
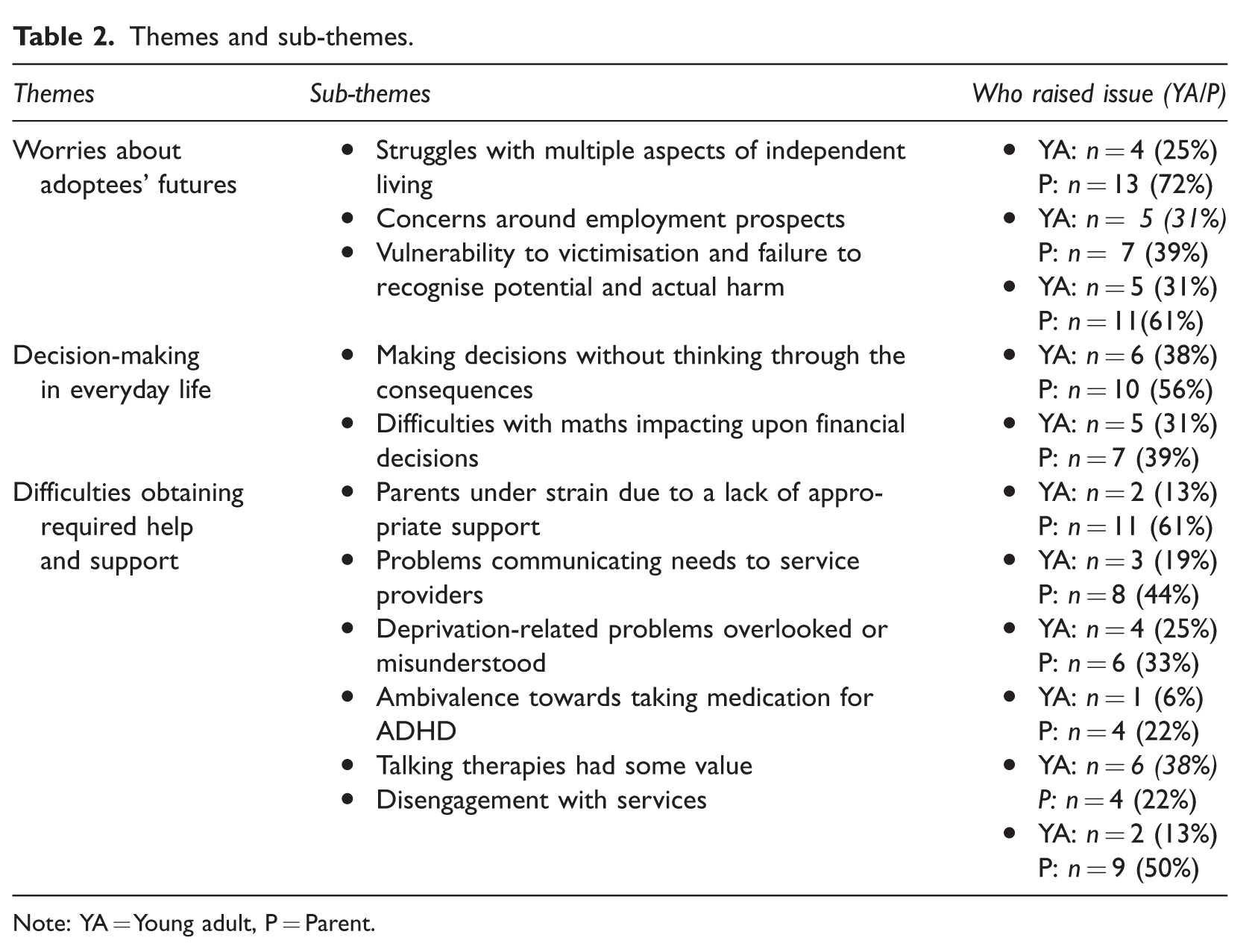
Note: YA = Young adult, P = Parent.
Worries About Adoptees’ Futures
The first theme referenced a range of challenges and the concerns these provoked about the adoptees’ futures. While the challenges were often acknowledged by the young adults, the associated concerns about the future were mainly raised by the parents. Concerns spanned multiple domains: difficulties with independent living; ongoing difficulties around employment; and a general vulnerability to victimisation.
Struggles With Multiple Aspects Of Independent Living
A core concern for the future described by parents was that their child would struggle to live independently without their ongoing support, despite continued efforts to facilitate their child’s successful transition to independent living. For example: They wouldn’t be able to do anything that would be expected of people at their age – look after themselves in a home environment, cooking, dealing with bills. (P, 9) I don’t think [they] ever will be [independent]. I can’t imagine that [they are] ever going to be able to live on [their] own without some kind of support. (P, 18) When we have discussions about what’s going to happen in the future, you know we’re not going to be [around] forever and all this kind of thing, and [they will] say, ‘Well, I can’t live on my own.’ (P, 9)
Concerns Around Employment Prospects
Another frequently mentioned source of concern for both young adults and parents related to the challenge of the adoptee obtaining paid employment and the limited opportunities for career progression. One parent (P, 7) worried their child was ‘not getting anywhere. They are just going round in circles … I feel very bleak about their future’.
Some of the young adults also commented on their struggle to obtain and retain employment. One young person (YA, 9) described how their learning difficulties had made this difficult on several occasions: ‘… but again I couldn’t get my foot in the door because of my learning difficulties’.
A number of the young adults and parents commented that they had attempted to go for more vocational roles, but were held back by the need for adequate written skills: … because at certain parts of the course you’d have to do, er, write … so they said she wouldn’t be able to do the English side of it. So that was like everything. (P, 2)
They continued: And if she’d progressed, then [the employer] would have had to seek expert opinion to find out what help she personally needed, because they didn’t feel they could help her. (P, 9)
Vulnerability To Victimisation And Failure To Recognise Potential And Actual Harm
This issue was raised primarily by parents. There were two distinct components to this theme, one being a general vulnerability to victimisation and the other linked to concerns that their child doesn’t have the insight to recognise the risk posed by other people acting in bad faith. Parents described scenarios where the young adult was seemingly targeted because of their vulnerability. For example, one parent reported that their child’s social naivety had been taken advantage of, whereby the young adult was repeatedly persuaded to pay for things on another person’s behalf after being told that this was normal. A concern raised by these parents was that their young adult children sometimes failed to ‘screen out’ those who wished them harm and were unable to recognise when they had been taken advantage of. For example: For instance, somebody came into the town and … was spinning this story about, you know, he needed this and he needed that, and my child actually took him into their home. They didn’t know him at all, and it turns out he was a con man. (P, 7) [A] guy that came and said, ‘Give me your credit card and I will get you some money and I will do this, that and the other.’ Now, I had her credit card at the time. If she’d have had it, she’d have given it to him … she thought he was her friend. (P, 18) I think he’s very easy to manipulate. I think he’s had a few friends that have been able to do that, and when he realises that they … even though maybe I have warned him, you know that it’s a bit one-sided this relationship, he feels very, very bitter when the penny finally drops and he realises they have manipulated him. (P, 14) … whereas someone else will think, ‘Mm, that person is a bit dodgy. I won’t walk down this street at night,’ you know, [they] will just steam straight in. (P, 11)
Decision-Making In Everyday Life
There appeared to be two areas of general difficulty in decision-making. First, there were difficulties with thinking through the consequences of actions. This appeared to arise partly due to forgetfulness and distractibility, but also a problem with thinking sequentially about future events. Second, there was a commonly described difficulty with handling numbers, which manifested as struggling to manage day-to-day finances.
Making Decisions Without Thinking Through The Consequences
Parents often described their child’s difficulties in thinking through the consequences of their actions. This affected their children both day-to-day and in the longer-term. For example, at one extreme, more than one parent described their child having made serious false accusations against individuals following moments of anger or stress, seemingly unaware that these would have major repercussions for the accused. Although when the repercussions were made clear, they showed remorse: It was mortifying… I think [they were] horrified too because [they] hadn’t realised until that point what an impact [their] accusations … had. (P, 9) She can’t organise herself. I mean you could typically say, ‘Can you go upstairs and can you do two things?’ and she will get to the top of the stairs and be confused because she can’t sort of … she can’t structure a sequence of events. So, we have to sort of take over some of that responsibility. (P, 12)
Difficulties With ‘Numbers’ Impacting Upon Financial Decisions
Both adoptees and parents highlighted difficulties with handling ‘numbers’ which impacted their ability to manage money: ‘Anything to do with maths, they just faze out, they just can’t do it.’ (P, 2).
Most adoptees recognised that they had in the past needed assistance with managing their finances. One adoptee described this in the following terms: Dealing with bills, dealing with bank details I couldn’t do it on my own without my mum at least explaining it to me, in a way … I just couldn’t deal with all the rent and stuff like that. (YA, 9) … but he’s given the money to me because he wants to, not because I’ve asked for it, but he gives his money to me and then asks for it from me, so I think that’s a way of trying to self-manage. (P, 17) I worry very much as well that … what to do about leaving her money, financially … erm, because she certainly wouldn’t be able to… they would easily get ripped off with anything, you know. (P, 18)
Difficulties Obtaining Help And Support
This third theme referred to a series of issues with accessing appropriate support. More specifically, parents described a general lack of external support and the mixed value of that which was available. This left parents providing the majority of support for their children, despite not feeling adequately qualified. It also resulted in high levels of stress that affected the parents’ wellbeing. Where appropriate support was obtained, e.g., Cognitive Behavioural Therapy (CBT) for depression and medication for ADHD, some positives were highlighted. Participants also described a series of challenges in communicating with professionals and ultimately, disengaging with service providers.
Parents’ Experience Of Strain Due To A Lack Of Appropriate Support
Multiple parents described both a general lack of support and a limited benefit from the support that had been accessed: I don’t think as a family we had enough support. When she was about, erm 15, I can remember going to social services and saying that I really couldn’t cope anymore … I was really asking for some help. And er, there wasn’t any available really. The only help that we had was that we were going to CAMHS [Child and adolescent mental health services], the hospital, erm and we’d been going there for years and nothing good had come from that at all really. (P, 18) We’ve lurched from one crisis to another really, which has put … a terrible strain on me. (P, 11).
Another said that: I’ve realised that I’ve done way too much and that’s not been a good thing because it got to the stage where I finally held my hands up and said, ‘I can’t cope anymore’ and ‘I’m not a professional. I can’t cope with the help that they need.’ (P, 18) … to the extent that a lot of members of my family were worried about my health then, and everybody started saying, ‘You’ve done everything you can. You need to think of yourself now.’ But that’s very hard to do because she’s got so many difficulties, so many problems, and despite all of that she is a lovely girl and it’s a shame. So, you know, what do you do? (P, 18)
Problems Communicating Needs To Service Providers
Both adoptees and parents reported that they had great difficulty in communicating needs to professional services. This took two forms. First, parents described general communication difficulties: At the end of it, you know, he was asking her questions and she just couldn’t understand what he was talking about, and he really didn’t know what to say, didn’t know what to do [and] she didn’t understand what it meant and was frightened what they would do with her, so said no. (P, 9) I don’t take support very well. I try and deal with it myself because I feel ashamed that people have to deal with my problems. (YA, 11)
As a result, parents often expressed frustration at their lack of ability to advocate for their children. At the same time, they felt that they could offer valuable advice to professionals but were often excluded from consultations as adoptees became adults: I’ve written lists of the kind of behaviour that they display when they have gone to certain meetings. I’ve got frustrated when the number of times people say, ‘I can’t talk to you because they are over 16. I’ve got to talk to your child.’ (P, 10)
Deprivation-Related Problems Overlooked Or Misunderstood
Many parents described how their child’s complex needs frequently did not map clearly onto established diagnostic criteria and how this presented a further barrier to receiving help: [They were] struggling a little bit at this and a little bit at that and you can’t quite label him because he hasn’t quite got total dyslexia, he hasn’t got this and he’s not quite something else, so therefore he doesn’t fall in the right categories. But if you look at him globally, there’s a person there struggling, and struggling every day, who isn’t being helped. (P, 17) We tried to get an assessment from social services, but yeah, their answer was he didn’t [get] any support because his IQ is too high. But that doesn’t mean to say he can look after himself and he’s got everyday living skills does it? (P, 4) Because she looks ‘normal’ in appearance, they forget that she has problems. And we explained to them, you know, because we had numerous meetings with them, erm, and said if she was a child with Down’s syndrome where it was obvious that there was … you know, some sort of medical condition, you wouldn’t talk to her like this. (P, 9) They look [up] things on the computer…they just absorb any facts that way and they’ve obviously pulled the wool over their [clinicians’] eyes, that they feel that because they have said set phrases they think, ‘Yes, they mean it’, but they [clinicians] don’t spend long enough with them to understand that, ‘No, they don’t!’ (P, 10)
Ambivalence Towards Taking Medication For Adhd
While many parents noted that ADHD medication brought about benefits, some stated that they would have preferred to have been offered alternatives to medication. Some adoptees did not like some of the side effects of certain medications, but it was generally perceived that clinicians had prescribed drugs which helped the functioning of the adoptees, particularly in relation to ADHD: Until they have had their medication in the morning, they are all over the place. (P, 4)
However, another young adult described their medication as having limited impact: ‘And I have medication in place for that but it doesn’t always seem to have the right effect. It doesn’t seem to work fully.’ (YA, 11)
Talking Therapies Had Some Value
Many adoptees in the current sample experienced emotional problems during their early adult years. Given that some felt misunderstood by people, the opportunity to speak with a therapist or counsellor was often highly valued: It’s nice talking to someone that isn’t involved in your thing, just to let it all out. (YA, 13)
In terms of efficacy, a number of the young adults emphasised that while CBT and similar interventions may not have reduced the underlying difficulties, they had nevertheless helped them cope with these challenges more effectively and had improved their mood in general: It has helped me a bit, because it’s like it helps me try and relax more and deal with, challenge sort of these sorts [of problems] a bit more, but there’s still something where I feel like, I don’t know, like it just, I feel like I’m not exactly cured. (YA, 8) She quite enjoyed talking to someone. She enjoyed it but it didn’t seem to have any difference in her behaviour. (P, 12)
Disengagement With Services
While some adoptees emphasised that they had experienced benefits from therapy, other parents noted that their children had difficulty in maintaining their engagement with service support, in the context of a long history of seeking it, with mixed results: We met this really brilliant counsellor, and in actual fact she ended up counselling me for free of charge instead of seeing my child, because my child at that time wouldn’t see her. (P, 18)
Discussion
By adopting a qualitative approach, our findings expand upon the existing literature and give depth to our previous quantitative results from the ERA study (Sonuga-Barke et al., 2017) and importantly, provide a voice to our participants. Findings that reinforce previous work in this area include difficulties with gaining and maintaining employment, a general vulnerability to victimisation, the original adoptive parents being required to continue support and deprivation-related problems often being misunderstood (Luke et al., 2014; Zosky et al., 2005). More novel findings include characterising how these difficulties translate into specific needs, such as the need for help with decision-making, the broad impact of difficulties with mathematics, specific trouble communicating these needs to support providers, as well as highlighting some services that have been perceived to be useful. These are discussed in more detail below.
First, young adult adoptees who have co-occurring neurodevelopmental difficulties resulting from severe deprivation early in life will often need support to become more effective decision-makers. In particular, this study highlights needs with regard to how adoptees (1) organise day-to-day practical matters and handle money, (2) consider future events and outcomes when making decisions, and (3) navigate the issue of their vulnerability to victimisation. More generally, decision-making can be marked by a failure to foresee the consequences of actions, social naivety and a failure to detect others’ harmful intentions. A qualitative approach revealed previously unrecognised problems with numeracy, which were highlighted by both parents and young people. For many of the young adult adoptees, their parents, fully aware of these difficulties, play a key role in managing and organising their children’s lives and finances and providing day-to-day support. Parents can also play a vital safeguarding role, keeping their young adult children safe from exploitation and victimisation. However, there are limits to what support parents were able to provide and parents especially worried about what the future holds when they age and are no longer able to supply this assistance. There appear to be parallels in difficulties with independent living between our sample here and the broader literature on neurodevelopmental disorders in adulthood. Specifically, issues around unemployment and a continuing reliance upon parental support have been documented (e.g., Eaves and Ho, 2008; Howlin et al., 2004; Pelham et al., 2020). Again, there seems to be a parallel with information-processing and problem-solving being highlighted as risk factors (e.g., Tsatsanis, 2005), which was also raised by our participants. However, difficulties with novel situations have also been highlighted as a risk factor in the general literature on neurodevelopmental disorders (Minshew, Meyer and Goldstein, 2002), which our participants did not highlight. There is a literature on interventions in those with neurodevelopmental disorders, such as video-based instructions, that target a breadth of functional living skills and therefore may also be of some value to those with a history of early adversity (Syriopoulou-Delli and Sarri, 2022).
Similarly, our finding that participants reported proneness to victimisation aligns with the literature on neurodevelopmental disorders without a history of early adversity, in that those with ADHD and even more so those with ASD appear to be victimised more frequently relative to their neurotypical peers (Twyman et al., 2010). The finding that social victimisation was perceived more often by parents than the young adults themselves is in keeping with the general literature on neurodevelopmental disorders (van Roekel, Scholte and Didden, 2010). One common risk factor may be social naivety (e.g., Sofronoff, Dark and Stone, 2011) but risk factors in the literature not reported here include heightened emotional response to victimisation acting to reinforce the victimiser’s behaviours (Kloosterman et al., 2014). It should be noted, however, that with a qualitative approach we cannot say that these issues were not present, just that they were not raised by our participants when prompted.
In contrast to what is found in some of the literature relating to issues in childhood among adoptees with a history of adversity, concerns around identity formation, stigma and relationship quality with the adoptive family were not raised as service needs by the adoptees or their families in our sample. These findings, together with previous work which showed a decline in identity issues by age 11 (Beckett et al., 2008) and strong relationships with the adoptive family in adulthood (Sonuga-Barke et al., 2017), suggest that these issues may be less central to that of service needs in adulthood among adoptees in the current cohort than has previously been found.
Second, although adoptees’ experiences with child and adolescent mental health services (CAMHS) had been mixed (with medication and talking therapies sometimes being perceived as valuable), both parents and young people highlighted how difficult it had been to engage with adult care and clinical services. This highlighted the degree to which young adult adoptees need advocates to help them engage with professionals, articulate their clinical and practical needs and difficulties, and navigate clinical and care systems to ensure that they obtain the adult support and treatments they need. Some parents were particularly concerned that since the transition from adolescence to adulthood they were excluded from discussions and not allowed to play a supportive role for their young adult children, despite their wealth of knowledge on their child’s needs. Again, many of these challenges and concerns may be shared by parents of non-adopted adults with ADHD and autism and are recognised in the adoption literature (Luke et al., 2014; Zosky et al., 2005). It is also possible that the challenges experienced by the young adult adoptees in this sample are further compounded by the complexity of their needs arising from their early experience of institutional deprivation.
Third, professionals in adult service provision (e.g., those in primary care and social workers), would benefit from a greater understanding of how early deprivation creates persistent neurodevelopmental problems that impact adoptees’ development and a shift of focus away from an emphasis on early bonding and attachment-related interpretations (Woolgar and Scott, 2014). It is possible that reliance on psychosocial models by service providers occurs for two reasons. First, the neurodevelopmental problems displayed by the young adult adoptees do not map neatly on to current diagnostic concepts, with individuals often showing a complex profile of multiple, often sub-threshold, problems. Second, some clinicians may lack a detailed understanding of how the brain is directly shaped by early adverse experiences during critical periods of development in ways that can persist independently of later enrichment, and generally de-emphasise the role that early adversity may have played in those experiencing neurodevelopmental problems (Kildahl et al., 2020). Parents may be similarly unaware of these issues, which can lead to adoptive parents feeling that they have failed their children when their problems persist despite this largely being outside of their control. This lack of awareness was previously highlighted in the ERA study (Castle et al., 2006), based on interviews conducted over a previous decade. This is despite an abundance of new evidence in this timeframe, including brain-imaging studies demonstrating that the neurodevelopmental problems seen in this cohort are mediated by tangible differences in brain development (e.g., Golm et al., 2020; Mehta et al., 2009). Consequently, there is the potential that with greater awareness and more timely screening for difficulties of this sort, earlier interventions may be able to mitigate at least some of the negative outcomes we describe here.
By adopting a dual informant approach and thereby providing a voice for the young adults themselves, and their parents, some areas of overlap emerged but also some which were most common to one perspective. Areas where parents and young adults appeared to agree included concerns around employment/financial issues and ambivalence towards medication for ADHD. Issues particularly raised by parents were around their child’s vulnerability to being victimised, concerns with their child’s deprivation-related difficulties being overlooked and how the parents themselves were required to provide support. In contrast, the young adults mostly highlighted the positives of the interventions they had received. These findings show up the added value to be gained through allowing for multiple perspectives.
Strengths And Limitations
The study had several strengths. It is the first to explore qualitatively the care needs and service experiences of adult adoptees with complex needs resulting from severe early childhood deprivation. The sample presented here is part of a prospective study with young people with a validated exposure to severe deprivation and detailed assessments of neurodevelopmental problems at multiple points across development. It also explored both adoptee and parental perspectives and insights.
There were three main limitations. First, different types of early adversity often have different developmental outcomes (Debowska et al., 2017) and so it may not be possible to generalise our findings to individuals who have experienced other forms of early adversity. The second limitation was that we cannot generalise the experiences with the support services referred to by our participants (e.g., primary and secondary care, private therapists and social workers) to other forms of service provision (e.g., educators and law enforcement). The third limitation is that it may be difficult to generalise our findings to service provision outside the UK.
Implications
It is unclear how similarly the experiences highlighted here resemble those experienced by idiopathic neurodevelopmental problems. Despite a recent increase in research, less is known about adult ADHD compared with childhood and within that, only a few studies have focused on services experienced. Those that have seem to suggest somewhat different experiences. For instance, Swift and colleagues (2013) describe a primary challenge being a continuation of care and a lack of specialist centres for adult ADHD. The issues raised in our sample appear to relate more closely to obtaining support initially, rather than concerns around whether it will continue.
Nevertheless, there also appear to be similarities. Cadman and colleagues (2012) describe a significant amount of support being provided by parents resulting from unmet needs. Furthermore, Adamou and Bowers (2011) highlight that there is a high level of co-occurrence of neurodevelopmental problems, as is the case in our sample. There also is some suggestion that adults with ADHD and autism may benefit from the involvement of professional coaches who can help them to develop decision-making and life management skills to better organise their lives (Murphy et al., 2010) and may require support from occupational health services/targeted occupational therapy (Golm et al., 2020; Taylor, Fauset and Harpin, 2010). Talking therapies may also play an important role. It is possible that such an approach could benefit young adult adoptees such as those in the current study, by promoting effective independent living skills and reduce the practical burden on adoptive parents, but this would need to be evaluated.
Conclusion
Young adult adoptees who have suffered neurodevelopmental problems from severe early deprivation have a complex range of persistent vulnerabilities and impairments that directly impact the way they organise and manage their everyday lives and relationships. Our analysis highlights the need for clinical and care services to work with these young people and their families to support the former’s successful transition into adulthood by providing appropriate practical interventions. Future research should explore more directly the experiences of those with idiopathic neurodevelopmental problems compared to those who experience them as a result of early adversity.
Supplemental Material
sj-pdf-1-aaf-10.1177_03085759231212497 - Supplemental material for Neurodevelopmental problems in adulthood following severe early deprivation: A qualitative analysis of clinical needs and service user experiences
Supplemental material, sj-pdf-1-aaf-10.1177_03085759231212497 for Neurodevelopmental problems in adulthood following severe early deprivation: A qualitative analysis of clinical needs and service user experiences by Christopher Edwards, Mark Kennedy, Nicky Knights, Hanna Kovshoff, Jana Kreppner, Barbara Maughan and Edmund Sonuga-Barke in Adoption & Fostering
Footnotes
Acknowledgements
We would like to express our sincere gratitude to all the families and young people who have participated in this study over the many years it has been running. Without them this work would not be possible. We would also like to thank Michael Rutter (King’s College, London) for initiating the study, as initial principal investigator (PI) and for his support throughout the project, Robert Kumsta (Ruhr University Bochum) and Wolff Schlotz (Max Planck Institute for Empirical Aesthetics) for their roles as co-PIs and Claire Ballard (King’s College, London) for her support during the most recent phase. Lastly, we would like to thank our funders, the ESRC and the Waterloo Foundation.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Professor Sonuga-Barke reports funding from Shire, Medice, grants from QBTech, personal fees from Neurotech Solutions. All other authors report no conflicts of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funders (The ESRC: ES/I037970/1 and The Waterloo Foundation: 686-4339) had no role in study design, data collection, data analysis, data interpretation, or writing of the report. This paper represents independent research part funded by the NIHR Maudsley Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Supplemental Material
supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.