
Abstract
Aim
To compare the maximum removal torque (MRT) of orthodontic miniscrews inserted using a manual driver versus a contra-angle motor-driven method.
Material and Methods
Forty self-drilling, tapered orthodontic mini-implants (8 mm length, 1.65 mm diameter) were inserted into artificial bone blocks without predrilling. Twenty were placed using a manual driver and 20 with a motor-driven contra-angle driver (40 rpm), all at a 90° angle. MRT was measured using a digital torque gauge. Statistical analysis was performed using the paired t-test (P < .05) in International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) v24.0.
Results
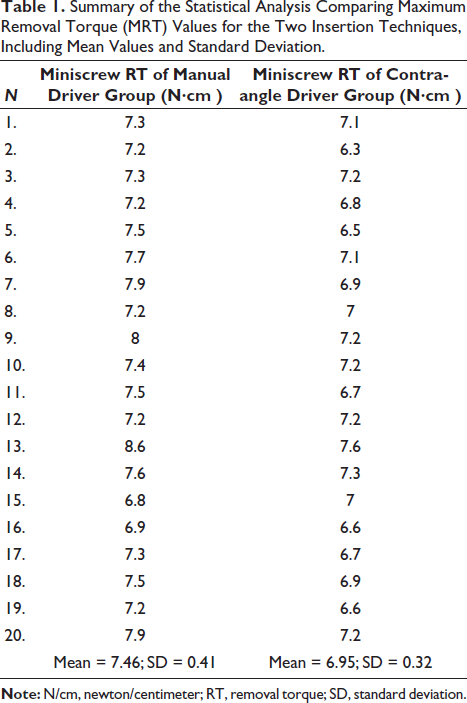
The mean MRT was 7.46 N·cm for the manual insertion group and 6.95 N·cm for the contra-angle driver group. The difference of 0.51 N·cm was statistically significant (P < .0001). MRT values ranged from 6.8 to 8.6 N·cm in the manual group and 6.3-7.6 N·cm in the contra-angle group.
Conclusion
Manual insertion yielded a higher average MRT than the contra-angle driver, with the difference being statistically significant. This suggests a potential clinical advantage of manual insertion in achieving greater primary stability.
Introduction
Anchorage in orthodontics refers to the resistance to undesired tooth movement caused by reciprocal forces. Achieving maximum anchorage is essential when treatment goals demand minimal or no movement of certain teeth. Over the years, several appliances, such as headgear, transpalatal arch (TPA), and the Nance button, have been employed to reinforce anchorage. However, temporary anchorage devices (TADs), introduced in the early 1990s, have become the most effective and patient-friendly method. These small titanium screws, typically 1.2-2.0 mm in diameter and 6-12 mm in length, are temporarily fixed to the bone and provide versatile clinical applications in orthodontic treatment.1, 2
Several factors influence the stability of TADs, with insertion torque (IT) and removal torque (RT) being particularly important. IT measures the rotational resistance during the insertion of the miniscrew into the bone, with higher values indicating stronger mechanical engagement.3, 4 RT, on the other hand, refers to the torque required to unscrew the miniscrew, directly reflecting its anchorage strength and stability.5, 6, 7 Correct insertion is crucial because most failures occur in the early phase after placement. Thus, torque-based evaluations provide valuable insights into the mechanical stability of miniscrews at the bone interface.8, 9
Previous studies have compared miniscrew stability using hand-driven and machine-driven insertion methods.10, 11 However, no study to date has directly compared the RT of miniscrews inserted manually with a hand driver versus a contra-angle motor-driven screwdriver. Understanding this comparison may help clinicians choose the most reliable technique for achieving optimal primary stability. Therefore, the present study aims to evaluate and compare the RT of miniscrews placed using these two insertion methods. The null hypothesis was that there would be no significant difference in RT between the techniques.
Materials and Methods
All insertions were performed by a single inexperienced operator at a 90° angle to the surface of the bone blocks. The use of an inexperienced operator was intentional in order to minimize bias introduced by personal technique and to better reflect real-world clinical conditions, where many operators may be at different stages of their learning curve. Placement at a 90° angle was selected to ensure standardization across all samples, eliminate variability from insertion angulation, and allow a more reliable comparison of RT between the two methods. Forty self-drilling, tapered orthodontic mini-implants (length: 8 mm, diameter: 1.65 mm) were obtained from a single manufacturer (Dentaurum GmbH & Co. KG, Turnstr. 31, 75228 Ispringen, Germany) to avoid variability due to differences in design or alloy composition.
The miniscrews were inserted into standardized artificial bone blocks (Sawbones, Pacific Research Laboratories, Vashon, WA, USA) without predrilling. All insertions were performed by a single inexperienced operator at a 90° angle to the surface of the blocks. The use of an inexperienced operator was intentional in order to minimize bias introduced by personal expertise and to better reflect real-world conditions, where clinicians may be at different stages of their learning curve. Placement at 90° was chosen to ensure consistency across all samples, eliminate angulation variability, and allow a reliable comparison of RT values between the two insertion methods.
The artificial bone blocks consist of rigid polyurethane foam with a density conforming to American Society for Testing and Materials (ASTM) F1839 specifications (ASTM F1839-08). Each block had a two-layer structure: a 2 mm cortical layer (40 PCF) over a 40 mm trabecular layer (20 PCF). The blocks were oriented so that the layers were aligned parallel to the axis of screw insertion.
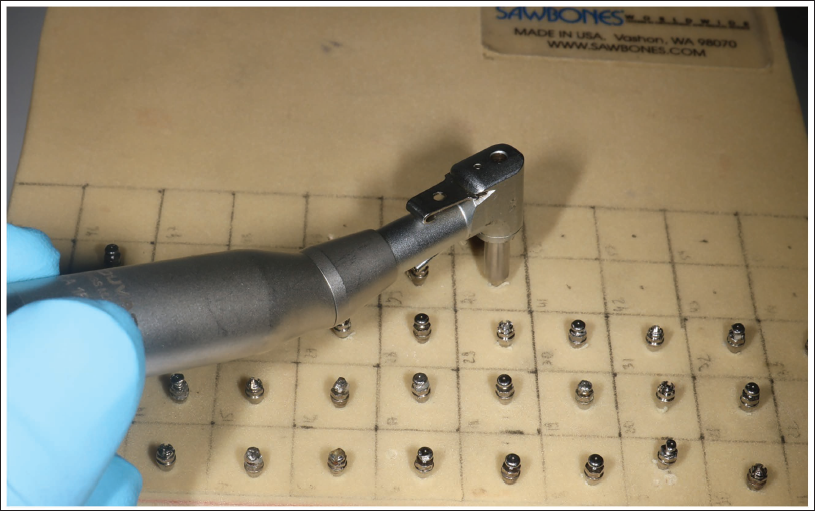
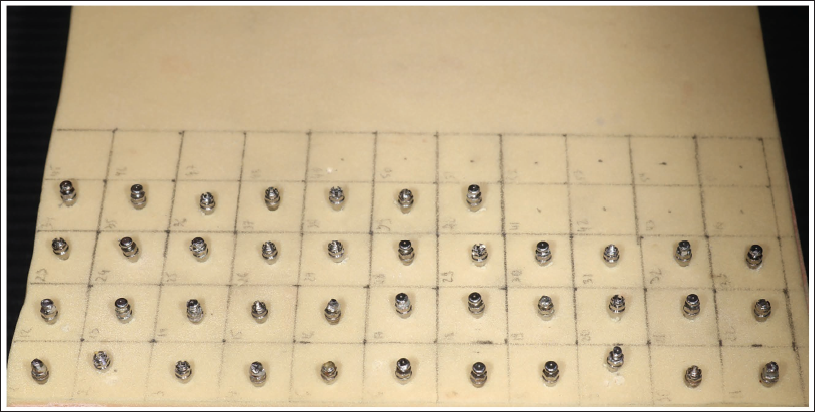
The 40 miniscrews were randomly allocated into two equal groups (n = 20 each): a manual driver group and a contra-angle driver group. The contra-angle driver was operated at a constant rotational speed of 40 rpm, using a torque-controlled motor unit. In both groups, insertion was continued until the screw head was flush with the cortical surface (Figures 1 and 2).
Insertion of Miniscrews into Artificial Bone Blocks Using a Contra-angle Driver. The Image Demonstrates the Insertion Process Performed at a 90° Angle to the Bone Surface.
A Total of 40 Miniscrews were Inserted into Artificial Bone Blocks, Categorized by Insertion Method: Manual Driver (20 Miniscrews) and Contra-angle Driver (20 Miniscrews).
After insertion, the miniscrews were removed by the same operator, and the maximum removal torque (MRT) was recorded simultaneously using a digital torque gauge (Tapha Tools, Taiwan; certified according to ASME B107.300-2010 and ISO 6788.2003) (Figure 3). The device had an accuracy of ±0.5% and was calibrated and certified by the ITRI — Industrial Technology Research Institute (Figure 3).
Comparison of the Mean Removal Torque (MRT) Between Miniscrews Inserted with a Manual Driver and Those Inserted with a Contra-angle Driver, Expressed in Newton-centimeters (N·cm).

Since the study was conducted entirely on artificial bone blocks and did not involve human participants or animals, no ethical committee approval was required.
Statistical Analysis
Statistical analysis of the measurements was performed using International Business Machines (IBM) Statistical Package for the Social Sciences (SPSS) Statistics v24.0 (IBM Corp., Armonk, NY, USA). The Shapiro–Wilk test was used to assess the normality of the data distribution. Levene’s test was applied to evaluate the homogeneity of variances between the groups. Descriptive statistics, including the mean, standard deviation, minimum, maximum, and range of RT values, were calculated for each group. Frequency observations were also noted in cases where RT in the manual group was equal to or lower than that in the contra-angle group.
For inferential analysis, a unpaired t-test was performed to compare the mean values between the two insertion methods. In addition, the effect size was calculated using Cohen’s d to quantify the magnitude of the observed difference. A P value of less than .05 was considered statistically significant.
Results
For both groups, the Shapiro–Wilk test confirmed the normal distribution of data (P > .05). Levene’s test indicated no significant difference in variance between the groups (P > .05).
The mean removal torque (MRT) for the manual driver group was 7.46 ± 0.45 N·cm (95% CI: 7.25-7.67), while the contra-angle driver group showed a mean MRT of 6.95 ± 0.36 N·cm (95% CI: 6.78-7.12). The mean difference between the two groups was 0.51 N·cm, which was statistically significant (P < .0001).
In the manual driver group, MRT values ranged from a minimum of 6.8 N·cm to a maximum of 8.6 N·cm. In the contra-angle group, values ranged from 6.3 to 7.6 N·cm. Despite some overlap between groups, manual insertion generally yielded higher values; in only 2 of 20 cases (10%), the contra-angle IT was equal to or exceeded that of the manual method.
The calculated effect size (Cohen’s d) was 1.29, indicating a large effect in favor of the manual insertion method.
Table 1 presents the detailed descriptive statistics and group comparisons.
Summary of the Statistical Analysis Comparing Maximum Removal Torque (MRT) Values for the Two Insertion Techniques, Including Mean Values and Standard Deviation.
Discussion
RT reflects the quality of the bone-implant interface and serves as a direct indicator of primary stability. 6 In this study, manually inserted miniscrews demonstrated significantly higher MRT than those placed with a contra-angle driver, suggesting stronger mechanical interlocking with bone.
The observed difference may be explained by the nature of the techniques. Manual insertion allows controlled, gradual pressure and tactile feedback, potentially leading to improved bone compression and stability. In contrast, even at low speed (40 rpm), the contra-angle driver applies more rapid mechanical force, which may reduce bone-implant contact and primary stability. Previous research also highlighted that the insertion technique influences stability, though findings remain controversial. Novsak et al. reported higher primary stability with manual insertion, while Kim et al. observed greater success rates with engine-driven insertion.10, 12 Our results align with studies emphasizing the advantages of controlled manual placement.
The absolute MRT values in our study (7.46 N·cm for manual vs. 6.95 N·cm for motor-driven) were lower than those reported in clinical studies.5, 8, 13 This discrepancy is expected, as our experiments were performed on artificial bone blocks without osseointegration, which, in vivo, can significantly increase RT.14, 15
Overall, manual insertion appears to provide superior stability, though it is influenced by operator skill and variability. Mechanical drivers, while more standardized, may compromise tactile control. Future studies should investigate how insertion angle, screw geometry, and clinical conditions further affect RT and long-term stability.
Conclusion
The study rejected the null hypothesis, demonstrating a statistically significant difference in RT. Miniscrews placed with a manual driver exhibited higher MRT compared to those placed with a motor-driven method. However, the motor-driven method remains a viable option for inexperienced clinicians, offering more stable insertion forces and speed.
This study was conducted using artificial bone blocks, where osseointegration does not occur; therefore, the results may differ under clinical conditions. In addition, all miniscrews were inserted at a 90° angle to standardize conditions, which may not reflect the variety of angulations used in clinical practice. These limitations should be considered when interpreting the findings.
Future studies should explore the long-term clinical outcomes associated with each insertion technique, including the effects of osseointegration, angulation, and patient-specific bone quality, to provide a more comprehensive understanding of their practical implications across clinical settings.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
This study did not involve human participants or identifiable data; therefore, ethical approval and informed consent were not required in accordance with institutional and national guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.