
Abstract
Maxillary transverse deficiency (MTD) is a common affliction among orthodontic patients, affecting 8%-17% of the population. Historically, MTDs have been treated using rapid palatal expanders (RPEs), typically anchored on molar and premolar teeth; however, their efficacy in achieving true skeletal expansion decreases dramatically during adolescence. For patients with mature sutures, a surgically assisted rapid palatal expansion (SARPE) was the only choice until the advent of miniscrew-assisted rapid palatal expansion (MARPE). In MARPE, the expansion screw is anchored on the basal bone through miniscrews. This provides a minimally invasive alternative to SARPE, while facilitating transverse maxillary expansion in older patients. There are many designs of MARPE in use. MARPE causes an increase in the width of the maxilla, with a more parallel separation of the midpalatal suture (MPS), with expansion effects reaching almost till the midfacial regions, minimal dentoalveolar effects, an increase in the airway, and effects are seen on the concomitant soft tissues. While the effects of MARPE have been well documented, the factors affecting its success are less understood. This position article on MARPE highlights the factors affecting the success and failure of MARPE. Procedures like corticopunctures and minimally invasive surgical and miniscrew-assisted rapid palatal expansion (MISMARPE) are being used to supplement MARPE and improve its success rate. Overall, MARPE is a highly successful procedure, well-accepted by patients and practitioners, and should be used when indicated, following the proper diagnosis of a true skeletal transverse deficiency of the maxilla.
Keywords
Introduction
Orthodontic diagnosis and treatment planning are fundamentally based on the assessment of the face and dentition in three dimensions—transverse, sagittal, and vertical. Of these, the transverse dimension has historically received the least clinical and academic attention. Until the early 1970s, orthodontic literature primarily focused on correcting discrepancies in the sagittal and vertical planes, with minimal emphasis on the transverse component. Furthermore, it was traditionally believed that transverse correction through orthopedic expansion was feasible only in growing patients, as the midpalatal suture (MPS) was thought to fuse by approximately 15 years of age.
As a result, diagnostic evaluation of skeletal or dental Class II and Class III malocclusions has often concentrated on sagittal and vertical aspects, with the transverse discrepancies being frequently overlooked. However, the transverse dimension warrants equal consideration in orthodontic diagnosis and treatment planning. Early identification and management of transverse problems are essential, as disturbances in this plane can influence occlusal relationships not only transversely but also in the sagittal and vertical directions. Since transverse growth completes the earliest among the three planes, it is often deficient by the time patients present for orthodontic treatment—making its timely recognition critical.
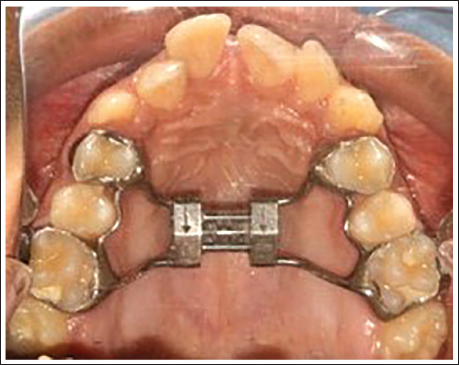
Maxillary transverse deficiency (MTD) is a relatively common condition, affecting approximately 8%-17% of the population.1, 2 It is typically characterized by unilateral or bilateral posterior crossbite, a constricted or high-arched palate, and dental crowding (Figure 1). 3 Although a posterior crossbite is a common clinical indicator, MTD may exist even in its absence. Hence, crossbite and MTD are not synonymous but rather represent a continuum of transverse skeletal imbalance. The dentofacial changes associated with MTD may also contribute to several anatomical and physiological consequences, such as reduced nasal airway volume, habitual mouth breathing, and a constricted V-shaped maxillary arch.4, 5 Because transverse growth ceases early, timely diagnosis of MTD is essential to prevent progression of both structural and functional issues.
Patient with Maxillary Transverse Deficiency Exhibiting Narrowing of the Maxillary Arch, Crowding, and Posterior Crossbite.

Traditionally, rapid palatal expansion (RPE) has been the treatment of choice for correcting MTD in preadolescent patients. RPE widens the maxilla by opening the MPS, thereby increasing both the transverse width of the dental arch and the nasal cavity. Conventional RPE appliances are typically tooth-borne and anchored to the maxillary first molars, or to both first molars and premolars, with or without palatal tissue support (Figure 2).6–8 The maxilla opens in a triangular pattern—greater anteriorly and hinging superiorly at the nasal base.
Conventional Rapid Palatal Expansion (RPE) Appliance or Hyrax Appliance Taking Support from Maxillary First Molars and First Premolars.
However, with advancing skeletal maturity, resistance to expansion increases due to progressive interdigitation and partial fusion of the midpalatal and circummaxillary sutures. Consequently, the efficacy and long-term stability of conventional RPE decline with age. 9 To address this limitation, surgically assisted rapid palatal expansion (SARPE) was introduced, where surgical osteotomies reduce the resistance of the circummaxillary sutures, allowing for expansion in skeletally mature patients. 10 Handelman et al. later advocated non-surgical slow maxillary expansion (NS-SME) in adults, utilizing the principles of alveolar bending and bone remodeling to achieve limited expansion. 11
More recently, the introduction of skeletal anchorage systems has revolutionized the management of transverse discrepancies in late adolescents and adults. The incorporation of temporary anchorage devices (TADs) or miniscrews in expansion appliances enables direct application of forces to the skeletal structures, facilitating true skeletal expansion and MPS opening beyond the conventional age limits of orthopedic expansion. This advancement has significantly broadened the therapeutic scope for managing MTD in non-growing patients.
Rationale
The primary objective of maxillary expansion is to widen the maxillary skeletal base rather than merely to expand the dental arch by moving teeth relative to the surrounding bone. Historically, RPE—most commonly achieved using a jackscrew-based appliance anchored to the maxillary first molars and premolars—was introduced to fulfill this goal. The underlying concept was that the application of rapid, high-intensity forces would minimize dental movements and instead transmit the force directly to the MPS, producing skeletal separation of the maxilla with minimal tooth displacement. In essence, rapid activation was intended to maximize skeletal effects while minimizing dentoalveolar changes. Although the principal movement involves the separation of the two maxillary halves, part of the expansion force is also transmitted to adjacent circummaxillary structures. 12
During RPE, the orthopedic appliance exerts significant force on the anchor teeth, leading to a transient reduction in blood flow within the buccal periodontium and the formation of extensive hyalinized areas. These conditions inhibit the normal remodeling activity of bone modeling units, essential for tooth movement within the alveolar bone, effectively stabilizing the supporting teeth until the MPS yields to the applied orthopedic forces. 13
Following active expansion, a stabilization or retention period is essential to allow for new bone deposition and consolidation at the expanded suture site. During this phase, the appliance maintains the achieved dental expansion; however, a degree of relapse occurs as the elastic recoil of the surrounding soft tissues causes the two maxillary halves to move slightly toward each other. Concurrent lateral dental movement on the supporting bone allows this adjustment to be possible.
In prepubertal and early adolescent patients, RPE with a tooth-borne expander can achieve transverse correction with approximately equal skeletal and dentoalveolar contributions—about 50% skeletal and 50% dental. However, in later adolescence, this ratio changes markedly to 35% skeletal and 65% dental, reflecting a diminished skeletal responsiveness to expansion forces.14, 15
When RPE is performed in late adolescent patients using conventional tooth-borne expanders, most of the observed correction is dentoalveolar rather than skeletal. The heavy orthopedic forces transmitted through the anchor teeth often result in undesirable side effects, including reduced alveolar bone thickness, buccal bone dehiscence and fenestration, excessive buccal tipping of posterior teeth, and gingival recession.16, 17
Therefore, when maxillary expansion is indicated in late adolescents or adults, it is crucial to employ a rigid system capable of delivering expansion forces directly to the basal bone. Such a design can achieve true orthopedic widening of the maxilla, minimize dentoalveolar side effects, and maintain the skeletal correction throughout the retention phase. The pursuit of an appliance that maximizes skeletal expansion while preserving periodontal health ultimately led to the development of the miniscrew-assisted rapid palatal expander (MARPE)—a hybrid design that combines skeletal anchorage using TADs with the conventional RPE framework.
The biologic rationale for this approach is grounded in evidence demonstrating that fusion of the MPS does not occur until well into the fourth decade of life.18–20 This finding supports both the feasibility and the unpredictability of achieving orthopedic expansion in young adults. By applying carefully directed forces through a suitably designed skeletal expander, the separation of a mechanically interdigitated yet patent suture becomes possible, rendering orthopedic expansion in young adults a realistic and biologically sound therapeutic option.
MARPE
The MARPE represents a simple modification of the conventional RPE appliance. 21 The key distinction lies in the incorporation of miniscrew implants within the palatal jackscrew assembly to provide direct skeletal anchorage, thereby promoting expansion of the basal bone while minimizing dentoalveolar tipping and dental expansion. MARPE is typically indicated in young adults between 16 and 25 years of age, presenting with transverse maxillary constriction.
The number, length, and placement sites of the miniscrews vary considerably among different MARPE designs. The term “MARPE” broadly encompasses any maxillary expansion appliance incorporating miniscrews for skeletal anchorage. However, there is currently no standardized design concept or universally accepted expansion protocol, and results from one MARPE study cannot be generalized to all designs. Each MARPE variant must therefore be evaluated individually to accurately determine its specific dental and skeletal effects.
Various forms of miniscrew-assisted expanders have been developed independently by early adopters, each guided by their distinct biomechanical philosophies and treatment concepts. The earliest report of a maxillary expander utilizing skeletal anchorage without dental support dates back to the year 1999. 22 Subsequently, appliances combining both dental and skeletal (miniscrew) anchorage began to appear around 2010,21, 23 and numerous studies have since been published describing their design and outcomes. We propose ‘Skeletally anchored maxillary expansion’ as a more generic term to describe this treatment modality.
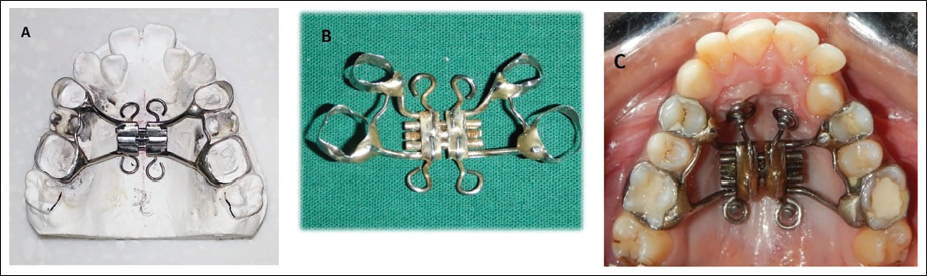
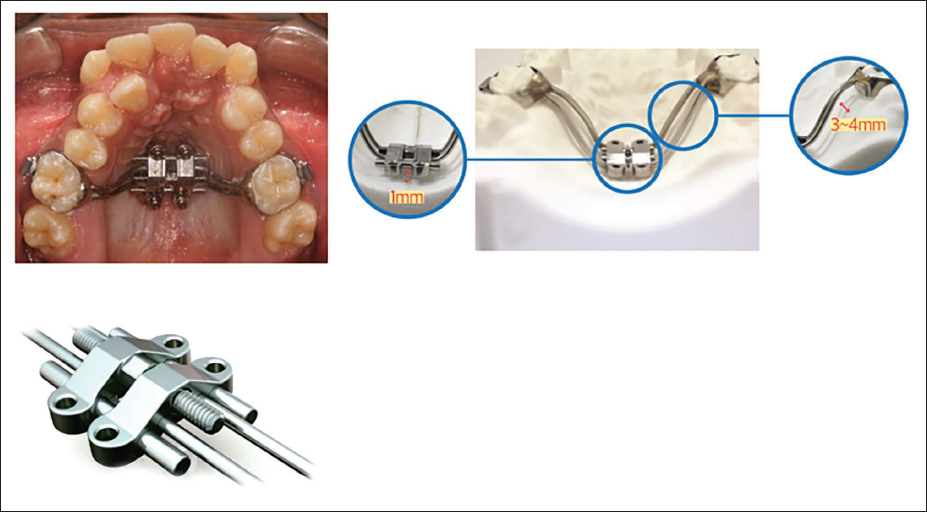
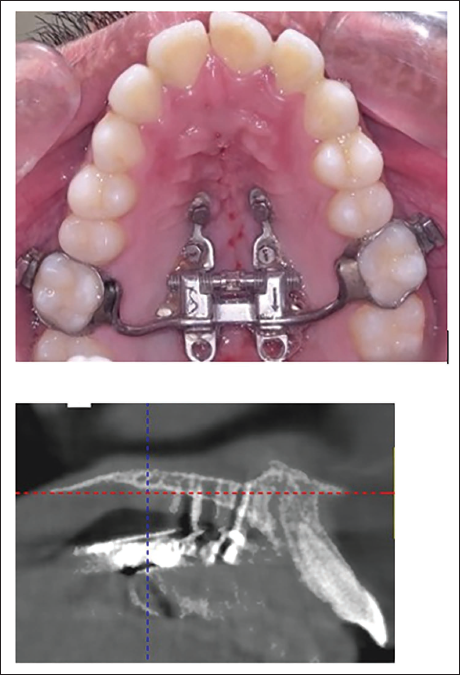
In the appliance described by Lee et al., 21 the MARPE consisted of four miniscrews: two anterior miniscrews positioned bilaterally in the anterior palate, lateral to the MPS, and approximately 3-4 mm posterior to the incisive foramen, and two posterior miniscrews placed parasagittally in the palate and connected to a Hyrax-type expansion screw (Figure 3). The patient was instructed to activate the screw one turn per day until the desired expansion was achieved, followed by a stabilization period of 3-4 months, similar to that of a conventional RPE.
Miniscrew-Assisted Rapid Palatal Expansion (MARPE) as a Modification of the Conventional RPE Appliance That has Four Rigid Wires Soldered to the Base of the Hyrax Screw, Two Anteriorly in the Rugae Area, and Two Posteriorly, Each Wire Ending in a Helical Hook (A). Miniscrews are Placed into the Palatal Bone Through the Center of the Hooks After Cementation of the Appliance (B and C).
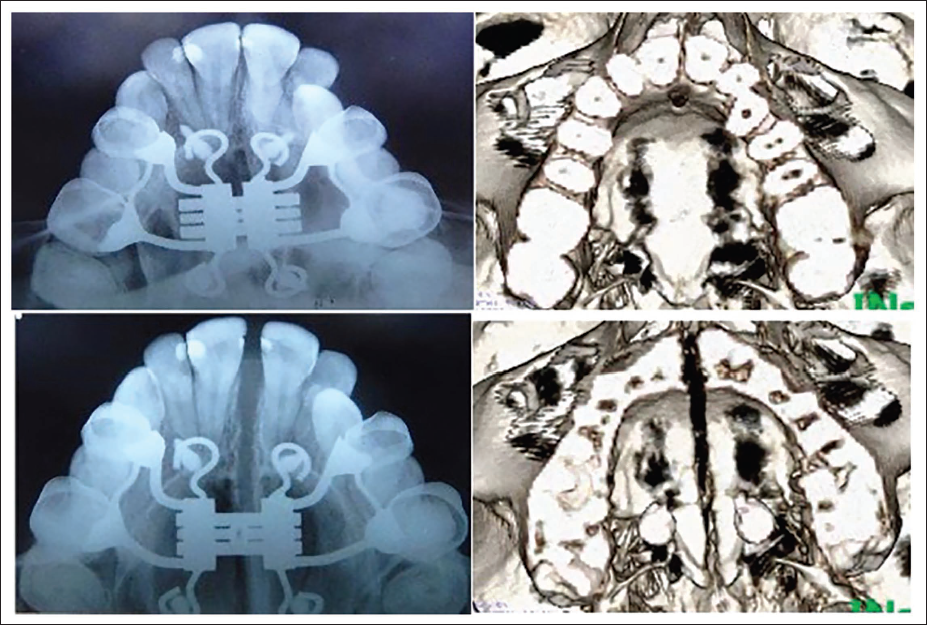
The resultant treatment effects represent a combination of skeletal and dentoalveolar expansion, as the appliance was both tooth- and bone-borne. The biomechanical rationale is that, by applying forces closer to the MPS, a more parallel and physiologic pattern of expansion can be achieved (Figure 4).
Parallel Separation of the Midpalatal Suture with Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in the Patient (19 Years/Female) Shown in Figure 3C.
While MARPE can effectively produce skeletal expansion in young adults with patent sutures, it cannot be expected to separate obliterated or fully fused sutures in older adults. Therefore, its use is best confined to late adolescent and young adult patients (typically from the late teens to mid-twenties). The primary objective of the appliance is to achieve maximum skeletal expansion in patients with patent sutures, rather than attempting to force separation in cases with advanced sutural fusion.
Classification
Skeletally anchored maxillary expansion appliances can be classified.
Based on the anchorage (Figure 5) as
Tooth- and bone-borne appliances or hybrid types, where anchorage is derived from both the teeth and miniscrews.
Two-arm design
Four-arm design
Bone-borne appliances, where anchorage is derived only from miniscrews (Figure 6).
Based on the sequence of appliance and miniscrew insertion.
A bone-first or TADs-first approach, where miniscrews are first placed in the areas of best cortical bone quality as per the T-zone concept, and the expander is constructed later to accommodate the miniscrew positions and is inserted.
Appliance-first approach, where the expansion appliance is inserted first, followed by the miniscrews. Here, the position of the appliance dictates the placement site of the miniscrews, rather than bone quality and quantity.
Based on the number of TADs (Figure 5).
Two-screw designs
Four-screw designs
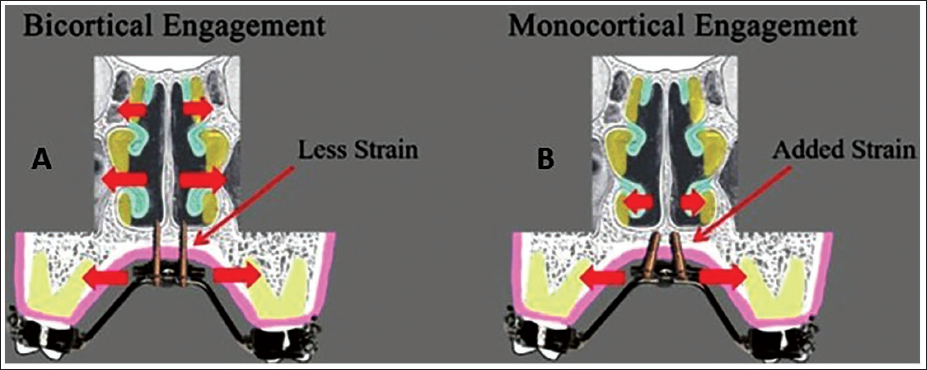
Based on miniscrew length and cortical engagement (Figure 7).
Monocortical
Bicortical
Based on the nature of fabrication.
Preformed appliances are available in different sizes.
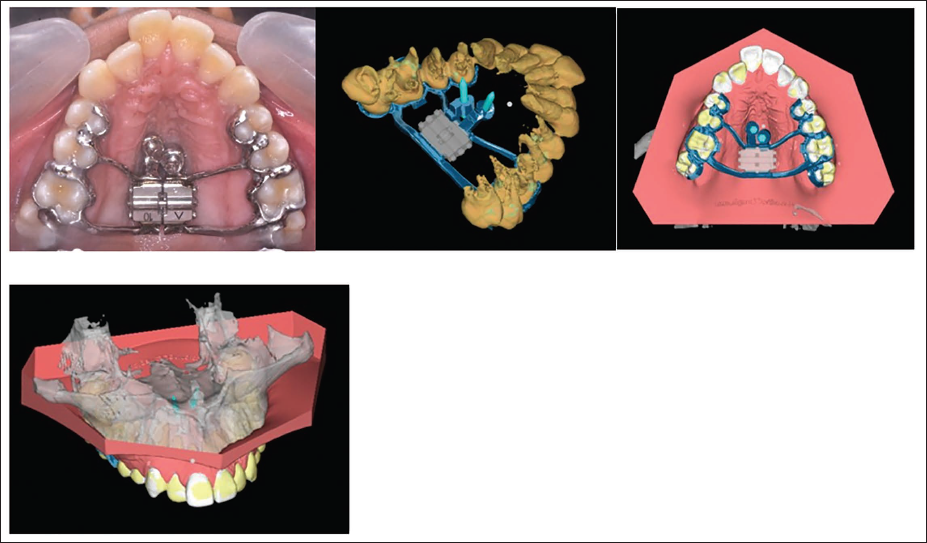
Customized appliances are fabricated using computer-aided design and computer-aided manufacturing (CAD-CAM) processes (Figure 8).
Miniscrew-Assisted Rapid Palatal Expansion (MARPE) Designs Based on Anchorage and Number of Temporary Anchorage Devices (TADs): (A) Tooth and Bone-borne Appliance with Four Minicrews and Four Support Arms; (B) Tooth- and Bone-borne Appliance with Two Minicrews and Two Support Arms; and (C) Bone-borne Appliance.
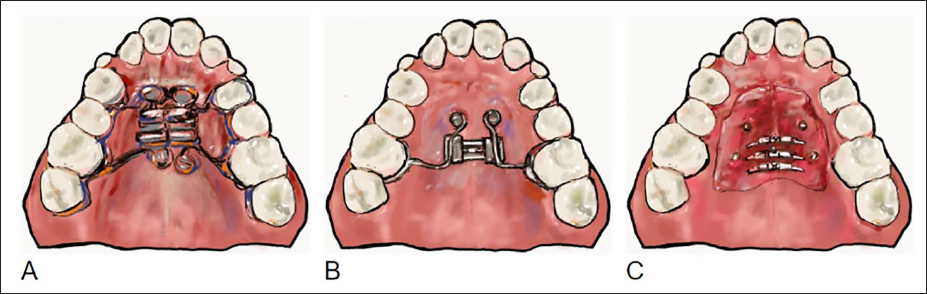
Bone Borne Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in a 15-year-old Male Patient.

Miniscrew-Assisted Rapid Palatal Expansion (MARPE) Designs Based on Miniscrew Length: (A) Bicortical and (B) Monocortical Engagement.
Customized Miniscrew-Assisted Rapid Palatal Expansion (MARPE) in Narrow Palates Using Computer-Aided Design and Computer-Aided Manufacturing (CAD-CAM) Processes Using Cone-Beam Computed Tomography (CBCT) Integration and 3D Printing.
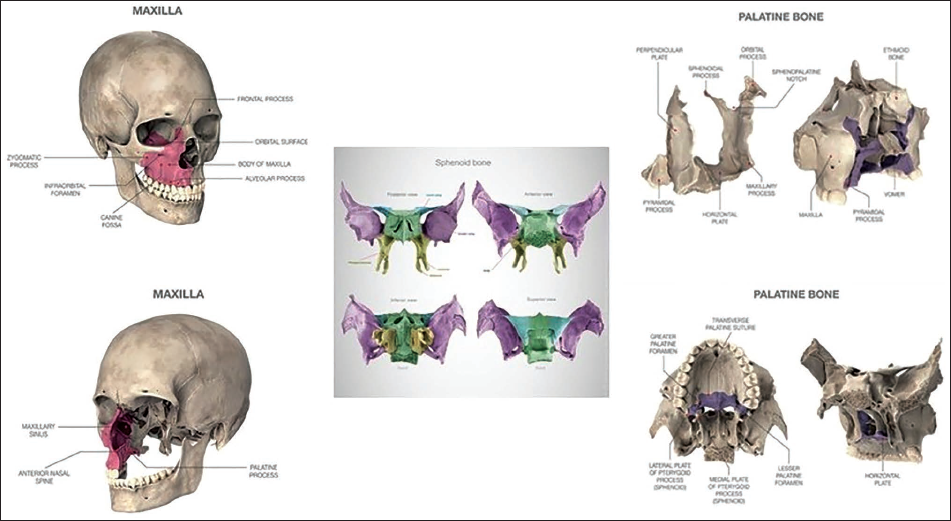
Anatomical Considerations
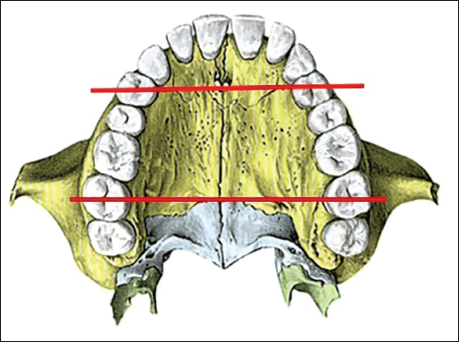
The MPS represents not only the fusion of the palatal processes of the maxillae but also the union of the alveolar processes of the right and left maxillae, and the horizontal osseous plates of the palatine bones. Therefore, any modification of this region affects the entire length of the suture as well as its adjacent anatomical structures. The suture can be divided into three distinct segments (Figure 9): The anterior segment, located anterior to the incisive foramen (the intermaxillary segment); The middle segment, extending from the incisive foramen to the transverse suture between the maxillary and palatine bones; and The posterior segment, which represents the suture between the palatine bones beyond the transverse suture.
The Midpalatal Suture Consists of Three Segments—the Anterior, Middle, and Posterior.
The principal resistance to the opening of the MPS is believed to lie not within the suture itself, but rather in the surrounding craniofacial structures—particularly the sphenoid and zygomatic bones (Figure 10).24, 25
Areas of Osseous Resistance to Midpalatal Suture Opening—Zygomatic and Sphenoid Bones.
The maxillae articulate with 10 other bones of the facial and cranial skeleton (Figure 11). Posterior to the maxillae lies the sphenoid bone, which forms the midsagittal portion of the anterior and middle cranial base. The pterygoid plates of the sphenoid, though positioned bilaterally, lack a midsagittal suture that would permit lateral displacement. Furthermore, the pyramidal processes of the palatine bones interlock with these pterygoid plates. This interlocking configuration provides a confining effect, significantly restricting the capacity of the palatine bones to separate along the midline.
Articulations of the Maxilla, Sphenoid, and Palatine Bones.
As the maxillae begin to separate during expansion, the zygomatic processes offer additional resistance; however, the complex system of sutures allows for compensatory adjustments or repositioning of the expanded structures. More posteriorly, the pterygoid plates of the sphenoid can bend slightly under applied pressure, but their resistance to deformation increases markedly in regions closer to the cranial base, where the bone is substantially more rigid (Figures 10 and 11).
Biomechanics
The biomechanical effects of conventional RPE and miniscrew-assisted rapid palatal expansion (MARPE) appliances can be described as comprising three main components: (a) buccal tipping of maxillary molars and/or premolars, (b) bending of the alveolar bone supporting the maxillary molars and/or premolars, and (c) separation of the MPS, leading to the division and rotation of the maxillary halves. 26
The location of force application relative to the resisting structures plays a decisive role in determining the pattern of expansion. Since most maxillary sutures are located posteriorly, this region provides the greatest resistance to expansion. The pterygomaxillary fissure, zygomaticotemporal, and zygomaticofrontal sutures are considered the primary sites of resistance during maxillary expansion.27–30
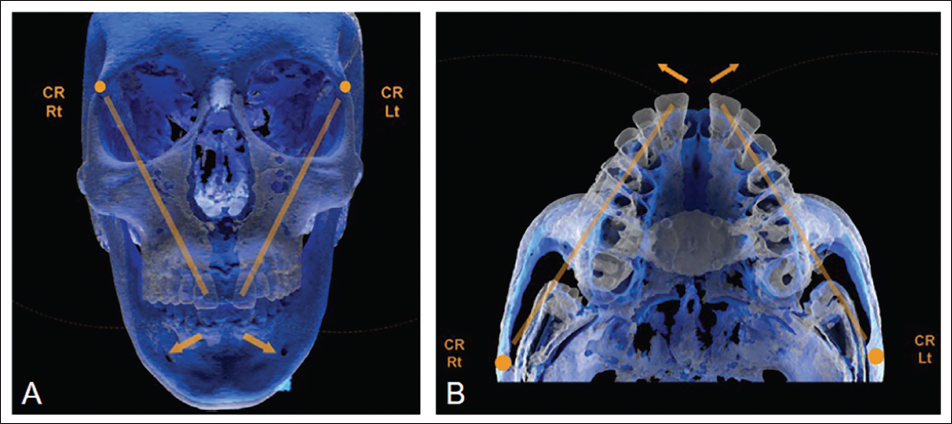
In MARPE appliances, the center of rotation of the maxilla in the frontal plane has been reported near the superior portion of the frontozygomatic suture, 31 while in the horizontal plane, it is situated near the proximal region of the zygomatic process of the temporal bone (Figure 12). 32
The Center of Rotation During Maxillary Expansion with Miniscrew-Assisted Rapid Palatal Expansion (MARPE) is Close to the Frontozygomatic Suture in the Vertical Plane (A) and the Proximal Portion of the Zygomatic Process of the Temporal Bone in the Horizontal Plane (B).
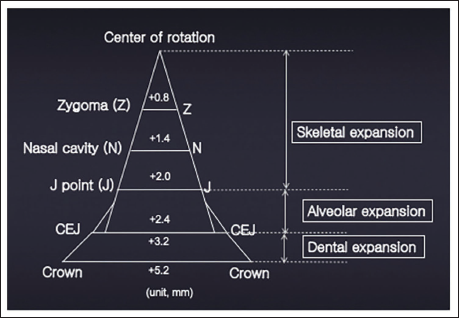
From a biomechanical standpoint, the expansion screw should ideally be positioned close to the center of resistance of the maxilla to enhance translatory movement and reduce rotational tendencies. In MARPE, the point of force delivery is deeper within the palatal vault, potentially bringing it closer to the center of resistance. 33 Consequently, MARPE produces broader skeletal effects, with maxillary expansion extending up to the zygomatic arch, 34 and influencing various perimaxillary sutures (Figure 13).31, 32
Diagrammatic Representation of Transverse Changes at Various Levels of the Maxilla After Maxillary Expansion with Miniscrew-Assisted Rapid Palatal Expansion (MARPE).
Research has demonstrated MPS separation accompanied by pterygopalatine suture opening in 16 (53%) of 30 cases, as well as a pyramidal expansion pattern of the zygomaticomaxillary complex associated with downward and forward displacement.35, 36
A key biomechanical distinction between hybrid and bone-anchored MARPE lies in the stress distribution: bone-anchored designs exhibit nearly double the stress concentration around miniscrews compared with hybrid systems. 37 In bone-borne appliances, miniscrews can be positioned either laterally to the MPS or along the palatal slopes. Finite element method (FEM) studies indicate that placing miniscrews closer to the MPS results in higher stress concentration in that region, while positioning them laterally yields more parallel displacement of the buccal bone and a more uniform suture opening. 38
In hybrid appliances, the expansion force is distributed between two structures—the MPS (via miniscrews) and the maxillary molars alone, or with the maxillary premolars. Consequently, hybrid MARPE produces lower stress levels in the midpalatal and circummaxillary sutures compared with bone-anchored systems. 37 Including dental anchorage along with miniscrew anchorage in hybrid MARPE appliances seems to improve biomechanical efficiency, according to their originators, as explained below.
Given the triangular configuration of the maxilla and its posterior fixation, forces applied at the tooth level in hybrid tooth-bone-borne expanders generate greater bending moments near the MPS. This leverage effect may facilitate suture splitting. 39
In mature patients, the interlocked MPS undergoes considerable three-dimensional torsion during expansion. The four implants experience excessive strain and tipping as the two maxillary halves diverge. The inclusion of maxillary molars for stabilization in hybrid designs maintains the jackscrew’s position in three dimensions, thereby reducing implant strain and preventing loosening or fracture. 40
For effective RPE, it has been suggested that expansion forces should range between 73 N (7.44 kg) and 154 N (15.70 kg). 41 While all MARPE configurations can generate this magnitude of force, two-armed hybrid MARPE devices produce greater expansion force—owing to their increased rigidity—compared with four-armed appliances. 42
Another factor influencing the force system of expansion devices is the retention arm design of the expansion screw. Screws with identical cross-sectional diameters can exhibit different loading capacities depending on the force, stress, and deformation characteristics of their arms. Notably, greater screw stiffness—in both body and arms—results in higher expansion forces. Because two-arm appliances generate higher forces per activation, they also experience greater deformation of the expansion key, retention arms, and screw body compared with four-arm designs. 43 The increased deformation during activation arises from elevated forces and reduced stiffness, as the arm length increases with screw opening.
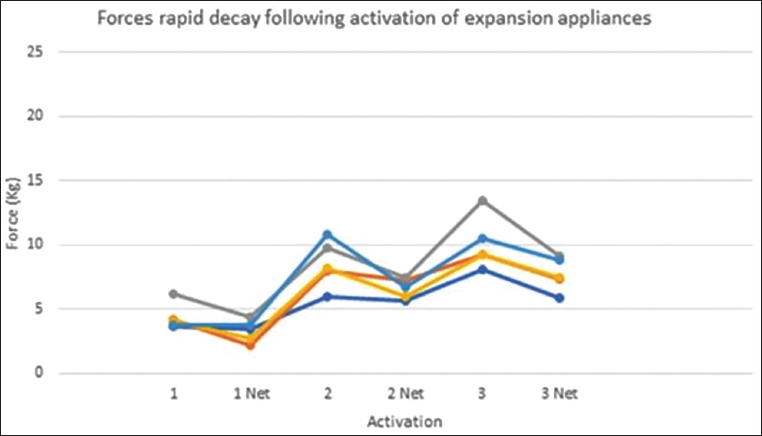
The following key principles regarding force behavior during maxillary expansion, derived from studies on conventional RPE and applicable to MARPE, should be recognized.26, 29, 30, 41, 44
A cyclical pattern of force activation and decay occurs after each activation turn;
The cumulative nature of expansion forces contributes to overall skeletal change; and
A constant residual force persists between activations (Figure 14).
The Cycles of Force Activation and Decay in Expansion Appliances. 26
When comparing MARPE systems, appliances with four miniscrews exhibit lower maximum stress per miniscrew than those with two, due to the more effective distribution of force across a greater number of screws.45, 46 Consequently, two-screw MARPE is generally indicated for younger adolescents, where the MPS is less interdigitated, while four-screw MARPE is recommended for adults, who require greater anchorage and experience more resistance to suture separation. 46
MARPE can employ miniscrews with either monocortical or bicortical anchorage. In monocortical designs, screws engage only the palatal cortical bone, whereas bicortical anchorage involves longer screws that reach the nasal floor cortex for added stability. Evidence comparing these techniques is mixed. Bicortical anchorage has been suggested to provide improved stress distribution and reduced miniscrew deformation, though findings remain inconclusive.45, 47–50 A recent randomized clinical trial found that miniscrew length did not significantly affect the success rate of MPS opening. 51 However, a recent meta-analysis indicated that miniscrews shorter than 8 mm are associated with higher failure rates.52, 53
In summary, the success rates of MARPE using either monocortical or bicortical anchorage appear comparable, provided that miniscrews shorter than 8 mm are avoided.
Maxillary Skeletal Expander (MSE) 54
The MSE is a specific subtype of MARPE, first developed around 2003, and it has since undergone several design refinements. The appliance consists of a rigid jackscrew body incorporating four slots for miniscrews, and four flexible metal arms—two on each side—soldered to bands on the permanent first molars (Figure 15).
Design of the Maxillary Skeletal Expander (MSE) Appliance.
Most MARPE designs position miniscrews in the anterior maxillary palate, where bone quality and density are superior. Consequently, these appliances tend to produce greater expansion in the anterior and inferior regions of the maxilla than in the posterior and superior regions.
In contrast, the MSE’s jackscrew is positioned between the maxillary first molars, enabling it to apply expansion forces in a more posterior and superior direction. The jackscrew is stabilized by four miniscrews that are closely adapted to the palatal vault (Figure 15). During activation, lateral forces are transmitted directly to the MPS, medial to the zygomatic buttress, resulting in a more uniform anteroposterior expansion.
Because the four miniscrews are spread out and integrated into the rigid framework of the jackscrew, the expansion achieved is highly parallel, frequently leading to the disarticulation of the pterygopalatine suture. 55 The MSE is designed to fit snugly against the palatal vault, and since its expansion forces act directly along the suture line, the lateral rotational movement of the maxillary halves—common with other expanders—is substantially reduced. Additionally, longer miniscrews are used in MSEs to ensure bicortical engagement with both the palatal and nasal cortical plates.
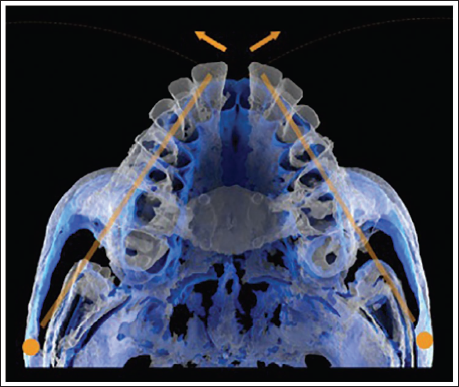
Because the lateral expansion forces are delivered high in the palatal vault and close to the zygomatic buttress, the rotational fulcrum is displaced further away compared to other MARPE systems. This results in a more translatory pattern of expansion (Figure 16). Consequently, the clockwise rotation of the mandible and associated bite opening are minimized, while archial movement of the hemi-midface occurs around a fulcrum near the frontozygomatic sutures.
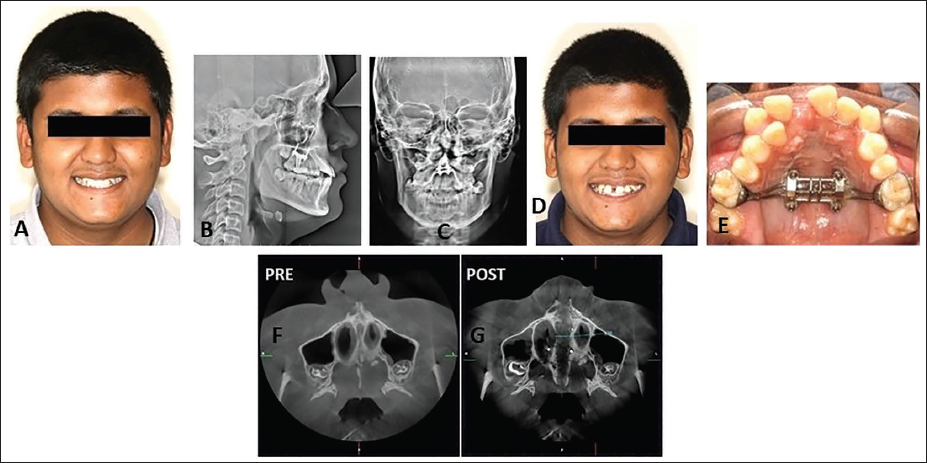
Maxillary Skeletal Expander (MSE) Placed in a 16-year-old Male Patient (A) Showing Bicortical Engagement of the Miniscrews (B,C), Appearance of Midline Diastema (D,E), and Axial Cone-Beam Computed Tomography (CBCT) Sections (F,G) Showing Parallel Midpalatal Suture Separation, with a Good Ratio of Expansion Screw Opening to Suture Separation (9.2 mm Screw Separation Producing 8.55 mm Suture Separation).
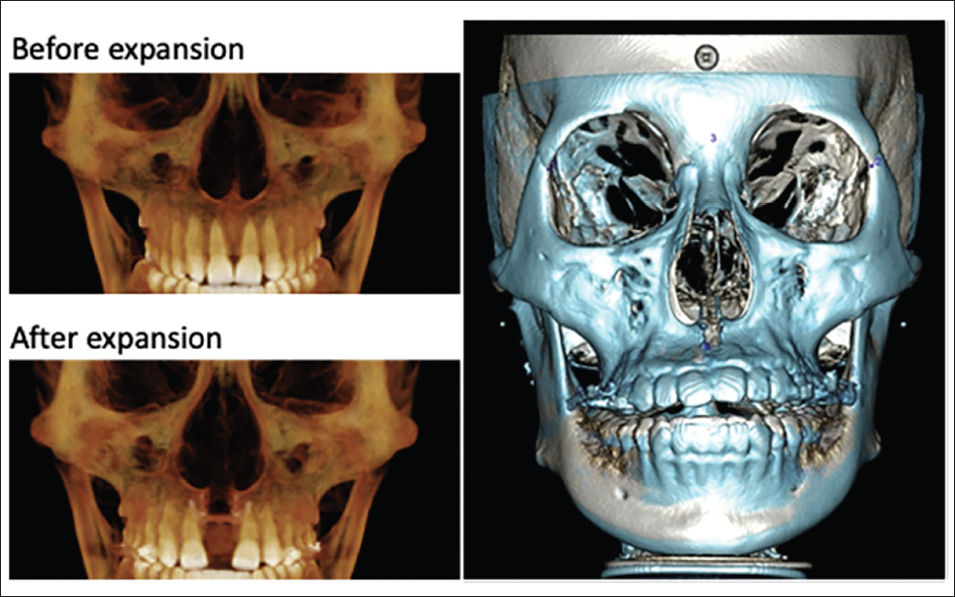
By promoting a near-parallel skeletal expansion, the MSE causes a substantial increase in nasal cavity volume and facilitates loosening or disarticulation of perimaxillary sutures. Improvements in nasal airflow and breathing function following MSE treatment have been documented in recent studies, and the combination of MSE with facemask therapy has been shown to produce enhanced orthopedic effects.
In cases where miniscrews tip or are dragged through the thin palatal bone, some of the expansion forces may inadvertently be transferred to the connecting arms and subsequently to the anchored teeth. To prevent this undesirable dental loading, MSEs are equipped with nonrigid metal arms that help absorb excess force, thereby minimizing unwanted tooth movement.
Effects of MARPE
Skeletal Effects26, 56
MARPE produces an increase in maxillary width, which is typically greater anteriorly than posteriorly (Figure 17).
Expansion occurs as a pyramidal opening of the maxilla in the coronal plane, with the base of the pyramid at the palate and tapering superiorly (Figure 18).
A significant increase in nasal cavity volume is observed.36, 57
There is an increase in bilateral nasofrontal suture width.
The zygomaticomaxillary suture distance also increases following expansion.
In Class II patients, MARPE may facilitate anterior repositioning of the mandible, particularly when mandibular growth is restricted by a constricted maxilla. 58
It can contribute to the improvement of abnormal condylar positioning. 59
Due to its distraction-like effect on perimaxillary structures, the deficient midfacial complex in skeletal Class III patients can be advanced more effectively when facemask protraction forces are used concurrently.
There is an Increase in the Transverse Width of the Maxilla, with More Widening Anteriorly than Posteriorly, as can be Seen in This Superimposition of Cone-Beam Computed Tomography Scans (CBCTs) Taken Before (Blue) and After (White) Expansion.
A Superimposition of the Pre- (White) and Post-expansion (Blue) Cone-Beam Computed Tomography (CBCT) Shows a Pyramidal Pattern During Maxillary Expansion, with the Palate as the Base.
Dental Effects
Buccal tipping of maxillary molars may occur.26, 60
In bone-borne appliances, this results primarily from alveolar bending.
In hybrid appliances, it arises mainly due to the buccal component of the applied force.
Intermolar and interpremolar widths increase—this change is typically greater with two-arm appliances compared to four-arm designs. 26
A transient midline diastema is a common finding during active expansion.
In a study by Paredes et al., 62 it was reported that traditional linear measurements tend to overestimate the dentoalveolar effects of MARPE. They recommended the use of angular measurements for a more precise evaluation. According to their analysis, linear measurements suggest approximately 60% skeletal, 16% alveolar, and 24% dental contributions to total expansion. However, angular measurements indicated that the expansion was composed of over 95% skeletal rotation, less than 0.5% alveolar bending, and under 4.5% dental tipping in a sample of 39 patients. The authors concluded that while angular analysis offers a more accurate biomechanical interpretation, linear assessments still provide a reliable representation of the overall 3D clinical effect of MARPE.
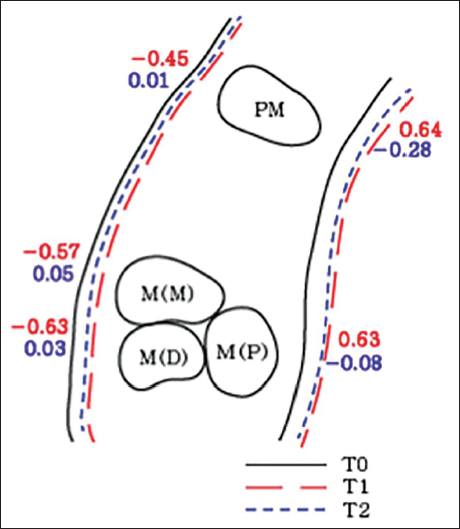
Periodontal Tissue Effects (Figure 19)60, 61
A decrease in buccal bone thickness is typically observed during expansion, with a slight recovery noted during the consolidation phase.
A modest increase in palatal bone thickness may occur following treatment.
After Expansion (T0 Pre- and T1 Post-expansion), There is a Decrease in the Buccal Plate Thickness with Mild Increase Seen in the Consolidation Phase (T2). There is Also an Increase in the Palatal Plate Thickness. 61
Soft Tissue Effects
Functional Effects
Patients frequently report an improvement in nasal breathing following expansion.
Apnea-hypopnea index (AHI) scores and symptoms of obstructive sleep apnea (OSA) show measurable improvement after treatment. 66
A transient rise in intracranial pressure may occur during screw activation. 67
A retrospective analysis found that the MPS opening efficiency—defined as the ratio of screw expansion to actual suture separation—was 71% anteriorly and 63% posteriorly. 35
In a related study, Park et al., 34 reported that skeletal expansion accounted for 37%, while alveolar expansion contributed 22% of the total expansion achieved by MARPE—values that are notably higher than those typically observed with conventional RPE. This indicates that MARPE produces predominantly skeletal effects. Furthermore, the mode of MPS separation differs from that of traditional RPE; MARPE produces a nearly parallel opening with an anterior-to-posterior ratio of 90%, whereas conventional RPE produces greater anterior and lesser posterior separation. 35
Rate of Expansion in Skeletally Anchored Expanders
The concept of rapid activation in conventional RPEs, which use teeth as anchorage, was originally developed to enhance skeletal changes while minimizing dental side effects. However, with skeletally anchored expanders that utilize miniscrews engaging the basal bone directly, the question arises—is rapid activation still necessary?
The primary objective of treatment with skeletally anchored expanders is not to generate excessive force, but rather to apply the expansion force directly to the bone, minimizing or eliminating pressure on the teeth. In young adults, where the jackscrew is secured to skeletal anchors, a rapid separation of the suture can be disadvantageous. Therefore, slow expansion (<2 mm per week) is preferred over rapid expansion. This slower rate induces intersutural tension, leading to bone apposition within the suture. However, the accumulated tension is not sufficient to break apart the interlocked bony structures, and the expansion force remains concentrated within the suture itself (Figure 20).
During Expansion, Slow Force Application Causes Tension in the Sutures, Which, While Adequate for Skeletal Expansion in Preadolescents, is not Enough to Overcome the Resistance Offered by the Interlocking Maxillae of the More Mature Suture in Late Adolescents and Adults. A Rapid Force is Required to Overcome This Resistance. 54
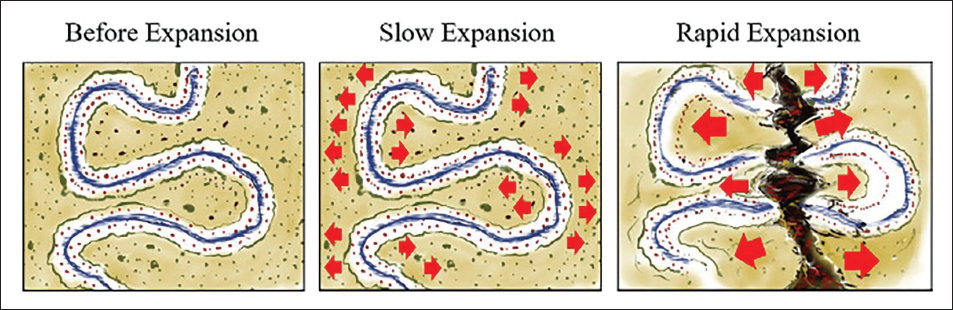
With increasing skeletal maturity, higher levels of force become necessary, and more frequent activations are often recommended. As the MPS matures, the two hemimaxillae become more interdigitated at their medial surfaces, and the expansion force must overcome this interlocking—particularly when a rapid approach is employed (Figure 20). The rising tension from periodic activations results in microfractures within the interlocked bone, eventually leading to the separation of the MPS.40, 54
As intersutural tension increases during activation, inflammatory processes within the suture stimulate osteogenic activity, facilitating suture splitting. Without this biological response, separation of heavily interlocked sutures may not occur. If repeated activations fail to achieve suture opening due to unfavorable mechanical dynamics, a resting period should be allowed for biological recovery. When expansion is resumed after this rest, suture separation often follows.
Hence, intermittent delivery of heavy expansion forces is considered ideal, utilizing both mechanical and biological mechanisms to achieve effective expansion. However, the optimal magnitude of applied force and the appropriate duration of rest periods remain uncertain. 54
MSE II Expansion Protocol—Clinical Recommendation (as per Won Moon)
According to Won Moon, activation should be continued until resistance to expansion is felt, after which one or two additional activations can be performed each day. 54 This approach maintains consistent intersutural tension, helping to gradually weaken the interlocked bony structures while stimulating osteogenic activity within the suture. This also accounts for daily variations in individual biological responses. Once a midline diastema becomes visible, the activation rate should be reduced to two turns per day.
Mini-implant Assisted Slow Palatal Expansion (MASPE)68–70
Rapid expansion techniques with hybrid MARPE involving 2-3 activations per day (0.4-0.6 mm/day) have gained popularity for overcoming increased skeletal resistance in adult patients. However, this rapid rate of expansion can cause undesirable side effects, including dental tipping, deformation, or loosening of connecting wires and miniscrews, potential cranial complications such as pterygoid deformations, infraorbital numbness, and even cranial fractures, often leading to the need for surgical intervention. To mitigate these complications, slow expansion protocols have been recommended. A more recent advancement, the MASPE or force-controlled activation protocol—known as the Force Control PolyCyclic (FCPC) protocol—utilizes bone-borne expanders such as the Micro4-expander and PowerScrew, activated slowly with controlled forces limited to 100-120 N using a torque wrench of 400-500 cN. The protocol incorporates a twice-daily “expansion–contraction” cycle, where expansion is followed by six reverse turns to eliminate the expansion force, thereby stimulating sutural remodeling while minimizing undesirable dental and skeletal effects.
Factors Affecting Success with MARPE
Published studies have reported that the success rate of MARPE ranges between 84% and 87%.34, 71, 72 Several factors have been identified as potential predictors of MPS separation with MARPE. 67 Among these, age, palate length, and MPS maturation stage show a negative correlation with successful expansion, whereas vertical and sagittal skeletal patterns, MPS density ratio, and sex do not appear to have a significant association with suture separation. 73
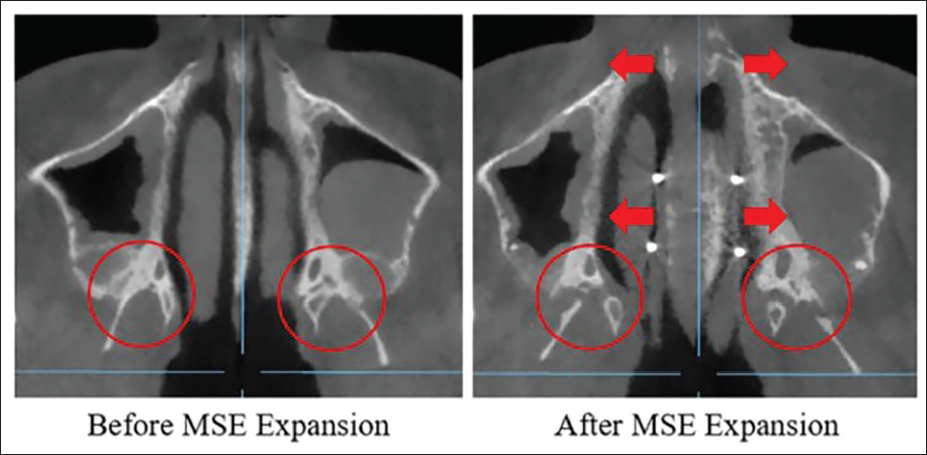
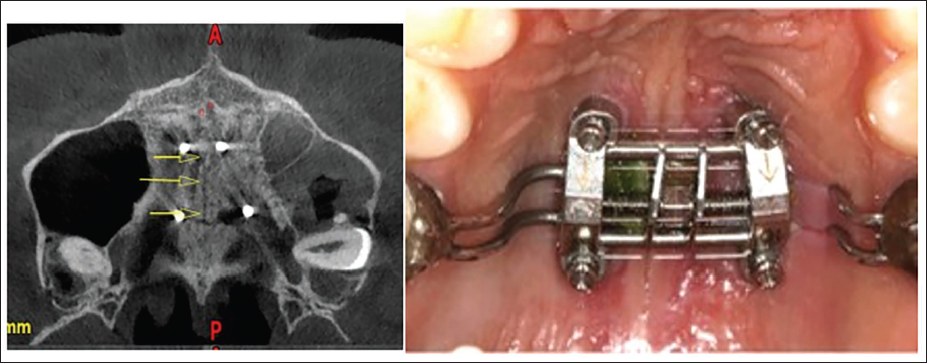
In another study, 50 MPS maturation was again shown to be negatively correlated with suture opening. However, Cantarella et al., 32 through a retrospective evaluation of 15 patients, found that age was not a determining factor for successful suture separation with MARPE. They also observed that the pterygopalatine suture separated following MARPE treatment and concluded that maxillary expansion may be restricted if the pyramidal process does not fully disengage from the pterygoid plate (Figure 21).
Pterygopalatine Suture Disarticulation and Complete Disengagement of the Pyramidal Processes of the Palatine Bones from the Pterygoid Plates with Successful Miniscrew-Assisted Rapid Palatal Expansion (MARPE).
In cases exhibiting asymmetric expansion, variations in the geometry of the zygomatic arches, 32 and differences in frontomaxillary suture separation, 74 have been suggested as influencing factors. Thus, bone density, sutural maturation, and the structural complexity of the midfacial region appear to be important predictors of successful maxillary expansion.
At present, the determinants of success for MSE or any form of MARPE are not clearly established due to the numerous variables involved, and current protocols are largely guided by clinical experience and professional judgment. Further research in this area remains essential.
Failure of the MPS opening is more common in patients older than 25 years, with 67% of such failures occurring in males. As a general clinical guideline, MARPE tends to fail more often in males beyond their mid-20s, whereas it may still succeed in females up to their mid-30s. 75
A significant factor related to the possibility and extent of successful suture opening even in matched patients may be the inherent morphological variability of the craniofacial structures among patients, in terms of skeletal patterns, bone size and density, bilateral symmetry, suture orientations, and surface areas of the suture interface, soft tissue, and muscular constraints. These affect the force trajectories that are created upon expander activation and the effects thereof. These areas have not been researched adequately till date. 76
Supplemental Procedures to Improve Success with MARPE
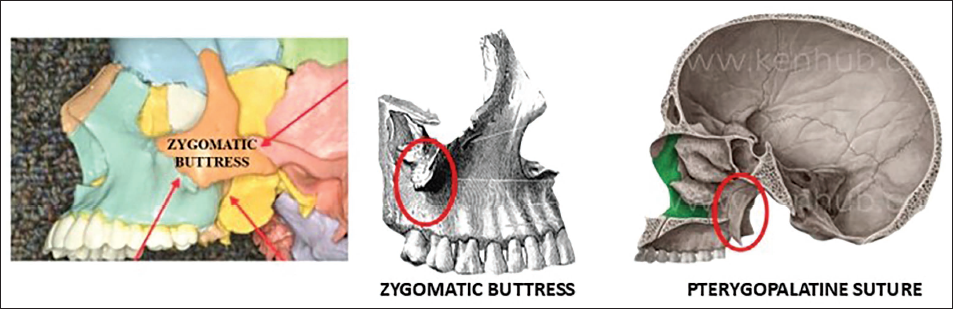
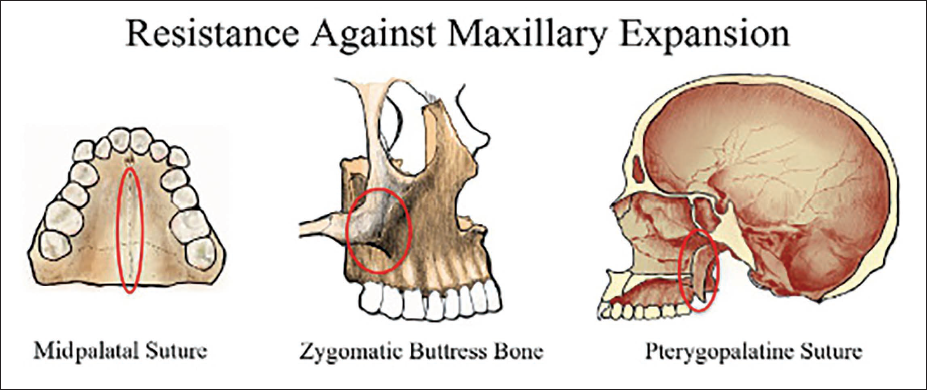
The major sources of resistance to palatal expansion include the zygomatic buttress, the pterygopalatine suture, the MPS (Figure 22), and other perimaxillary sutures. Supplemental procedures designed to enhance the success rate of MARPE primarily focus on reducing these areas of resistance.
The Sources of Major Resistance to Palatal Expansion.
Two such techniques are corticopuncture (Figure 23) and minimally invasive surgical and miniscrew-assisted rapid palatal expansion (MISMARPE).77, 78 These adjunctive procedures aim to facilitate easier suture opening and improve skeletal response during expansion.
Corticopuncture Done to Assist in Maxillary Expansion.
Suzuki et al. reported a successful case of MPS separation in an adult patient following corticopuncture, after a previous attempt with conventional MARPE had failed to achieve suture opening. 78
Airway Implications
Since MARPE has demonstrated greater efficiency in expanding the bony maxilla compared to conventional RPE, it is anticipated to be more effective in widening the airway as well. However, the airway’s structure and function depend not only on the bony framework but also on the surrounding soft tissues. Therefore, the influence of MARPE on airway enlargement and improvement in breathing function should be interpreted with caution.
Expansion of the bony maxilla can alter the tension, contour, and configuration of the soft tissues within the nasal cavity and nasopharynx, potentially affecting adjacent soft tissue structures in the oropharynx and laryngopharynx, which are both anatomically and functionally interconnected. These effects may occur immediately or develop gradually due to the adaptive response period required for soft tissue remodeling.79–82
Further comprehensive studies, incorporating both subjective assessments and objective measurements of airway function, are essential to accurately evaluate MARPE’s impact on patients with respiratory issues and to identify which patients are most likely to benefit from the procedure.
Complications75, 83
Inflammation of the soft tissues surrounding the appliance.
Asymmetric expansion or unfavorable fracture patterns (“bad splits”).
Infection and necrosis of the bone or mucosa adjacent to the implants.
Hypertrophy of the palatal mucosa (Figure 24).
Ulceration of the palatal mucosa.
When performed along with corticopuncture—possible submucosal hematoma and swelling.
Breakage or distortion of the jackscrew (Figure 24).
Tipping of the miniscrews.
Miniscrew migration or fracture (Figure 24).
Complications with Miniscrew-Assisted Rapid Palatal Expansion (MARPE)—Tissue Hypertrophy, Jackscrew Distortion, and Miniscrew Migration.
Contraindications 54
Extremely narrow palatal vault—in such cases, a customized MARPE fabricated using CAD-CAM technology may be considered as an alternative.
History of midfacial trauma.
Very thick or dense palatal bone and/or dense zygomatic buttress bone.
Very thin palate with poor bone density.
Unfavorably shaped palatal tori that interfere with proper MSE placement.
Severe skeletal asymmetry leading to uneven or canted force vectors.
Stability
Long-term stability data for MARPE are limited. In one study with a mean follow-up period of 30.2 ± 13.2 months, both skeletal and dental expansions remained stable, showing less than 0.5 mm of change, and no significant alteration in maxillary clinical crown heights—indicating favorable periodontal health and maintenance of expansion. 72 Similarly, another study evaluating patients 1 year post-expansion reported stable skeletal and dental outcomes. 71 However, comprehensive data on long-term follow-up, retention, and retention protocols after MARPE are still insufficient and require further investigation.
Conclusion
MARPE has proven to be an effective approach for the correction of transverse maxillary deficiencies. With a reported success rate of approximately 87%, it offers patients a relatively comfortable experience. Research indicates that MARPE is generally well tolerated, with only a mild and temporary reduction in Oral Health-related Quality of Life (OHRQoL) during the active expansion phase, which returns to baseline levels following completion of treatment.
In summary, MARPE represents a significant advancement in orthodontic therapy, providing greater skeletal expansion, reduced dental side effects, improved stability, and shorter overall treatment durations compared to traditional methods (Figure 25). As advocates of evidence-based clinical practice, we support the incorporation of MARPE into orthodontic treatment protocols to enhance patient outcomes and satisfaction in addressing maxillary transverse discrepancies (Figure 26 and Table 1).
Miniscrew-Assisted Rapid Palatal Expansion (MARPE) Represents a Valuable Advancement in the Correction of Maxillary Transverse Deficiency.
Integration of Miniscrew-Assisted Rapid Palatal Expansion (MARPE) into Orthodontic Protocols to Optimize Patient Outcomes.
Current Consensus on Miniscrew-Assisted Rapid Palatal Expansion (MARPE).
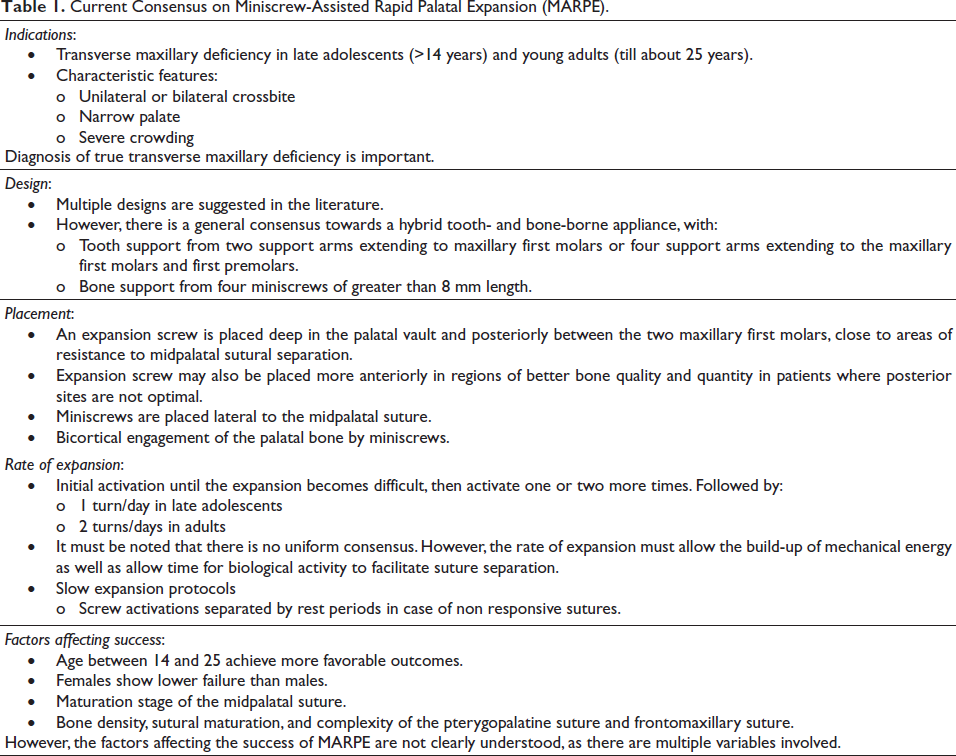
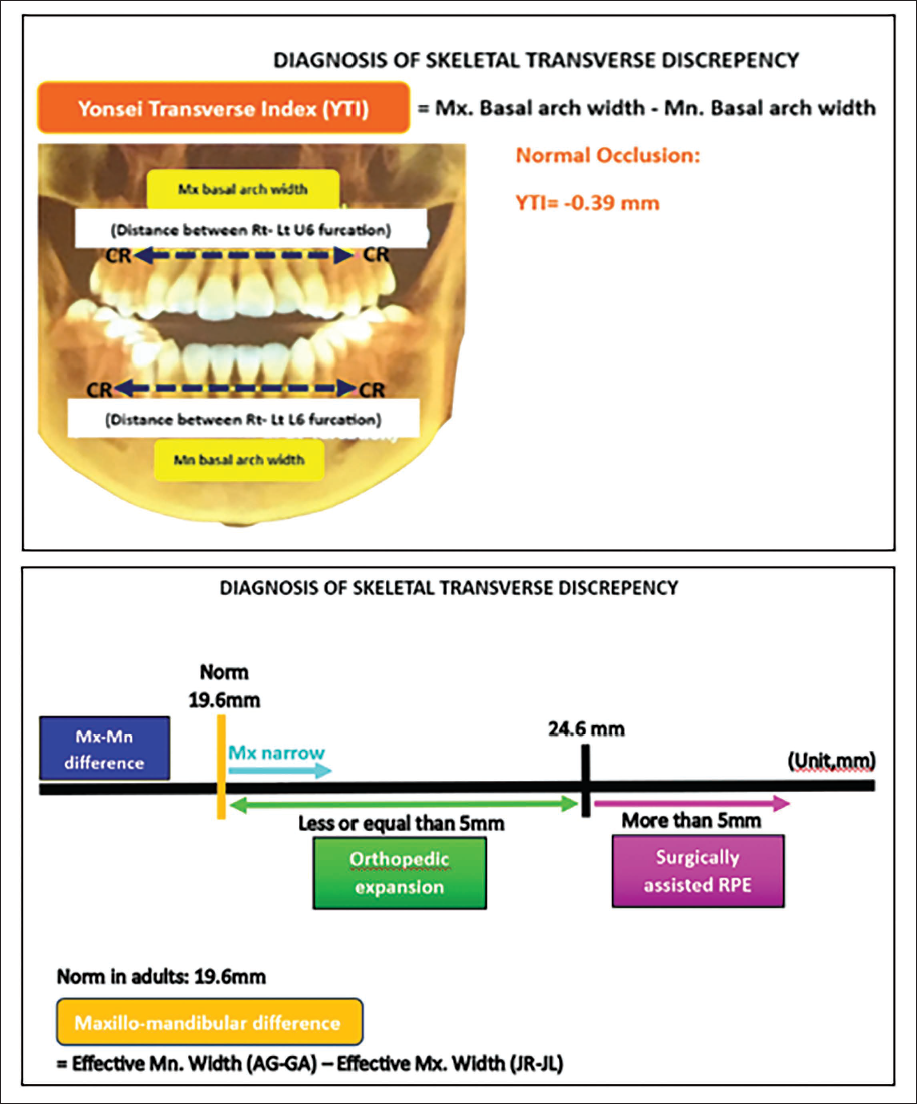
However, it is crucial to emphasize that MARPE, despite its advantages, is sometimes inappropriately applied, particularly in cases where the maxillo-mandibular differential is less than 19.6 mm. 84 Accurate diagnosis of true skeletal transverse discrepancies, based on the center of resistance of the posterior segments, remains essential for ensuring proper case selection and achieving predictable treatment results (Figure 27). 85
Diagnosis of True Skeletal Transverse Discrepancy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This narrative review did not require any informed and ethical consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.