
Abstract
This study explored how child maltreatment, alongside a range of other variables, predicted adverse outcomes for children adopted from the foster care system in England. The participants were 319 adoptive parents who completed an in-depth online survey about their most recently adopted child. The mean age of children at placement for adoption was 28 months (range 0–11 years) and their ages at the time of the survey ranged from 0 years to 17 years (mean = 7 years). Detailed information was collected about children’s backgrounds, including their experiences in the birth family and the care system before adoption. Adoptive parents also reported on how well children were getting on in a range of areas of functioning and how well they felt the adoption was going overall. Child maltreatment and child adverse outcomes were modeled as two factors in a latent factor structural equation model. The relationship between these two factors was explored alongside a range of covariates. Associated with worse outcomes for children were potentially heritable factors (parental learning disability), the pre-birth environment (exposure to drugs or alcohol in utero) and the period between birth and moving to the adoptive family (higher levels of maltreatment, spending more than a year in care, having two or more foster placements). The child’s distress on moving from the foster home to the adoptive family was also highly significant in linking to poorer outcomes, suggesting the detrimental effect of poorly managed transitions. Implications for child welfare practices before and after adoption are discussed.
Introduction
This study focuses on children adopted from care, a form of adoption used in the United Kingdom and several other jurisdictions including the U.S., Spain, Portugal, France, New South Wales, and Canada (Fenton-Glynn, 2016; Palacios, Adrohar, et al., 2019; Thoburn, 2010). The goal of such adoption is to provide legal, residential, and psychological permanence for children who cannot remain within their birth family (Brodzinsky & Smith, 2019). In an extensive overview, Palacios, Adrohar, et al. (2019) argue that when ethical and legal standards are properly adhered to, adoption “may be one of the best alternatives for children who need a family life” (p. 32). For children who have experienced adversity, adoption can be an “effective intervention,” providing opportunities for developmental recovery (Van IJzendoorn & Juffer, 2006, p. 1240). In England, where this study took place, the average age of children adopted from care when their adoption was legally finalized was 3 years and 1 month in 2018/2019 (Department for Education [DfE], 2019). The majority of such children are likely to have experienced abuse and/or neglect, as well as other adverse childhood experiences, prior to adoption (DfE, 2019; Selwyn et al., 2014; Tregeagle et al., 2019; Turney & Wildeman, 2017). Children’s developmental outcomes can vary widely (Grotevant & McDermott, 2014) and it is important that adoptive parents have realistic expectations about children they are adopting (Moyer & Goldberg, 2017). The Adoption and Children Act 2002 in England requires agencies to make an adoption support plan prior to the child’s adoption. Anticipating children’s support needs requires a good understanding of the impact of risk factors on children’s development, and this knowledge is vital for professionals and prospective adopters.
The outcomes of adoption for children in care
The majority of adoptions provide residential permanence for children, although measuring the incidence of adoption “breakdown” is dogged by problems of terminology and methodology (Palacios, Rolock, et al., 2019). The rate of post-order adoption breakdown in England over a 12-year period has been estimated to be 3.2% (Selwyn et al., 2014). While adoptions that breakdown may be a small minority, a wider proportion of adoptive families where children are adopted from care will experience persistent challenges (Thomas, 2013). For example, while one third of adoptive parents surveyed by Selwyn et al. (2014) reported that their child’s adoption was going well, another third said they experienced “highs and lows,” a quarter said they had major challenges, and 9% reported the adoption to have disrupted. A recent survey of over 2,638 adoptive parents in the United Kingdom used similar rating categories. Under half of these parents (41%) reported the adoption to be going “really well,” 38% said they had significant challenges but were managing, 18% faced severe challenges, and 3% reported a disruption (Adoption UK, 2019).
Children adopted from care seem particularly at risk of experiencing emotional, behavioral, and mental health problems (Adoption UK, 2019; Anthony et al., 2019; DeJong et al., 2016; Simmel, Barth, & Brooks, 2007; Tarren-Sweeney, 2017; Tarren-Sweeney & Hazell, 2006). Adopted children can have difficulties in attachment relationships with their adoptive parents and in relating to peers (Hodges et al., 2005; Román et al., 2012; Rushton & Dance, 2006; Van den Dries et al., 2009). In terms of their physical development, adopted children often show good recovery from initial developmental delays for example with weight and height (Palacios, Roman & Camacho, 2010; Van Izendoorn & Juffer, 2006), but in the longer term early adversities may carry risks for cardiometabolic disorders (Baldwin & Danese, 2019). The foster care population, and by extension adopted children, are at high risk of fetal alcohol spectrum disorders (FASDs) (Astley et al., 2002; Chasnoff et al., 2015; Gregory et al., 2015).
The impact of maltreatment and other factors affecting adopted children’s development and adoptive family stability
The origin of adverse outcomes for adopted children may relate to a range of different factors located within the child and their life history, birth and adoptive family factors and service factors (Palacios, Rolock et al., 2019).
Age at placement and child maltreatment
Age at placement has often been studied, with older children found to be at greater risk of later problems (Barth & Berry, 1988). However, age may be predominantly a proxy for length of exposure to adverse experiences and may be less influential per se than these other adversities (Howe, 1998; Palacios, Rolock et al., 2019; Rutter, 2005). Children who are adopted at older ages may have had greater exposure to abuse and neglect, and such maltreatment can have far-reaching developmental consequences (Egeland et al., 1983; Rutter, 2005). Childhood maltreatment has been linked to a broad variety of neurological, behavioral, emotional, health, and cognitive difficulties in looked after and adopted children (DeJong et al., 2016; Hornfeck et al., 2019; Rushton & Dance, 2006; Tarren-Sweeney, 2017). The preferential rejection of one child in a sibling group is a further risk factor for some adoptees (Dance et al., 2002; Rushton & Dance, 2006).
Pre-birth risks
Risks from maltreatment interact with genetic inheritance and pre-birth risks (Howe, 1998). Genetic risk factors include parent mental health problems (such as schizophrenia and affective disorders) and intellectual disabilities (Cadoret, 1990; Ingraham & Kety, 2000; Smoller & Finn, 2003; Vissers et al., 2016). Exposure to alcohol, opioids, and other drugs in utero has been linked to neurobehavioral deficits in babies and children (Bandstra et al., 2010; Moe, 2002). It can be difficult to determine the precise influence of various factors due to the complex interplay of genetic, pre-birth, and post-birth factors (Rutter, 2005). For example, De Bellis et al. (2001) found that parents/caregivers of maltreated children had significantly higher incidences of alcohol and/or substance abuse, and greater incidences of mental health problems, thus their children may be exposed to in utero harm, genetic risks, and maltreatment. This illustrates the overlapping nature of risks that adopted children often experience, and hence the need for research designs that can account for this complexity.
Risks encountered in care
Adopted children in England spend an average of 23 months in the foster care system before moving to their adoptive family (DfE, 2019). This time can provide opportunities for children’s recovery to begin, but additional moves, extended stays in care and poor quality foster care, can all pose further risks (Biehal, 2014; Meakings & Selwyn, 2016; Rolock et al., 2019; Simmel, Brooks, et al., 2001; Ward, 2009). In England, most children are adopted by matched new families, so they experience separation from temporary foster carers, often at a very sensitive age. This can be very distressing for very young children and those placed at older ages (Thomas et al., 1999; Yarrow & Goodwin, 1973). The transition from foster to adoptive home is typically made over a short time period in England (7–14 days). The difficulties for children in separating from foster carers can be a “blind spot” for adults focused on their own anxieties, and children’s feelings and needs can be sidelined (Boswell & Cudmore, 2017). Transitions considered by adoptive parents to be badly handled have been found to be associated with later adoption disruptions (Selwyn et al., 2014).
Adoptive family factors and the child’s increasing age
In terms of adoptive family structure, single parent adoption does not appear to pose additional risks, and for some children may be advantageous (Brodzinsky & Pinderhughes, 2005; Tan & Baggerly, 2009). However, social workers may still hold views about married couples being “ideal” adopters (Farmer & Dance, 2015). Family process variables such as parents’ motivation and expectations regarding adoption, the stability of couple relationships, parental warmth, and parenting abilities (including adoption communication openness) may all impact on outcomes (Anthony et al., 2019; Brodzinsky, 2005; Grotevant & McDermott, 2014; Palacios, Rolock, et al., 2019).
Adopted children can show good developmental catch-up over time (Van Ijzendoorn & Juffer, 2006) which would suggest that longer time in the adoptive family would be associated with better outcomes. However, adolescence often heralds an increase in emotional and behavioral difficulties for adoptees (Brodzinsky, 2011; Neil et al., 2015; Sonuga-Barke et al., 2017), and the majority of post-order disruptions occur in adolescence (Selwyn et al., 2014). Stability, improvement, or deterioration in mental health over time are all possible outcomes (Tarren-Sweeney, 2017); hence, it is unclear whether length of time in the adoptive family (which will correlate with the increasing age of the child) acts as a risk or protective factor.
The current study
Untangling the relative effects of different adversities on children’s development is challenging because of the complex and overlapping nature of risk factors. Few studies of children adopted from care have had large enough samples to manage this complexity and hence identify the independent contributions of correlated risk factors. This study aimed to address this gap in the research through using in-depth survey data from a sample of 319 adoptive parents to explore links between children’s pre-adoption experiences (in utero, at home with their birth family and in foster care) and their progress in the adoptive home (across a range of domains) using a latent factor structural equation approach. Child maltreatment and children’s outcomes are multidimensional concepts so we modeled them as two factors in a latent factor structural equation model. This approach allows researchers to test the validity of hypotheses about both measurement and structural relationships simultaneously and within a single framework (MacCallum & Austin, 2000). It is suitable for dealing with multicollinearity (where many covariates of interest are highly correlated) which can potentially create problems in interpreting findings. It also recognizes that constructs such as child maltreatment and outcomes cannot be observed directly in surveys but must be constructed or inferred from a set of answers to survey questions. It recognizes that the survey indicators are also prone to measurement errors resulting from their self-reporting nature, such as differing interpretations of the questions based on respondents’ experiences, attitudes, and knowledge.
The four key components of the model we employed are the two latent constructs (children’s experiences of maltreatment; children’s adverse outcomes) and two sets of mediating factors (factors influencing maltreatment such as length of time at home, parental pathology; factors influencing adverse outcomes such as length of time in the adoptive family, adoptive family structure). Our hypotheses were that (1) that higher values on the maltreatment index would be associated with more adverse outcomes, (2) values on the maltreatment index would be greater for children who stayed in the home environment longer, whose birth parent(s) had learning difficulties, mental health problems, and/or substance misuse problems, and (3) a range of other covariates would also impact children’s outcomes independent of their experiences of maltreatment.
Methodology
Participants
The participants were 319 adoptive parents who completed an in-depth online survey in 2016–2017 (See Neil, Young & Hartley, 2018 for full details of the survey). They were recruited through 21 adoption agencies in one region of England. Respondents indicated their consent to participate by completing and submitting the survey. The study received ethical approval from The University of East Anglia, School of Social Work Research Ethics committee.
Eighty-five percent (n = 268) were mothers and 15% (n = 48) fathers. A minority (17%, n = 53) were from single parent households. Three-quarters (n = 238, 76%) were part of a heterosexual couple and 7% (n = 22) part of a gay or lesbian couple. The majority of adoptive parents (n = 217, 93%) were White British or Irish. Most (88%, n = 281) had adopted a child previously unknown to them; two parents knew their child from their professional or family network and 36 (11%) were foster carer adopters.
One parent per family completed the survey about one child (their most recently adopted child, or the oldest of siblings placed together). Children were aged 0–17 at the time of the survey, the average age being 7. Age at placement ranged from 0 years to 11 years (mean = 28 months). Just over half (53%) were boys and 47% were girls; 89% were White (British, Irish, or “other”) and 8% were from Black and ethnic minority groups.
Measures
Indicators of maltreatment
There were six questions about pre-adoption abuse (physical abuse, emotional/psychological abuse, sexual abuse involving contact, sexual abuse not involving contact, witness to domestic violence, singled out for rejection) and five about neglect (medical neglect, nutritional neglect, emotional neglect, physical neglect, supervisory neglect). In completing this section (and other questions about the child’s history pre-adoption), adoptive parents were likely to have drawn on a range of sources including the child’s permanence report prepared by the social worker prior to adoption, plus other information passed on by professionals, foster carers, or birth family members. Adopters were provided with detailed definitions of types and levels of severity of maltreatment.
For all maltreatment variables except “singled out for rejection,” data were coded as follows: don’t know (score as missing), not experienced (Score 0), experienced at mild level (Score 1), likely experienced/unsure what level (Score 2), experienced at moderate level (Score 3), and experienced at significant level (Score 4).
With “singled out for rejection,” we created a dummy variable taking the value of one when experienced (encompassing “mild,” “likely,” “moderate,” and “severe”) and zero when this was not known to have been experienced (encompassing the previous codes “don’t know” and “not experienced”). This approach was taken because the preferential rejection or scapegoating of one child in the family was considered to be not an additional type of maltreatment (it may have manifested, e.g., as physical, sexual, or emotional abuse or neglect), but a factor making maltreatment psychologically worse for the child (because it was directed mainly or wholly at them and not at their siblings).
These 11 dimensions were then aggregated to 4 for the statistical analysis: neglect (medical neglect, nutritional neglect, emotional neglect, physical neglect, supervisory neglect); physical abuse; emotional abuse (emotional/psychological abuse, witness to domestic violence, singled out for rejection); and sexual abuse (sexual abuse involving contact, sexual abuse not involving contact).
The highest score on any one of the relevant subscales was used as the score for the neglect, physical abuse, and sexual abuse indicators. The emotional abuse indicator was constructed using the highest score on “emotional/psychological abuse” and “witness to domestic violence” and adding an extra score of 1 for “singled out for rejection” (if the child had experienced this). If data were missing for one or more of the subscales, the overall score for each of the four dimensions was still calculated using the highest score from remaining subscales. Pairwise correlation coefficients between maltreatment factors were high (all correlations being significant at the .05 level—see Table S4 in the supplementary materials), and the internal consistency was very high (Cronbach’s α statistics: .8025).
Indicators of adverse outcomes
The outcome indicators used in the model were adoptive parents’ reports of the adoption overall and of their child’s progress in eight different areas of development.
How was the adoption faring overall?
Five options were given. This variable was recoded as follows: 1 = going really well, 2 = managing challenges, and 3 = struggling (combining three options struggling, possible that the child won’t remain in the family, and adoption has broken down).
Child behavior, well-being, and relationships
Parents were asked to indicate whether their child showed strengths or challenges in eight different areas: general behavior in the home, general behavior outside the home, general physical health, emotional well-being, self-esteem, relationship with the parent completing the survey, social interaction with adults outside the family, and making and maintaining friendships. Respondents could tick one of the four options and these were assigned scores as follows: serious challenges (3), moderate challenges (2), no challenges (1), and a particular strength (0). Pairwise correlation coefficients between all outcome factors were all significant at the .05 level (Table S5 in supplementary materials). Values associated with the internal consistency were high (Cronbach’s α = .9049). These results, together with the results relating to the latent maltreatment index, support the use of a latent factor approach.
Covariates
The first set of covariates included factors found previously to be associated with child maltreatment:
The child’s sex
Male = 0, female = 1.
Exposure to drugs or alcohol in utero
0 = not known that the child had been exposed to either drugs or alcohol (don’t know, not experienced) and 1 = known exposure to drugs or alcohol or both (mild, likely/unknown level, moderate, significant).
Learning disability of birth parents
This was coded as 0 where neither birth parent was known to have a learning disability, 1 = where one parent was known to have a learning disability and 2 = both birth parents were known to have a learning disability.
Serious mental illness of birth parents
A variable for the presence of bipolar disorder and/or schizophrenia in birth parents was included. This variable was scored as 0 (neither parent known to have these mental illnesses), 1 = one parent is known to be affected, or 2 = both parents known be affected.
The age of the child when finally removed from the birth family
To account for potential nonlinearity in the relationship between the length of time the child was exposed to the birth parent environment and the maltreatment index, five different dummy indicators were defined, with cutoffs for the age of the child set at 3, 5, 11, 17, and 23 months old. The reference category was therefore a child that was finally removed from the birth parent(s) after 23 months.
A second set of covariates were those found in previous studies to be associated with child outcomes:
Time in foster family(ies) (time in care)
This was approximated by subtracting age at final removal from birth family from age at placement with adopters (or with foster carer adopters). To allow for nonlinearities, two binary variables were generated: the first took the value of 1 if the child spent less than 12 months in care; the second took the value of 1 if the child spent between 12 months and 24 months in care. The reference category was therefore a child that spent more than 24 months (2 years) in care (not with the family who adopted them).
Child’s distress on moving from the foster home
A binary indicator was generated from the question “Overall, how did your child find the process of moving to your household?” with five possible responses given. “Extremely difficult” and “somewhat difficult” were recoded as “difficult move” (1) and the other categories of response (neither easy nor difficult, somewhat easy, and extremely easy) were coded as (0).
Number of foster homes
0 = no or one previous foster home and 1= two or more foster homes before moving to the adoptive family.
Adoptive family—single or dual parenting
A binary variable was generated taking the value of 1 if the parent was single and 0 otherwise.
Child’s length of time in the adoptive family
This was calculated by subtracting the child’s age at placement in the adoptive family from their age in years at the time of the survey.
Statistical analysis
The structural model implemented (shown in Figure 1) comprised the following four different components that were being estimated simultaneously.
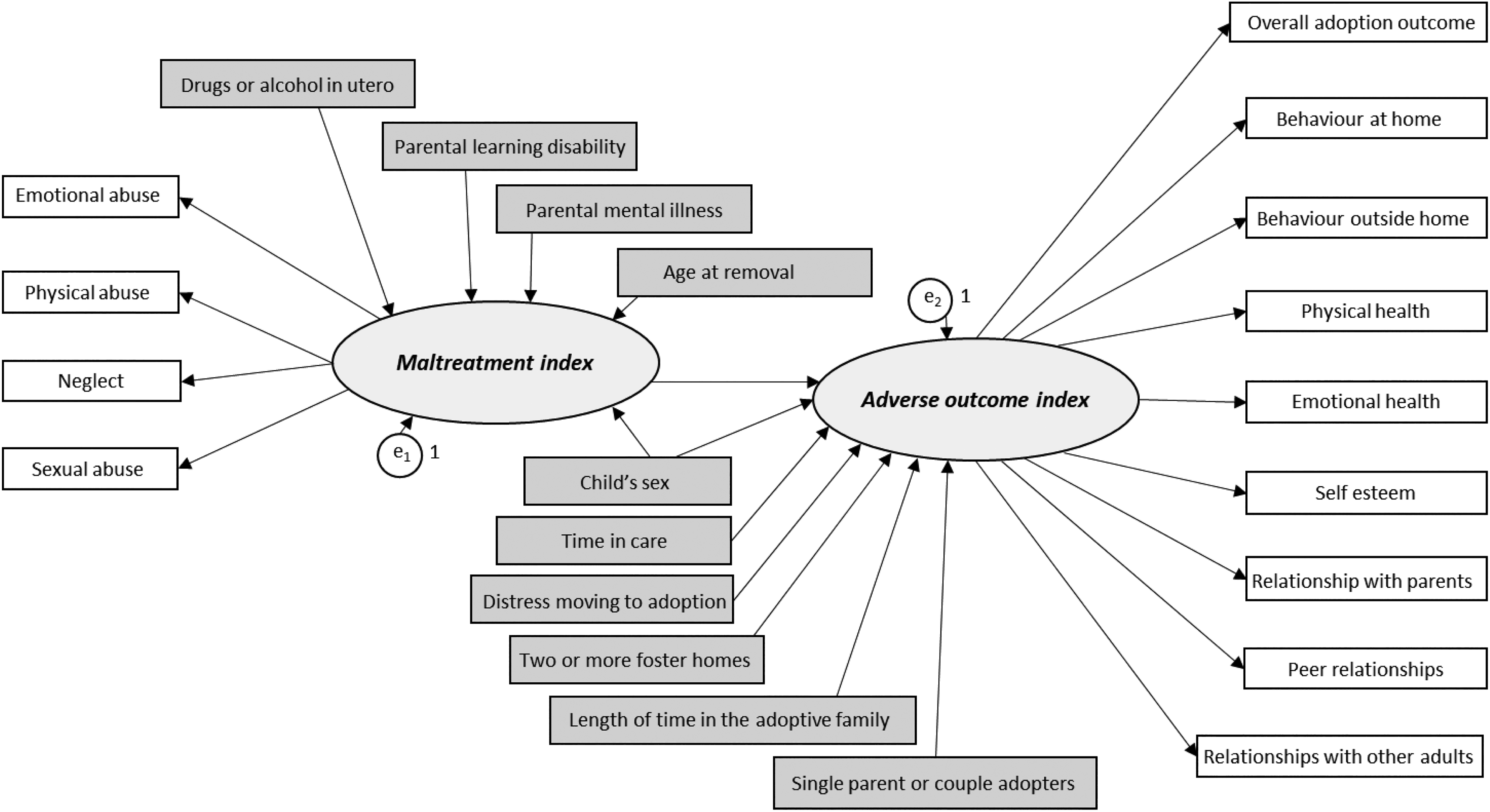
Latent factor structural equation model: Child maltreatment and adoption outcomes.
Child maltreatment
The exposure to and severity of maltreatment was modeled as a latent construct that cannot be directly observed but can be estimated by making use of parents’ responses to the questions about maltreatment. This maltreatment variable is shown as an oval on the left-hand side of Figure 1. The square boxes to the left indicate the four maltreatment aggregated indicators described earlier.
Factors influencing maltreatment
The underlying (latent) maltreatment index is allowed to covary with the set of covariates documented earlier. Because these factors are assumed to influence the child maltreatment score derived, they are shown in the model on the left-hand side, above the latent maltreatment index.
Measuring children’s adverse outcomes
Children’s outcomes were also modeled as a latent factor, measured using adoptive parent’s ratings of their child’s behavior, well-being, relationships, and how the adoption was faring overall. Higher scores on this index represented poorer outcomes; hence, we labeled this the “adverse outcome index.” This latent construct is shown on the right-hand side of Figure 1 in the oval figure, with the square boxes (to the right) representing the observed indicators used to estimate it.
Factors influencing outcomes
The adverse outcome index is then allowed to be influenced by a set of factors, including the maltreatment index. Other covariates included time in foster family(ies), number of placements in care, the child’s distress on moving from the foster home, length of time in the adoptive home, child’s sex, and whether the child was in a single or two-parent family.
Results
Descriptive statistics
The descriptive statistics for all the variables used in this analysis are provided in Tables S1 to S3 in the supplementary materials.
Neglect was the most prevalent form of maltreatment, with 59% of children having experienced this at a moderate or significant level. Almost half of the children (47%) had experienced moderate to very severe emotional abuse. In contrast, physical abuse was less commonly experienced (18% physical abuse at moderate or significant levels) and only 4% of children were reported to have experienced moderate or significant sexual abuse. All four types of maltreatment were significantly correlated with each other at the 5% level or higher, with the highest correlations being between emotional abuse and neglect.
In terms of how the adoption was going overall, 44% of parents said things were going well, 35% said they had challenges but were managing, and 21% said they were struggling. The most common child adverse outcomes reported by adopted parents were related to behavior in the home and emotional well-being with fewer concerns being shown about the child’s physical health, relationships with the adoptive parents, and social interaction with adults outside the home (see Tables S2 in supplementary materials).
Over half of the children (54%) were reported to have been exposed to harmful levels of drugs or alcohol in utero (see Tables S3 in supplementary materials). Almost one third of children (31%) had at least one parent with a learning difficulty. In contrast, just 5% of children had at least one parent known to have a bipolar or schizophrenic disorder. In terms of age at removal, almost half (48%) were removed from home in the youngest age band (under three months), but over one in five children (22%) were not finally removed until they were 2 years or older. The descriptive statistics also show that one third of children (33%) had lived with two or more different foster families before moving to their adoptive family.
Regression results
Factor loadings
Figure 2 shows estimated factor loadings for the maltreatment index. All abuse indicators had a significant and positive effect in determining the overall level of the maltreatment index. The most significant factors were emotional abuse and neglect. In other words, children who experienced these types of maltreatment had particularly higher levels/severity of maltreatment overall (see Figure 2). Note that for identification purposes we set the residual variance of both the latent factors equal to 1.
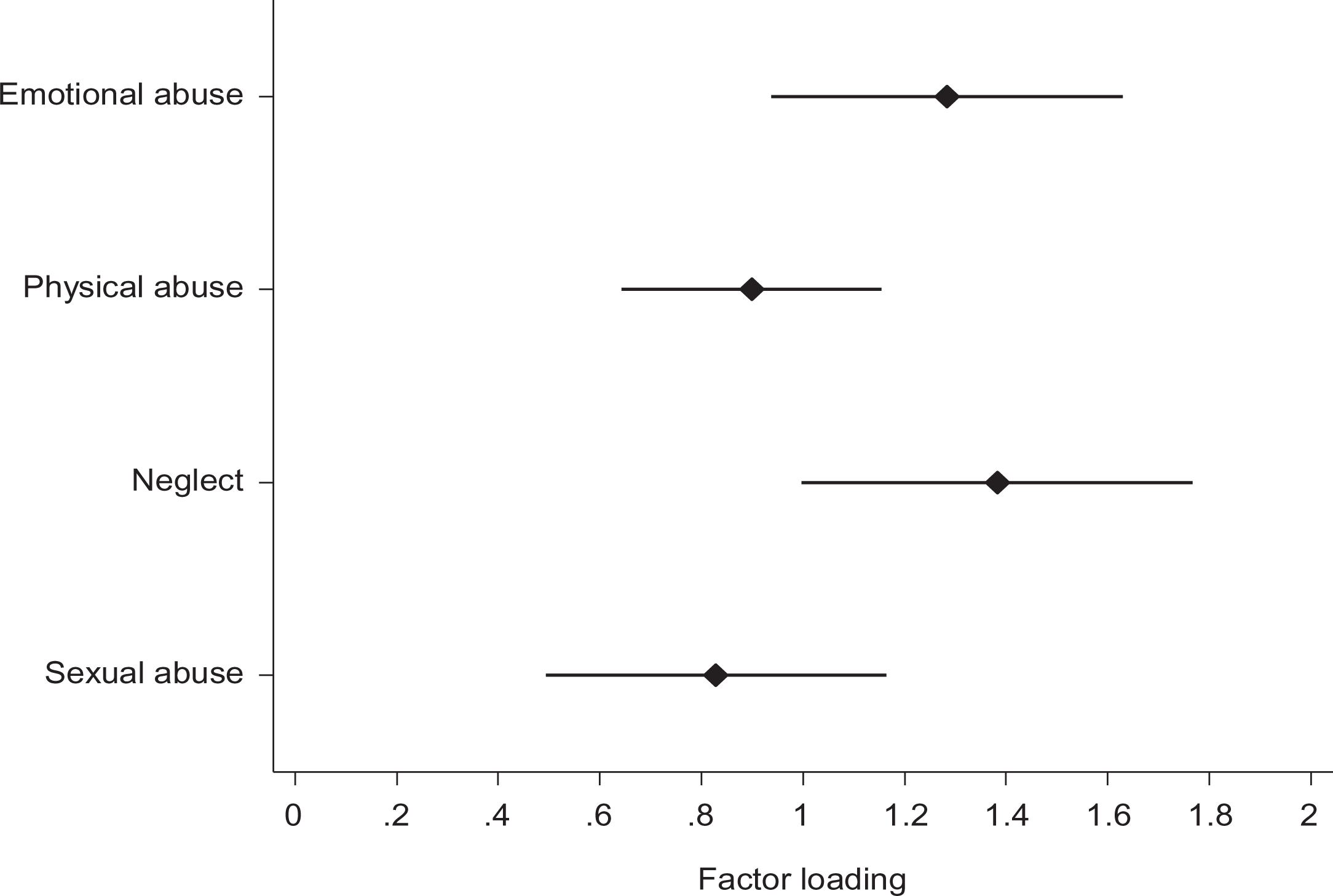
Estimated factor loadings associated with the maltreatment index.
Figure 3 shows the estimated factor loading for the adverse outcome index. Similarly, indicators on parents’ ratings of outcomes in the different areas loaded onto the adverse outcome index highly significantly. Some indicators were more relevant than others in determining the latent outcome index: the highest correlations were found for emotional health, self-esteem, and behavior at home. The overall adoption outcome indicator was also significantly correlated with the latent index derived (see Figure 3).
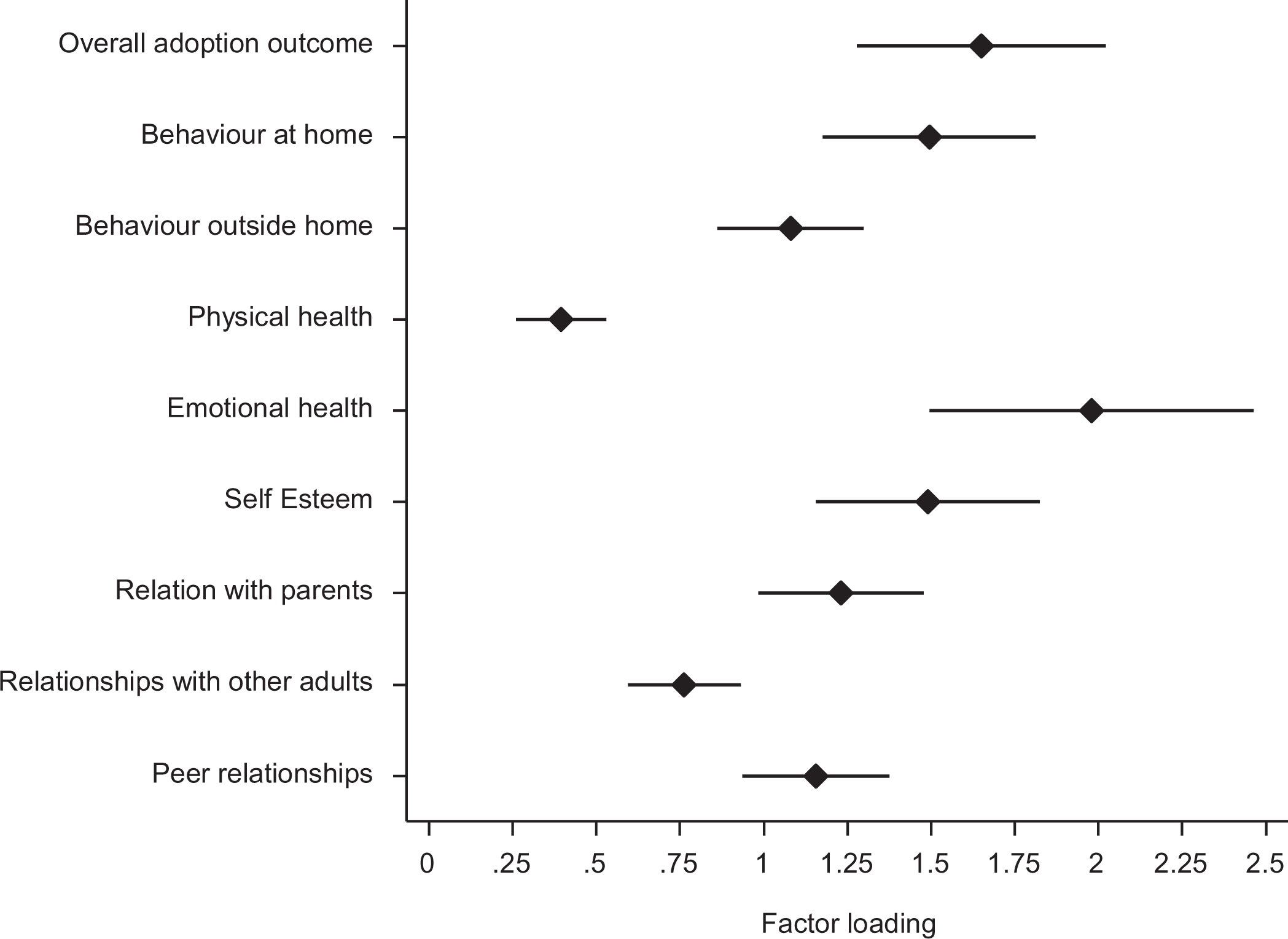
Estimated factor loadings associated with the adverse outcome index.
Estimated relationships for the maltreatment index
The first column of Table 1 provides estimated coefficients for the maltreatment index—the factors that influence the child’s experience of maltreatment. The latent maltreatment index significantly increased with the length of time the child was exposed to the birth family. Note that the effect was not linear: children who were removed from the birth parents when under 3 months had, as expected, significantly lower maltreatment index scores than those removed when aged 17 months or above. This group may stand out as it contained a large number of children removed either at birth or within their first month of life, so the length of exposure to the birth family environment was very minimal. Children removed from the birth family in all groups up until 18 months of age experienced less severe maltreatment than children who remained in the birth family for 2 years or longer. The maltreatment index was significantly higher for those children exposed to drugs and/or alcohol in utero. The maltreatment index was also higher for those children with birth parents affected by major psychiatric problems and learning disabilities. The effect, however, was significant at 5% level for learning difficulties only. Psychiatric problems were not associated significantly, when controlling for exposure to alcohol/drugs.
Estimated coefficients for the latent maltreatment index and the latent outcome index.
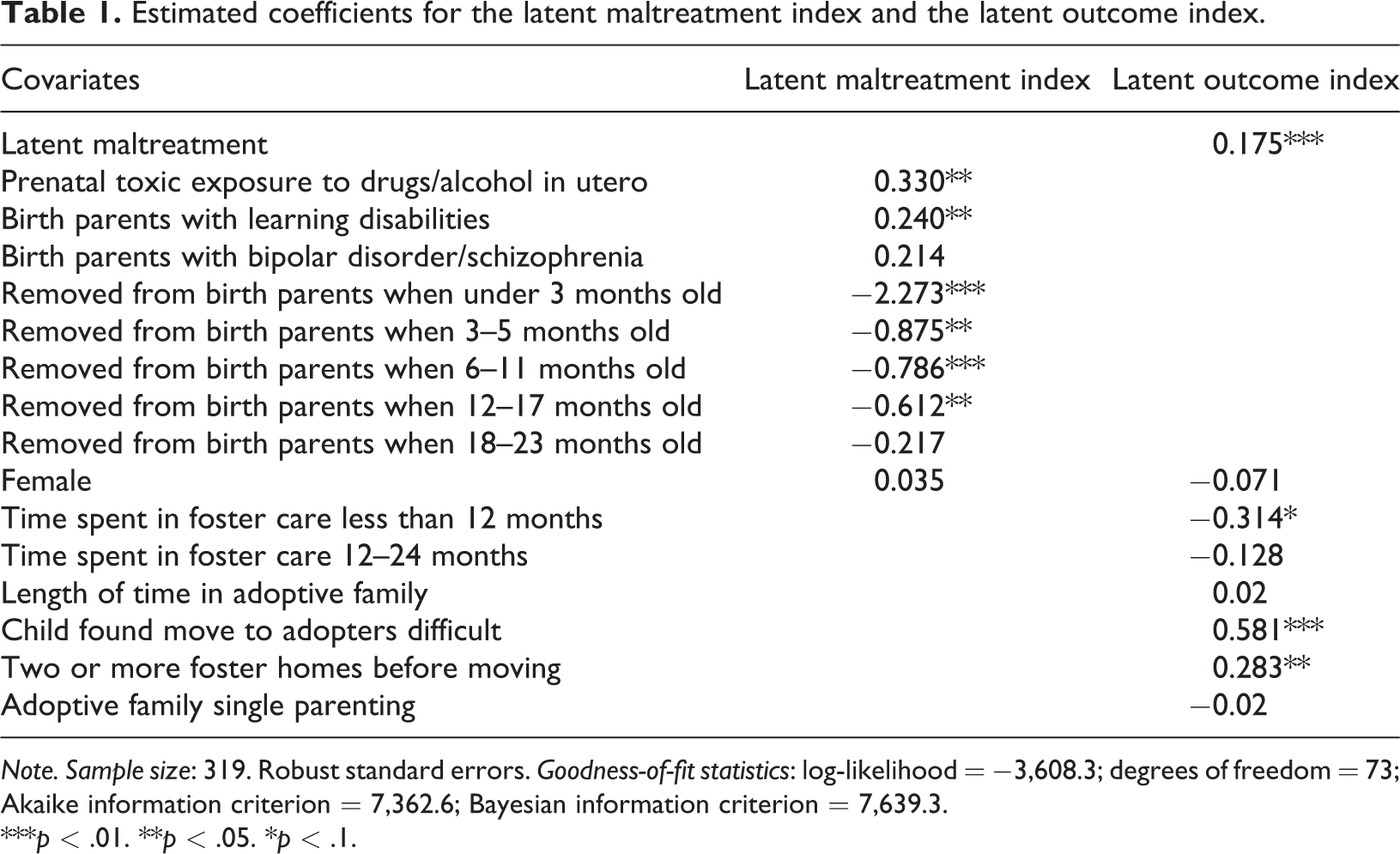
Note. Sample size: 319. Robust standard errors. Goodness-of-fit statistics: log-likelihood = −3,608.3; degrees of freedom = 73; Akaike information criterion = 7,362.6; Bayesian information criterion = 7,639.3.
***p < .01. **p < .05. *p < .1.
Estimated relationships for the outcome index
The second column of Table 1 provides estimated coefficients for the adverse outcome index. As expected, the latent adverse outcome index was significantly higher (i.e., worse) for children with a high value on the maltreatment index. The time that children stayed in foster care was negatively linked to the outcomes observed, all other factors being equal. Those children who stayed in foster care (in a different family to the one that adopted them) for less than 12 months had, on average, better outcomes than those who spent a longer period in care. Beyond 12 months, however, there were no significant associations between the outcome index and the time in care. Children who had two or more foster placements before moving to their adoptive family had significantly poorer outcomes than those who had just one foster placement or who were placed directly with their adoptive parents. Controlling for other characteristics, the length of time in the adoptive family (which was strongly linked to current age) had no significant association with the latent outcome. Those children who experienced the move to adopters as difficult were more likely to have poorer outcomes, when all other factors were taken into account. No significant differences between boys and girls were found either in terms of the latent maltreatment index or the adverse outcome index. Finally, it appeared that family structure was not significantly associated with outcomes: the coefficient associated with being a single parent was small in magnitude and not statistically significant.
Sensitivity analysis
Results from a fuller set of variations of the latent factor structural model in Figure 1 are available in the supplementary information (pp. 7–8). The most salient result was that exposure to drugs or alcohol in utero and learning disability of birth parents were both found to be positively and significantly associated with the adverse outcome index at 5% and 1% levels, respectively, indicating that these factors were independently associated with worse child outcomes.
Discussion
Adopted children’s outcomes (in terms of the overall progress of their adoption and the adopters’ ratings of the child’s progress in eight areas covering physical, emotional, and behavioral development and relationship with parents, peers, and others) were affected by range of risk factors each of which were significant when controlling for a comprehensive set of other factors. These factors included possible heritable factors (parental learning disability), the pre-birth environment (exposure to drugs or alcohol in utero), and the period of their life between birth and moving to their adoptive family (higher levels of maltreatment, spending more than a year in care, having two or more foster placements). The child’s distress on moving from the foster home to the adoptive family was also highly significant in linking to poorer outcomes. This confirms the findings of Selwyn et al. (2014) but demonstrates that this factor (arguably a risk created by the adoption system itself) is significant even when other factors are taken into account. Children’s outcomes did not appear to be significantly affected by their sex, whether they were in a single-parent or two-parent family, whether their birth parents had a mental illness (schizophrenia or bipolar disorder), or the length of time in their adoptive family. Although the older children in this study (and therefore those who had been in their adoptive family for longer) had much higher problems than the younger ones (Neil, Young & Hartley, 2018), our analysis suggests these differences were primarily to do with the higher levels of other risks factors for such children rather than their older age at the time of the survey.
Many of the factors identified as a risk for adopted children’s development concur with findings of previous research (Palacios, Rolock, et al., 2019). However, this novel analytical approach, previously not applied in adoption research, has enabled the relationship between the latent variables (maltreatment and child outcomes) to be examined alongside further observed variables simultaneously and within a single framework, providing more robust evidence about the individual impact of various factors.
Implications for policy and practice
Risks experienced before entering care, even before birth, impact significantly on children’s likelihood of experiencing maltreatment and directly on their adoption outcomes, pointing to the importance of supporting and protecting children in their families of origin before they enter care. Primary risk factors such as parental substance misuse need to be understood in the context of secondary risk factors such as poverty, ill-health, and housing problems (Brown et al., 2016; Bywaters et al., 2016; Sidebotham et al., 2006) but, in the United Kingdom, austerity policies have led to drastic cuts in family support services (Kelly et al., 2018). Alongside family support, timely safeguarding of children, and where necessary proactive planning for permanence, is also needed to prevent or reduce children’s exposure to maltreatment and promote their long-term welfare (Davies & Ward, 2012). While a policy focus on adoption support is much needed, this must considered alongside (not at the expense of) the provision of interventions at an earlier stage that support families and safeguard children.
Once a child enters care it is important to avoid unnecessary delay in permanency planning and to reduce the number of pre-adoption foster homes, preferably to one or none (i.e., where the child is adopted by foster carers). Concurrency or foster for adoption placements can reduce children’s time and moves in care (Dibben & Howorth, 2017; Monck et al., 2004). Purposive court and social work intervention and interdisciplinary practice with birth parents prior to and during the child’s placement in care can also reduce disruption for children and help parents tackle their problems, Family Drug and Alcohol Courts being one example (Harwin et al., 2018). Our analysis suggested the key difference for children was spending less than 12 months in care; there were no significant differences between those who stayed 12–24 months or more than 24 months. This may suggest that for children who have already waited a year, speed is not necessarily the most important factor—the quality of the in-care experience, the appropriateness of the match with adopters, and careful preparation of the child may be more significant. Our analysis found that child outcomes did not differ by family structure (one- or two-parent families). This suggests that when matching children, decisions should be based on the capacity of the parent(s) to meet the child’s needs, rather than on unfounded assumptions that couples can offer more than single parents.
When children do move from foster care to their adoptive family, the focus may need to switch from reducing time delays to moving at a pace that is comfortable for the child. There was little diversity in how transitions were handled in this study. The vast majority of moves were short (12 days on average from the child first meeting the adopters to them assuming full-time care). Whether or not foster carers stayed in touch after the move was very variable, and adoptive parents frequently described transitions as intense and exhausting (Neil, Young & Hartley, 2018). Transitions may be easier if there is greater temporal and relational overlap between the foster and adoptive family systems. This can be achieved by adopters and foster carers working together and at the child’s pace, and foster carers providing early support to the child and adopters after the move (Neil, Beek & Schofield, 2018; Boswell & Cudmore, 2017; Lewis, 2018).
Information about risk factors known to agencies at the point of placing children for adoption should be used to identify which children might need further specialist assessment and intervention. Screening for the possibility of FASDs where prenatal exposure to alcohol is known is important, as early diagnosis and appropriate treatment can help adopters to better understand their child’s needs and prevent secondary disabilities (Lange et al., 2013). Children who are showing signs of attachment difficulties or whose experience of adversity puts them at risk of such problems should be assessed for attachment disorders and parenting interventions such as video feedback or therapeutic play sessions should be offered (National Institute for Health and Care Excellence, 2015). Other common mental health problems, especially behavior problems, neurodevelopmental difficulties, trauma, and mood disorders, may also need to be considered and assessed by specialists (Woolgar et al., 2018).
Information about children’s risks should be used in the recruitment and preparation of adoptive parents. Adoptive parents commonly report feeling ill-equipped for the realities of parenting an adopted child; they are likely to value specialist clinical information and opportunities to connect to others with relevant personal experiences as well as access to services and parenting tools and strategies (Lee et al., 2018). Providing prospective adopters with more information about the impact of risks factors on children may help build their empathy and increase their confidence in considering a child with special needs such as FASD (Edelstein et al., 2017). Better initial preparation and training for adoptive parents can normalize expectations about the need for support and increase willingness to seek help later on (Wind et al., 2007). A focus on a wide range of risk factors beyond age at placement is important, as the support needs of children placed as babies and toddlers can be overlooked (Meakings et al., 2018). Simplistic or deterministic predictions about children’s development need to be avoided as sensitivity to risk varies and children’s outcomes are diverse (Woolgar & Simmonds, 2019), but building a realistic understanding of potential challenges balanced with a sense of optimism is important (Lee et al., 2018).
Limitations
Our analysis was able to include a good range of variables but the sample size, although large for an adoption study, limited the number that could be included. Other variables that could be studied in future research include, for example, the impact of structural and communicative openness, placement with siblings, the child’s development (disability and emotional and behavior development) at the time of placement, and adoptive parenting stress. It is also vitally important to study adoption outcomes as perceived by adoptees themselves.
A key limitation of the analysis is that adoptive parents reported both on the child’s history prior to adoption and their current outcome. In the light of the child’s current progress, parents may have (re)interpreted information given about the child’s past, or vice versa. We attempted to reduce this potential bias by including detailed definitions of the types and levels of severity of maltreatment. To attenuate the risk of “shared method bias,” future research should consider the use of triangulated information about children’s backgrounds and/or their progress (e.g., from adoptees, social workers, or teachers) although this yields the problem of dealing with potentially discordant reports. Adoptive parents were recruited via adoption agencies, and parents of older children may have been those who were actively seeking or receiving support, hence over representing adolescents with difficulties. This shows the importance of controlling for age at placement and other risks factors when analyzing cross-sectional samples of adopted children and adolescents.
Conclusion
This study found that adopted children’s adverse outcomes across several domains rated by their adoptive parents were negatively affected by a wide range of risk factors. The relatively large sample size enabled the novel use of latent factor structural equation modeling methods, allowing us to examine the independent effects of often highly correlated variables. Children were found to have experienced higher levels of maltreatment when they lived at home for longer and when their birth parents had learning difficulties and/or drug or alcohol problems. These problems of birth parents also negatively affected children’s outcomes regardless of levels of maltreatment experienced. Higher levels of maltreatment predicted worse outcomes for children after adoption, but the child’s duration in care and the number of foster homes were also influential. A new finding was that children who were distressed on moving from their foster home had worse outcomes, showing the importance of thinking about and addressing loss and separation for adoptees.
Improving outcomes for adopted children requires a focus on child welfare practices before and after adoption. Children adopted from care encounter many hazards in their lives before adoption, not just in their families but within the care system. Family support and child protection services are vital in reducing risks of maltreatment. Further harm due to multiple moves in care and poorly managed transitions into the adoptive family are preventable risks, and reducing these should also be a priority. Policy makers, practitioners, and prospective adopters need to use information about risk factors to make realistic and properly resourced plans for the support children may need, continually or episodically, after they have been adopted.
Supplemental material
Supplemental Material, supplementary_information_27_january - Exploring links between early adversities and later outcomes for children adopted from care: Implications for planning post adoption support
Supplemental Material, supplementary_information_27_january for Exploring links between early adversities and later outcomes for children adopted from care: Implications for planning post adoption support by Elsbeth Neil, Marcello Morciano, Julie Young and Louise Hartley in Developmental Child Welfare
Footnotes
Acknowledgements
The authors acknowledge the contribution of Dr. Irina Sirbu who assisted with production of the online survey and preliminary data analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from Barnardo’s on behalf of the Yorkshire and Humberside Adoption Consortium; Dr. Morciano’s contribution was supported by the Economic and Social Research Council, United Kingdom, through the Business and Local Government Data Research Centre Grant (grant number ES/L011859/1).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.