
Abstract
This qualitative retrospective recall study utilised nine in-depth, semi-structured interviews with adoptive mothers involved with an online support group often used by adoptive parents facing difficulties. The aim was to explore their transition to adoptive motherhood. The study was unusual because it covered a lengthy period, from pre-adoption and the motivation to adopt to 12 months post child placement and used Reflexive Thematic Analysis to analyse the data. Findings include the mothers’ sense of misaligned expectation, uncertainty, powerlessness, isolation, and emotional and physical fatigue. The most prominent findings centred on the high level of mental health issues reported by the mothers which included post-adoption depression, anxiety and trauma. New insights are discussed along with implications for future research and practice, along with the limitations of the study.
Keywords
Introduction: The transition to adoptive parenthood
For adoptive parents, the arrival of a new child is always a time for celebration. But, for some, the transition is challenging as parents adjust to changes in family relationships (Ceballo, et al., 2004; Cowan and Cowan, 2000; McKay, Ross and Goldberg, 2010) and face threats to their mental and physical health (Foli, 2010; Foli, et al., 2017a; McKay, Ross and Goldberg, 2010; Saxbe, Rossin-Slater and Goldenberg, 2018; Senecky, et al., 2009).
During March 2018–2019, 3570 children were placed for adoption in England (Department for Education, 2019). In most cases, this leads to better lives for children and fulfils desires of parenthood for the adopter (Dance and Rushton, 2005; Palacios and Brodzinsky, 2010). However, for some the transition to adoptive parenthood is overwhelming.
The decision to adopt often follows fertility difficulties that may prompt painful reactions and longer-term psychological problems (Bonovitz, 2008). Individuals may continue to struggle with the psychological effects of infertility while engaging with the adoption process, hiding any feelings of loss and grief, in order to appear ‘ready’ for adoption to professionals (Brinich, 1989).
Further pressures are imposed by assessments and panel approvals, uncertainty surrounding child characteristics, lengthy timescales and disputes about parental rights (Cebello, et al., 2004; Levy-Shiff, Bar and Har-Even, 1990; Rushton, 2004; Selwyn, et al., 2006). Some mothers speak of ‘instant parenthood’ (Quinton, et al., 1998) and ‘hitting the ground running’ because on average, newly placed children are three years old and have largely been in care due to neglect and abuse. Many adopters, therefore, underestimate the nature of adoptive parenting and the demands posed by parenting a child with psychological and behavioural difficulties resulting from early trauma (Goldberg, 2009; Rushton and Monck, 2009). Research highlights the protective factors of being older, with more opportunities to develop support and coping mechanisms that better prepare them for parenthood (Ceballo, et al., 2004; Levy-Shiff, Bar and Har-Even, 1990).
Adoptive parent experience
Despite the substantial amount of research into adoption, little is known about the emotional and psychological impact of transitioning to parenthood from the perspective of the adopters (Meakings, et al., 2018; Selwyn, et al., 2006). This is likely to be significant as adoption disruption has been linked to parental factors at time of transition, such as adopters’ unrealistic expectations, idealised view of adopted children, help-seeking behaviour and motivation to adopt (Goldberg, 2009; Palacios, et al., 2019; Randall, 2013; Rushton and Dance, 2004; Selwyn, Wijedasa and Meakings, 2014).
Although the prevalence of adoption breakdown is low, approximately 3% in England and Wales (Selwyn, Wijedasa and Meakings, 2014), this encouraging figure should be seen in the wider context where adoptive parents struggle with their child’s challenging behaviour and poor emotion regulation from the onset of placement (Palacios, at al., 2019; Selwyn, Wijedasa and Meakings, 2014).
These difficulties have been highlighted in several studies from around the world. In the USA, for example, Foli and colleagues (2010, 2017b) explored the prevalence of post-adoption depression and warned that unrealistic expectations of self and others heighten the risk of it developing after child placement (Foli, 2010; Foli, et al., 2017a; Foli, Lim and South, 2017b). The prevalence of post-adoption depression six weeks after child placement is comparable to that of post-partum depression (McKay, Ross and Goldberg, 2010; Senecky, et al., 2009). In Canada, Daniluk and Hurtig-Mitchell (2003) interviewed 39 couples who had adopted a child within the previous two years. Parents found the transition stressful, with three factors contributing to stress: accepting infertility and deciding to adopt; psychologically surviving the uncertainties of the adoption process; and coming ‘full circle’ by adapting to adoptive parenthood.
In the UK, Selwyn and colleagues (2006) conducted a longitudinal study exploring the costs and outcomes of non-infant adoptions, specifically involving children placed at the age of three to 11 years. The authors scrutinised 130 children and carers (both adopters and foster carers) over 11 years, reviewing life changes and financial and emotional costs, as well as outcomes for both child and carers. They highlighted the need for improved post-adoption services, particularly those offering emotional support to adoptive parents/carers. A later UK study by Dance and Farmer (2014) recorded the reflections of 27 adoptive parents as they progressed from application to adoption placement and concurred with others by highlighting the physically draining aspects of the process and the value of connecting with already established adoptive parents as a means of support.
More recently, UK researchers have emphasised the love felt by new adopters towards their child and the success of family adjustment, with expectations being more than met (Adoption UK, 2019; Lewis, 2018; Meakings, et al., 2018; Tasker and Wood, 2016). If problems do arise, they centre around different inter-generational parenting styles, a sense of continued uncertainty in the parental role (Tasker and Wood, 2016) and a lack of authority and support for well-being (Lewis, 2018).
A longer time period has been used in two further studies. The Wales Adoption Study (Meakings, et al., 2018) surveyed 96 adoptive families at four months post-placement and 40 of them at nine months. The findings offered a comprehensive exploration of the support needs of adoptive families, particularly the value of short-term financial help, assistance with securing the adoption order and the need to be informed about the stages of the legal proceedings. A further large study, The Adoption Barometer survey by Adoption UK (2019), captured the experiences of adoptive families across the UK via an online survey of 3500 parents. It showed that half of new adopters found the early months so challenging they wondered if they could continue. Moreover, 54% of parents experienced stress, anxiety or post-adoption depression symptoms during the early weeks. In addition, social isolation thereafter was a continuing concern. Advice from social workers to keep family at a distance deepened this sense of isolation and loneliness.
From this literature review, it can be seen that much of the research on adoption tends to focus on specific events within the transition, such as ‘matching’, ‘introduction’ and support needs, with the emotional and psychological impact on parents discussed as a secondary issue. This study adds to the literature by exploring parents' transition to adoptive parenthood over a lengthy period – from point of decision to adopt through to 12 months post-placement – and pays particular attention to their emotional and psychological well-being.
Methods
Participants
The participants comprised nine white, heterosexual adoptive mothers who used an online support group often used by adoptive parents who are facing difficulties. They had formally adopted 14 children, with one of those adoptions completed at least a year ago. No fathers, members of the LGBTQ+ or BAME community were represented. Inclusion criteria were: sufficient fluency in English, UK residence and adoption in the UK through public, private or international agencies. Eight families had adopted through the local authority and one via a private agency. Eight children were below the age of 24 months when placed, younger than the current average age of around three years in the UK (CoramBAAF, 2019). The remaining six were aged between three and five. In eight of the families, the adopted children’s ethnicity resembled that of their adoptive parents and seven mothers described themselves as married, with one identifying herself as divorced and another single.
Procedure
Ethical approval (University of Sussex Sciences & Technology C-REC, ref ER/CK377/4) was granted prior to recruitment via three local authority adoption agencies and online support groups. Participants were selected on a first-come, first-served basis with consideration given to the number of children and their ages, as well as the presence of birth children in the family, in order to enhance the representation of different family structures. Each participant received an information sheet prior to interview, including details of data management arrangements. If more than one child had been adopted, parents were asked to speak about the most recent.
Genograms
The genograms of the nine families are laid out below (Figure 1).
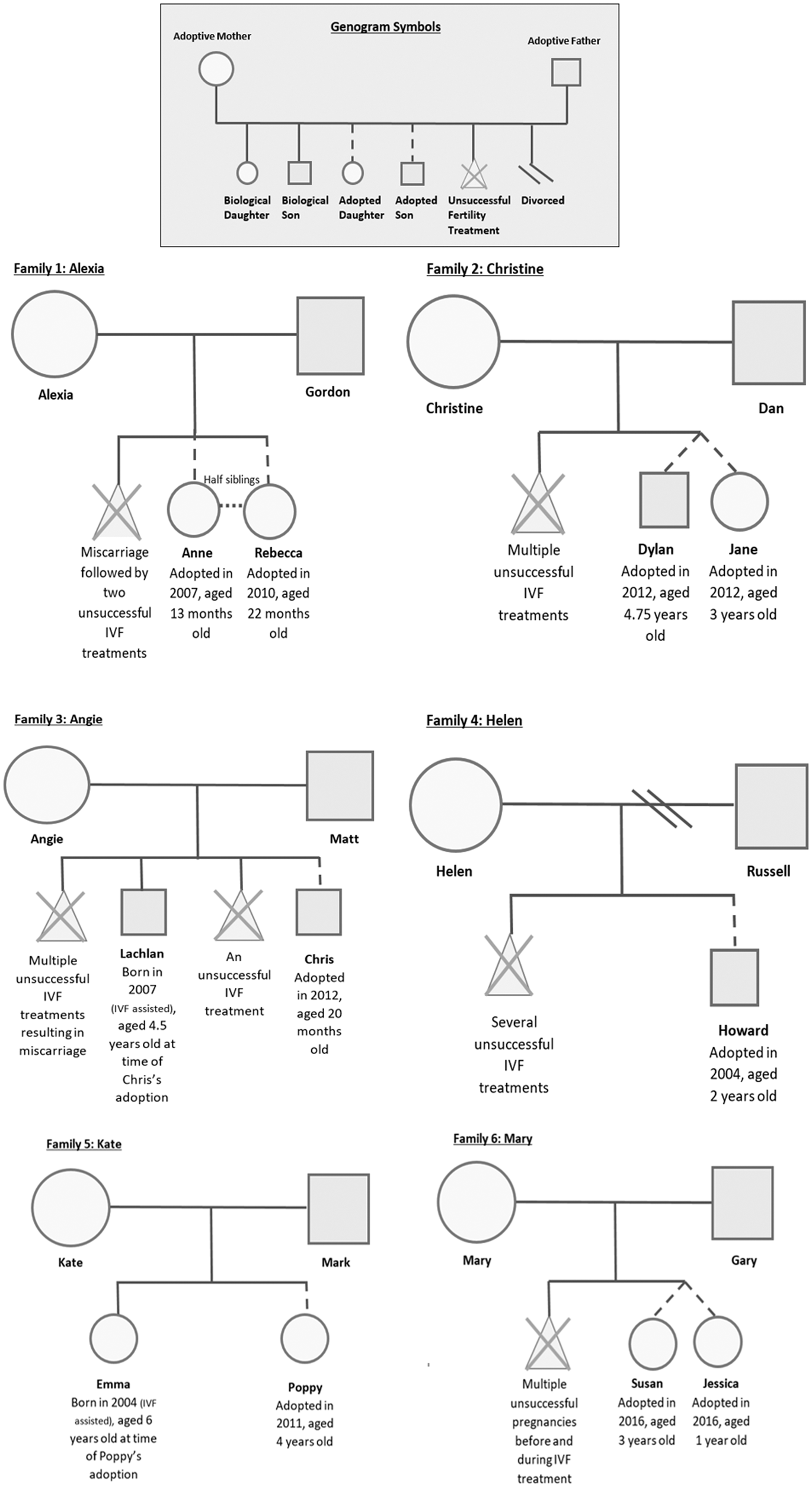
APEx: Participant genograms.
Data collection and analysis
Semi-structured interviews were conducted between April and June 2019. They focused on retrospective and current adopter experiences and how the family had evolved from pre-placement to its current situation. As the focus of the article is on the transition to adoptive motherhood, content relating to this was extricated from the wider interview transcripts. Interviews were recorded and transcribed verbatim and pseudonyms are used for names, locations and identifiable organisations.
Reflexive Thematic Analysis, as described by Braun and Clarke (2006, 2019), was used to analyse the material as it facilitates the identification of themes both within and across data. The analysis followed the RTA method and comprised repeated reading of transcripts, the generation of descriptive and meaning-based codes across the whole dataset, reviewing each transcript and checking against the created themes and refining theme names and definitions. Themes were developed based on the level of impact not only within each individual narrative but also across the individual transition period as well as across the wider group narratives.
Results
Five key themes were identified from the interviews: ‘reality not living up to expectation’; ‘uncertainty and powerlessness’; ‘emotional and physical fatigue’; ‘uniqueness and isolation’; and ‘love, loss and ambivalence’.
These themes were not entirely independent but in the following discussion the significance of each of them for well-being is dealt with separately. References made to adopters’ psychological well-being reflect their own descriptions of their emotional states and have not been clinically validated.
Reality not living up to expectation
For eight of the nine mothers, expectations about what adopting a child would be like, how the process would unfold and how the family would function differed from the reality of their experiences. They reported an optimistic, somewhat fantasised view of parenthood and ‘glossed over’ the hurdles they needed to overcome. For those seeking to adopt a second child, familiarity with the process reduced this lack of realism and boosted their confidence. In Kate’s words: I just assumed I’d be having a four-year-old child. I had a six-year-old and had she been four, I'd have known what four-year-olds entailed. I always thought that’s what I could be getting … I just thought as soon as that child comes through to me, she’s going to be the most fabulous girl, fabulous boy, whatever, and they’ll merge straight into my family and it’s going to be great.
But such expectations neglected factors like uncertainty about the adoption process, the child’s past experiences and the special demands of parenting a child from care. For all but one mother, there was a discrepancy between the child they expected and his or her presentation once in the family: the child profile and information provided by those who knew the child, such as social workers and foster carers, did not mirror the individual they were seeing and parenting. To quote Angie:
We were quite dreamy about it … I assumed I’d be okay. The reality was that I wasn’t … I had a child who I didn’t know what he wanted, I didn’t know what he needed because all the things I was told he needed he didn’t want anymore, and so there was this major breakdown in communication … I felt all I said to him was ‘no’, he screamed, I said ‘no’ and he screamed and attached himself to me so I felt physically – I just couldn’t breathe. I went on anxiety medication within six weeks of Chris moving into the home.
Other mothers spoke of ‘rose-tinted’ expectations with reality being ‘completely different from what they envisaged’ and ‘not within the realms of normal parenting’. The experience of delayed or regressive behaviour, child hostility or violence and challenges to parent–child attachment were unforeseen aspects of their adoption journey.
Interviewees who expressed the most distress were mothers whose prior expectations were mostly unmet and whose high level of uncertainty endured beyond child placement. One summarised her experience as feeling ‘completely unprepared for the intensity’ of her child’s behaviour, often struggling to relate and bond with one child while ‘surviving’ the often dysregulated, aggressive and violent behaviour of the other. To quote Angie again: It was horrendous … I felt claustrophobic and wanted to escape most of the time … I was desperate for anybody else to be in the house, so I didn’t have to manage this on my own … I didn’t feel safe often … I had been through a trauma.
In contrast, two mothers did not experience large discrepancies between expectations and reality and did not report great emotional distress. On referring to a friend who had adopted, Tracey stated:
[They had] quite a horrendous experience, but I was obviously looking on at this time quite closely thinking, ‘Oh, do we really want to do this?’ … but actually having that knowledge was really useful because we saw the kind of, I wouldn’t say the worst-case scenario because it isn’t the worst-case scenario, those children are now grown up and you know, doing okay so … but they did have a really tough time in the beginning, so we kind of went into it with our eyes open … quite aware that you know, it might not be … an easy journey.
So, to summarise, the analysis of this theme showed variation in the contrast between mothers’ expectation and reality and that those for whom the gap was smallest reported less emotional distress throughout the transition period.
Uncertainty and powerlessness
Feelings of uncertainty and powerlessness were frequently expressed in the interviews, particularly about the length of the process and perceptions of authority within child selection and eventual adoption approval. Angie highlighted these features in her complaint about the process timeframe and her lack of power to influence it: You find a child, oh no you haven’t, we’re going to go to matching panel, or no we’re not. There are just so many variables. At least with pregnancy you know you are going to have a baby at the end of it and it’ll be around this date. But in adoption you can’t even put a date on it … you just don’t know when to get excited.
Immediately after panel our social worker had some children for us that we wanted to adopt immediately, and we thought ‘Oh, nailing this’. It was a sibling pair, a boy and a girl, who were five and three at the time. Um, and they liked us, and it was all progressing, and everybody was very happy, and we decided – because it was all going along and they were talking about when the children were going to move – we decided to have a pre-child holiday. And on the Friday, they told us they needed me to try and find a school for the boy to start in September and on the Monday, they phoned us to say it was off, that was it, they weren’t going to proceed with us. And we had been involved in the match for about three months. The social worker told us to buy beds, we bought beds and bought bedding.
Interviewer: Did they tell you why?
Yes, well another social worker looked into the paper and – I don’t know why this happened because none of this is in the paperwork, but she got out of my paperwork that I was very mentally fragile and couldn’t go to the shops by myself … . But it doesn’t say that in any of my paperwork … I had a full-time job … we had spent three months falling in love with these children and making plans and … [we were] absolutely devastated, unbelievably devastated. We fought it as much as we could, but they wouldn’t change their mind even though they were happy to admit that basically it was a big lie.
Mary’s experience reflects the power imbalance experienced by all the mothers throughout the process. This was also evident after placement when birth parents contested the adoption, leaving one mother to say, ‘We had no idea that might be a possibility.’ The powerlessness and uncertainty mothers felt reflects the realities of the situation, namely that children's services and/or birth parents remain very powerful.
Emotional and physical fatigue
All the mothers spoke of emotional and physical fatigue throughout the adoptive process. For seven of them, the toll of fertility treatment was a precursor to their decision to adopt. Interestingly, fatigue was not reported during the assessment and matching stages, but more once approval had been granted and the parent and child were united in a phase called ‘introductions’. In Kate’s words:
I was tired. The transition period was over two weeks and Poppy was over in [location] and I had to be over there for like 7:30am. You can’t get there for then because the traffic was crazy, and I had a child already … yeah, I was stuck in the foster carer’s house, I felt like a spare part and I felt really uncomfortable … it was very difficult. … I just couldn’t envisage how traumatic that would be for us … I was having to leave earlier and earlier, and I wasn’t seeing Emma in the morning. And she was going to school and missing me … it was tiring. So exhausting.
While the emotional intensity of this period produced mixed feelings among the mothers, physical demands were reported by all. The adherence to statutory requirements meant that they lacked sleep and a lot of travel was involved, often with early starts and late finishes. Days were spent in unfamiliar locations while attempting to bond with an unfamiliar child. This was Helen’s experience: As soon as I saw him, I wanted him to be my baby … but he has gone from his foster home to being with me, he didn’t sleep, I can’t tell you how tired I was. I went to bed at 4.30 in the afternoon, I cried at going to bed at 4.30pm but he was asleep, so I was going to go to sleep. He hardly slept; I couldn’t leave him for any period of time … I couldn’t return to work.
It was all just so overwhelming and from the beginning of introductions, Susan was very rejecting of me and didn’t want to particularly be near me or do anything with me… There was a lot of violence between them … Susan had always had more challenging behaviours than her sister, so a lot of her violence was towards me … [there] wasn’t a fable honeymoon period that people talk … she was very verbal from the off but the violence towards me started very quickly … It was a total surprise. There was nothing in their paperwork.
For these mothers, the behaviour and characteristics of their newly placed child were unexpected and their frustration was exacerbated by the fact that statutory bodies continued to maintain a parental responsibility during this time, and monitor the situation to assess the progress of the placement. Under such pressure, mothers hid their distress, fearing the child would be removed if they acknowledged their difficulties, a response that could only further increase their physical emotional exhaustion.
Uniqueness, difference and isolation
For seven mothers, the adoption process was new to them and those around them. Uncertainty about the process, along with recollections of previous pregnancy complications, led them to withhold information about the decision to adopt or the progress of the application from others. This was Sarah’s experience:
I went on adoption leave and that’s the other odd thing because we’d kept it private… a lot of people were surprised, and I only gave something like a week or 10 days’ notice to work that I’d be leaving and going on leave. Unless you choose to tell people… which we didn’t…there wasn’t any notice for people of what you are going to be doing. You don’t have that lead-up with getting to know other mums and things. You’re just suddenly there with two kids. But in the village, there were some parent and toddler groups, so I joined those but it’s a different starting point. To suddenly go in and everybody talks about births and pregnancies and things, so you’d feel a bit alienated I think at the beginning.
Every mother spoke of the unique position of beginning their parenting journey with a child who had started his or her life within another family and the sense of ‘missing information’ about them. The task of looking after a child while developing a meaningful mother–child relationship recognisable both within the family and the wider community was a challenge.
All but one of them spoke of the time commitment of appointments and continued monitoring by statutory services post-placement. To quote Helen:
All of a sudden I’d gone from being at work and having a friendship group and a really great social life, to being at home with a two-year-old who I didn’t really know, and also we had social services visiting, his social worker, our social worker, we had review meetings, he had a guardian because the birth father was challenging the adoption. A guardian was appointed who had to be a visitor as well; I had a health visitor, I had a play worker, a paediatrician. So, every week there was at least two official meetings for him, where I was expected to keep him quiet and occupied and take part in a meeting.
At a time when most new biological mothers are given space to recover, bond and lean on family for support, adoptive mothers continue to be assessed and monitored. Access to tailored support appeared non-existent in the majority of cases and in all the adoptions physical contact with family and friends was discouraged in the initial weeks. This was Kate’s experience:
I was a bit stuck really because, like when I had Emma my parents came over, my mother-in-law and father-in-law all came over, they brought food with them, I didn’t have to do anything, I was really looked after. But when I had Poppy, I couldn’t allow any family to come, the bonding is really important, but I needed my family, I needed my mum to cook me a meal. It was really exhausting [cry], sorry I don’t mean to cry… but I was tired.
Many mothers struggled with the lack of personal contact with close family, suggesting they needed hands-on support to help manage day-to-day tasks. However, they complied with instructions from social workers to delay or avoid such contact in order to promote positive attachment. Knowing whom to share information with, how much to share and when proved to be a challenge throughout the transition period and beyond.
Across the narratives there was a sense of isolation from other new mothers and a lack of the understanding and support afforded to biological mothers. They reported a pressure to be seen to cope, be ‘perfect’ or a ‘wonder woman’. To quote Kate again:
I just felt no one really saw it from my point of view, have any concept of how it could feel for me. And actually, not long after that my friend had a baby and she was diagnosed with post-natal depression and everyone supported her through that … but for me there is actually no one there for you. You’re discouraged from seeing anybody or meeting anybody. It’s about you and the child and the bond. Oh my goodness, you need to have a break!
Feelings of isolation, difference and fear were shared by the six mothers who struggled the most, one commenting, ‘I wish I’d been told that it’s okay not to be okay.’ They wanted social workers to provide reassurance that if they felt they were not coping very well, they could admit it and be told, ‘It’s fine and your child won’t be taken away.’ Six mothers also felt isolated by their friends and by their family’s misunderstanding and ignorance about their situation. In Angie’s words: [T]he first six or nine months were horrendous, and there was almost the feeling of ‘Well, you wanted this, now you have to get on with it’ or ‘you know, it’s just a tantrum and you just put him in his bedroom’, and no you don’t. When you are faced with that complete lack of understanding it’s easier to just say everything is fine because it’s too emotionally difficult to try and explain it to somebody and then still not receive the support you need from them. This is when we shut down a little really.
Loss, love and ambivalence
The theme of loss, love and ambivalence captures the evolving nature of relationships during the adoptive parent journey. Like most adopters around the world (Schmidt, 2010), all nine mothers had attempted to become biological parents. Most had experienced unsuccessful fertility treatments before considering adoption as a means of creating a family life.
These experiences left many with a strong sense of loss concerning life expectation and control of life choices, a prolonged sense of stress associated with a risk of developing mental health symptoms linked to anxiety and depression (Schmidt, 2010; Verhaak, et al., 2007). Interestingly, only two mothers referred explicitly to the emotional impact of this loss and in both instances, it endured, even post-adoption. For Molly: ‘I don’t dwell on it but sometimes something will come out of nowhere, like on the telly, you know like a scan and it’ll make me go [physically retract and sigh].’
More common was reference to the physical and/or financial toll of fertility treatment. Each mother began her adoption story by referencing her fertility or infertility status, perhaps suggesting that this loss is an important aspect not only related to her motivation to adopt but also her identity as an adoptive mother.
Another loss which seemed apparent to the researcher but was not explicitly acknowledged by most of the mothers was that associated with the fantasised child. Each mother held strong views of either what their adoptive child would be like or how their post-adoption family would function. In all but one case, these expectations or fantasies were not realised and a loss of the ‘idealised child’ was experienced (Hugger, 2009).
Despite stems of affection developing throughout initial meetings, the challenges of day-to-day life and the need to abandon previously held fantasies resulted in mothers finding it difficult to bond and attune to their child. For four of them, the first year after placement was filled with ambivalence. Angie again: [At the beginning] I’d given him my heart … I felt there was a connection … [but when he was placed] there was a major communication breakdown … I’d go into survival mode … love was gradual.
While loss and ambivalence touched each mother’s story in some way, love was threaded throughout: love held for the fantasised child, love at first sight for the real child and/or the development of love over time. Despite the challenges throughout the process, five mothers experienced a positive connection – a love, a sense of togetherness with their new child.
Alexia: Once I’d met Anne … I just got tunnel vision. It was like, right … I need to look after this little baby, and that is what I’m gonna do, and I couldn’t really give a toss about those other things or the class I left behind, you know. It was amazing how focused my brain was and I thought, ‘This must be what happens when you have a baby!’ … that was a strange feeling and actually quite brilliant.
Others also felt ‘instant’ and ‘powerful’ connections, describing a sense of belonging and ownership: ‘He is mine.’ Perhaps it was the feeling of having ‘a lot of love to give’ and belief – ‘I was meant to be a mother’ – that motivated mothers throughout the adoption process. But for some, the reward came from an immediate strong connection, a love at first sight, leading Alexia to experience a type of Winnicottian ‘maternal preoccupation’ (Holloway, 2012) more commonly associated with biological motherhood.
These extracts encapsulate the complexities and transient nature of relationships during this transitional period. Adoptive mothers explicitly or implicitly referred to the desire to develop a connection with their new child/ren, while perhaps overlooking the child’s own sense of mourning or loss connected to the adoption. Their narratives depict a transitional experience shaped by unanticipated challenges, a sense of uncertainty and powerlessness and lack of parental autonomy, leading many to suffer distress and poor mental health in what should be a primarily joyful life change.
Discussion
As the emotional distress associated with the adoption process has been somewhat neglected as a prime focus in past research, the mothers’ experiences captured in this study provide new insights into its effects.
The first is that only a minority of mothers recalled a completely free transition, attaching to their new child with ease and adjusting physically and emotionally to the life change. Instead, they described turbulence, often feeling unprepared to deal with their child’s challenging behaviour, powerless to plan or control events within their own family, isolated from their surrounding support networks and different from new biological mothers. Despite this, mothers showed remarkable ability to overcome such difficulties and express love towards their child (Brinich, 1989; Brodzinsky, 1987; Brodzinsky and Huffman, 1988; Selwyn, Wijedasa and Meakings, 2014).
While these findings concur with those of other studies, they provide new insights into the emotional and psychological state of new adoptive mothers. For example, while Lewis (2018) and Tasker and Wood (2016) found high levels of physical tiredness due to pre-placement processes, our findings emphasise the emotional fatigue felt on top of physical tiredness, suggesting that mothers found themselves in a state of emotional and physical exhaustion well before starting the task of parenting an unfamiliar child. Moreover, those who reported high levels of emotional and physical fatigue at the time of child placement also expressed high levels of anxiety, depression and/or trauma.
A further important finding is the emotional and psychological impact of the process on mothers, particularly the escalation of self-reported mental health issues among those caring for a behaviourally challenging child or with poor support networks, both compounded by misalignment of expectation. Several studies have indicated anxiety or depression among adoptive parents throughout transition, but the findings from this study suggest that levels of negative mental health may be higher than previously reported and persist long after the settling-in period.
All new parents experience a certain amount of anxiety, stressors and sense of unpreparedness (Ceballo, et al., 2004; Cowan and Cowan, 2000; Harris-Waller, Granger and Gurney-Smith, 2016; Levy-Shiff, Bar and Har-Even, 1990) so it might well be asked what is special about adoptive parents? Our findings suggest that they face the additional challenges like those described earlier, making them more vulnerable to stress and negative emotional states (Daniluk and Hurtig-Mitchell, 2003; Harris-Waller, Granger and Gurney-Smith, 2016; Schmidt, 2010; Schoemaker et al., 2020) and that these pressures are greater the older the child at the time of adoption.
Limitations
There are several limitations to this study that restrict wider application of the findings. All participants were members of an online support group, often used by parents who are having difficulties within their adoptive family, so their experiences may have been unduly negative. Second, the sample is small and comprised nine heterosexual white mothers. The experiences of fathers, members of the LGBTQ+ community, or people with non-white ethnicities were not included. Fourth, adoption practices differ across geographical areas and vary over time. These might have affected the waiting times, access to financial support and post-adoption interventions experienced by the mothers in the past. Fifth, one factor possibly affecting the study was the length of time from transition to parenthood – from three to 15 years – and the accuracy of memory recall over such a long period. Sixth, the interviewer’s own status as an adoptive mother was made known to interviewees and this may have created a more open environment, facilitating fuller disclosure of negative emotional experiences. Finally, Reflexive TA was used for the analysis and the strengths and weaknesses of this method in highlighting some factors at the expense of others must be considered,
Future research
Suggestions for further research emerging from the study include: replication using larger and more representative samples; the inclusion of potentially significant factors, such as quality and satisfaction with the partner relationship, the psychological impact of infertility and parents’ levels of knowledge and understanding of their child’s characteristics; investigation into the prevalence and nature of post-adoption depression, anxiety and secondary trauma among adoptive parents; and a review of the timing and content of pre-adoption training.
Implications for practice
Four implications for practice are indicated by the study. First, it is helpful for those working with adoptive parents to understand the high level of physical and emotional exhaustion parents feel when completing the adoption process itself, let alone meeting their new child for the first time. Slowing down or extending the introduction phase could provide parents with time to replenish emotional and physical reserves, become more in tune with idiosyncratic characteristics of the child and provide space for them to discuss and manage unexpected challenges. Similar proposals have been made previously but statutory process remains unchanged. Second, in response to adopters’ high levels of emotional distress and feelings of unpreparedness for the parenting task ahead, provision of psychological interventions targeting the parents themselves may be warranted. Parent-focused and clinically informed interventions delivered at the time of child placement are likely to be especially effective. Third, along with ‘specialist interventions’, it is worth developing a general service focus on both child and adult well-being. If the focus is dominated by child adjustment to the exclusion of adopter responses, parents may feel unsure of the legitimacy of their own emotional health concerns. Fourth, because mothers report a need for face-to-face support from close family at the time of placement, it may be beneficial to review the advice given to keep friends and family at a distance during early placement as this can isolate adopters and exclude supporters – risking further adjustment problems.
Conclusions
This study reports the findings of nine interviews with adoptive mothers, exploring their transition to adoptive motherhood. The most significant findings reveal reports of severe and enduring psychological distress throughout the transition period, with self-reports of high anxiety, post-adoption depression and ‘trauma’, as well as emotional and physical fatigue.
The demands of their children’s needs and subsequent parenting tasks mean that families facing the most challenging child behaviour often feel the most isolated, separate from other parents and misunderstood by wider support networks. Although it is important not to pathologise mothers based on their reported levels of distress, and bear in mind the limitations of the study, it is nevertheless just as important to recognise that for most of these mothers their transition into adoptive motherhood was marked by risks of mental health problems which clearly warrant attention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.