
Abstract
Introduction:
Correction of Class II has become a routine with the introduction of mini-implants.
Objective:
The objective of the study was to evaluate the clinical efficiency of bone-anchored intraoral bodily molar distalizer (BAIBMD) as compared to bone-anchored pendulum appliance (BAPA).
Materials and Methods:
This split-mouth study included 11 subjects (6 boys and 5 girls) who required molar distalization. BAPA constructed on one side and BAIBMD on the other side. Both the appliances were anchored to the bone, using a single 2 × 8 mm titanium mini-screw placed in the anterior para-median region of the mid-palatal suture with its head embedded into the Nance button during construction. The force delivery mechanism on both the sides consisted of 200 g-force application, using an activated 0.032˝ titanium molybdenum alloy (TMA)[A]:Author: Please provide expansion for “TMA.” springs fabricated with respective designs and inserted into the lingual sheaths of the first molar bands. The rate, duration, and nature of tooth movement for both the sides were compared. Descriptive statistics for various parameters were analyzed using Wilcoxon signed-rank test.
Results:
Clinically successful distalization was achieved on both sides. No statistical difference was found in the rate of distalization. Differences in the treatment duration between the two groups were statistically significant, with less duration taken for distalization with BAPA. Statistically significant molar tipping was observed in BAPA.
Conclusion:
While both the appliances provided a similar rate of distalization, BAIBMD took more duration than BAPA but produced a predominantly translatory type of distal tooth movement.
Introduction
Correction of Angle’s Class II malocclusion sometimes requires distalization of maxillary molars, creating necessary space to address the problem. Pendulum appliance 1 is often the appliance of choice for distalization because of its ease of fabrication and cost-effectiveness. Obtaining proper translatory type of tooth movement during distalization is difficult with pendulum appliance. Intraoral bodily molar distalizer was introduced by Keles and Sayinsu 2 to overcome the predominant tipping nature of the tooth movement achieved with the pendulum appliance.
The challenge often faced during distalization is the loss of anchorage, which is undesirable. Konomi 3 described the application of mini-implants for orthodontic anchorage. The advent of skeletal anchorage has led to the development of distalization appliances, which leverage the anchorage potential of mini-implants placed in the palatal bone. Kircelli et al, 4 Escobar et al, 5 Oncag et al, 6 and Polat-Ozsoy et al 7 described an application of skeletal anchorage with pendulum appliance. Chung et al 8 used segmented wire mechanics with mini-implant for molar distalization. Konomi 3 used miniplate fixation screws for anchorage.
The use of skeletal anchorage along with intraoral bodily molar distalizer would provide the additional advantage of preventing anchorage loss in the anterior segment while bringing a predominantly translatory type of tooth movement. Such a design was not described earlier in the literature. We incorporated a mini-implant in the design of bodily molar distalizer and named it bone-anchored intraoral bodily molar distalizer (BAIBMD). The present study was carried out to evaluate the efficiency of BAIBMD as compared to bone-anchored pendulum appliance (BAPA). The null hypothesis stated was that there is no difference in the efficiency of BAIBMD and BAPA.
Materials and Methods
This split-mouth study initially included 11 subjects (6 boys and 5 girls) who required molar distalization. The study was approved by the Institutional Ethical Committee (No: XXXX/IEC/2012/07) and by the Institutional Research Board (No: XXXX/IRB/1407). The subjects were selected from patients reporting to the Department of Orthodontics, based on the following selection criteria, after obtaining the patient consent.
Inclusion Criteria
The following criteria were included in the study:
Angle’s Class II molar relation bilaterally (> 3 mm);
13- to 16-year-old male or female patients with erupted or partially erupted II molars and showed the presence of developing third molars on orthopantomograph;
horizontal or average growth pattern (SN-Go-Gn);
good oral hygiene; and
no history of previous orthodontic treatment.
Exclusion Criteria
The following criteria were excluded from the study:
uncooperative patients;
medically compromised patients; and
vertical growth pattern.
All patients and parents were informed about the procedure, and signed consent was taken. Pre-treatment photographs, study models, and cephalograms were taken for all the subjects.
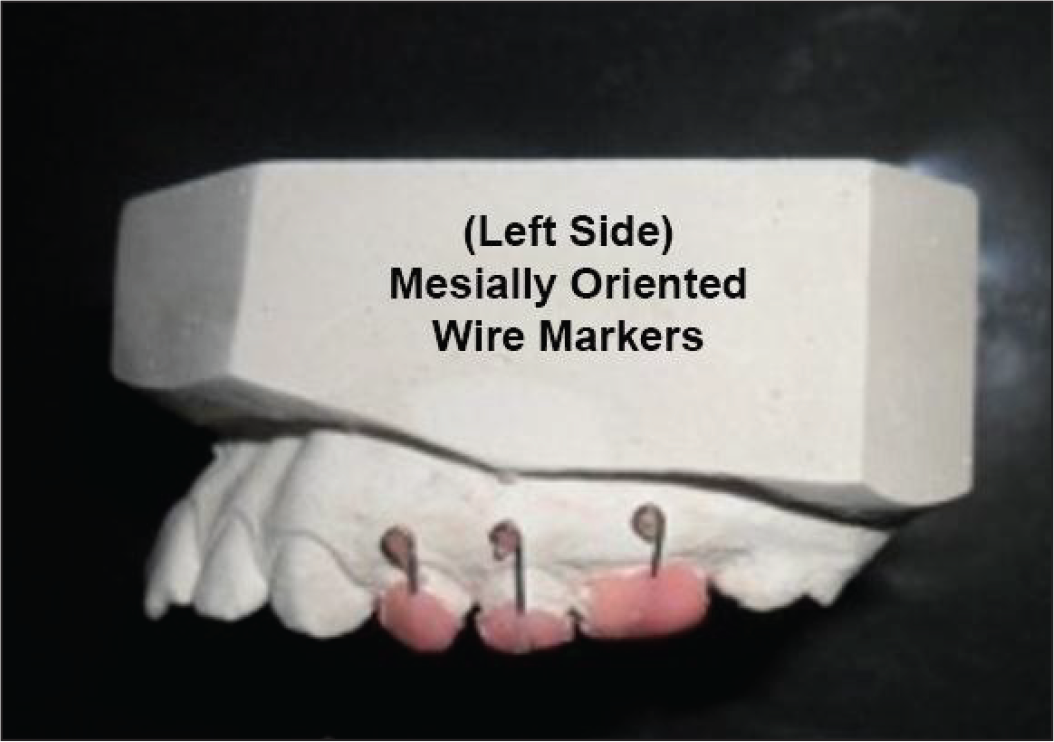
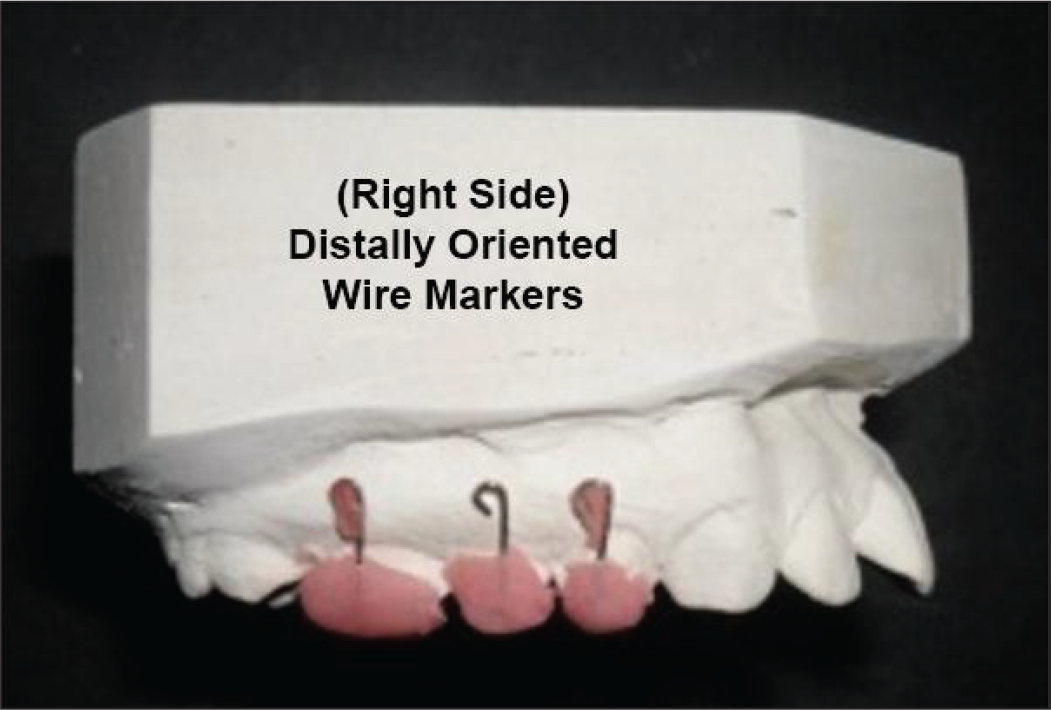
Titanium mini-screw (2 × 8 mm, SK Surgicals, Pune, India) was used for skeletal anchorage. 0.032″ Titanium–Molybdenum alloy (Ormco, Orange, CA) wire was used for the fabrication of distalization springs. A mini-screw was placed in the anterior paramedian region of the mid-palatal suture, 7 to 8 mm posterior to the incisive foramen, and 3 to 4 mm lateral to the median line. Along with the mini-implant in place, alginate impressions were made, and stone casts were obtained. Specially fabricated 0.016″ SS wire markers (Figures 1 and 2) were used for the study. These were oriented vertically and retained in acrylic caps, which were made for maxillary first molars, first premolars, and second premolars. The acrylic caps holding the wire markers were cemented temporarily, and a lateral cephalogram was obtained. These wire markers aid in assessing the amount of molar distalization and the extent of tipping movement (molars and premolars) on cephalogram. To differentiate right- and left side segments, as well as to overcome the problem of superimposition on cephalograms, the tips of these wire markers were bent distally and mesially on the right and left side, respectively. After obtaining the cephalogram, these acrylic caps with wire markers were removed from the teeth and stored for their use to aid the same process again after distalization. Molar bands with welded lingual sheaths were cemented on maxillary first molars. Another impression was made with these bands and a mini-implant in place. Stone casts were obtained. On the cast model, the mini-implant head was blocked out with wax to prevent extending acrylic material on to it during Nance button construction.
Distally Oriented Wire Markers on Right Side.
Mesially Oriented Wire Markers on Left Side.

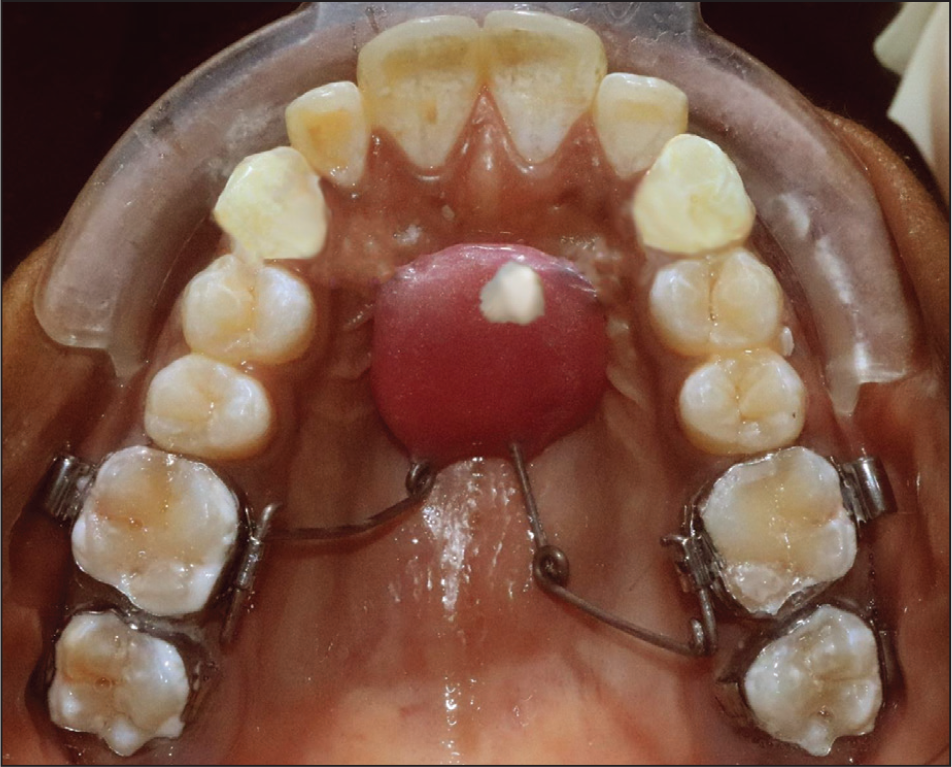
Distalization spring for pendulum appliance was constructed on the right side, whereas distalization spring for bodily molar distalizer was constructed on the left side. The auxiliary wires that extend to the occlusal surface of the first and second premolars in the original design of the pendulum appliance were excluded from both sides, taking into consideration the nature of skeletal anchorage being employed in the current design. The appliance was seated on the palate, and adaptation was checked clinically. The Nance button was connected to the mini-screw head using composite. The distalization springs were activated parallel to the median palatal suture to generate 200 g of force and inserted into the lingual sheaths on the first molar bands. Schematic diagram of the springs in passive condition and active conditions is presented in Figures 3 and 4. Fabricated appliance seated in the mouth in passive and active conditions is presented in Figures 5 and 6, respectively.
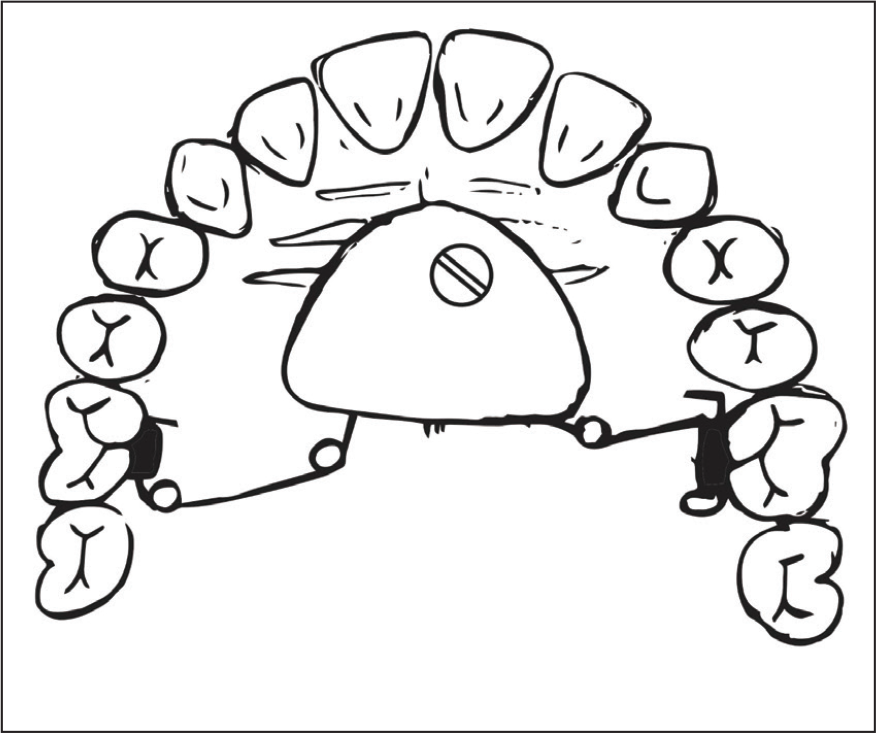
Schematic Diagram of the Springs in Passive Condition.
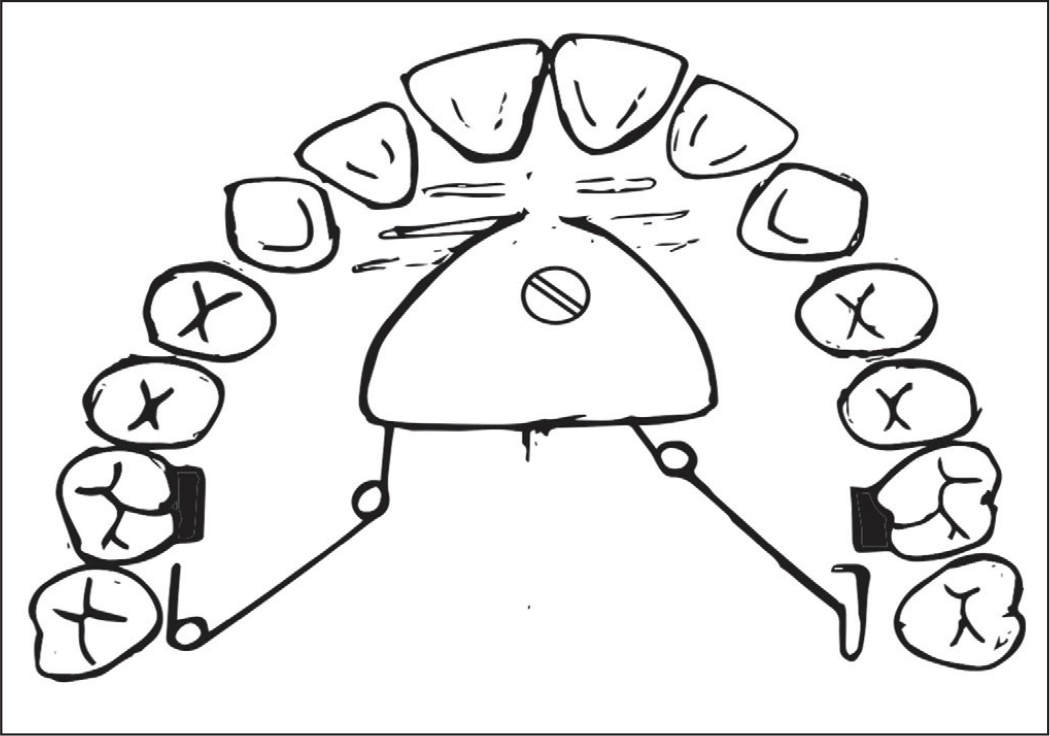
Schematic Diagram of the Springs in Active Condition.

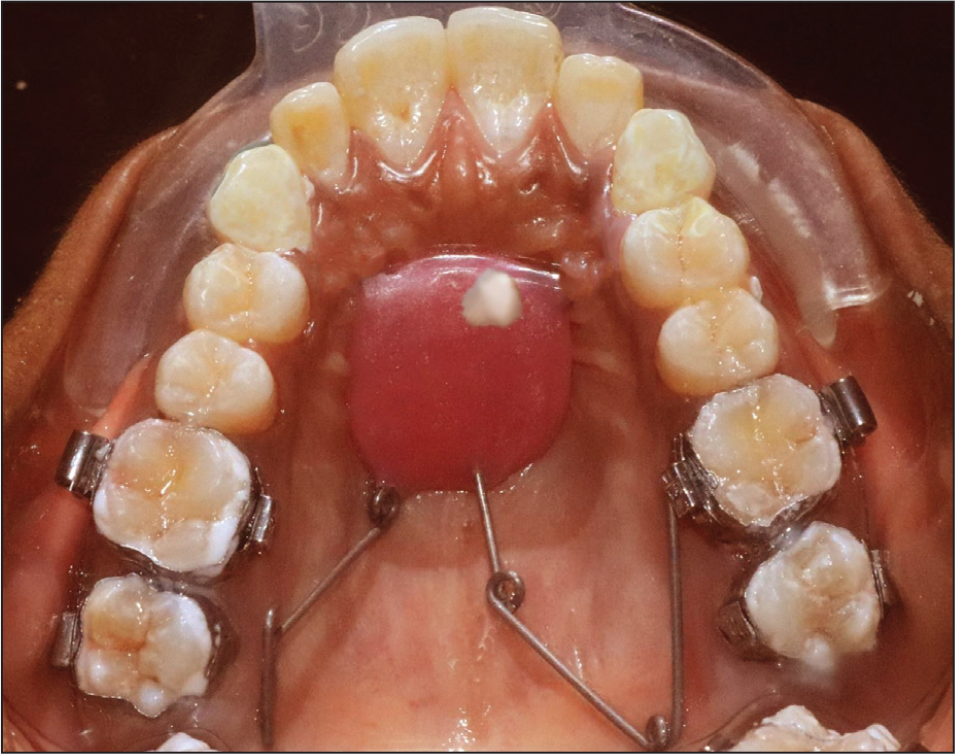
Fabricated Appliance in Passive Condition.

Fabricated Appliance in Active Condition.
Oral hygiene instructions were given to all the patients to keep the appliance and surrounding tissues free of any visible deposits. The patients were recalled at every 4-week interval for follow-up. Force levels were regularly monitored during these visits, and the springs were reactivated, if required. In none of the patients, the mini-screw failure was seen. After achieving the Class I molar relationship, the distalization spring on that side was deactivated and passively reinserted until the other side distalization was complete. Once Class I molar was achieved on both sides, the appliance was removed.
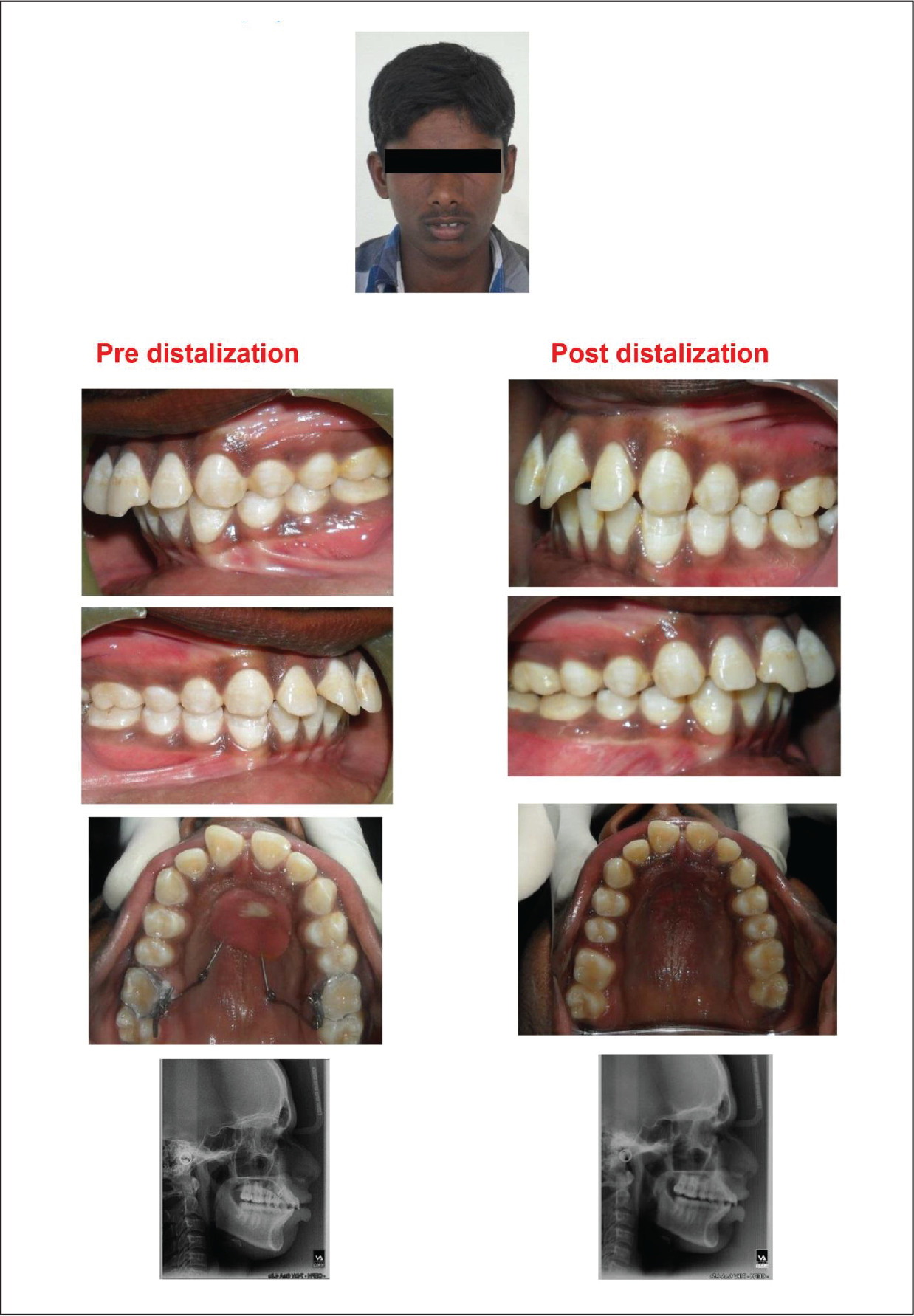
Post-distalization photographs, study models, and lateral cephalograms were taken with the previously stored acrylic caps holding the wire markers. Figures 7 to 10 present pre-distalization records and Figures 11 to 14 present post-distalization records of one subject, whereas the pre- and post-distalization records of two more patients treated by these appliances are presented in Figures 15 and 16. Distalization achieved was stabilized by placing Nance palatal arch which also serves to reinforce anchorage during subsequent mechanotherapy.[A]:Author: The sense of the sentence “Distalization was stabilized…” seems to be unclear. Please, therefore, consider rephrasing the same for better clarity.
Pre-distalization Intraoral Left Side.

Pre-distalization Intraoral Right Side.

Pre-distalization Intraoral Upper Occlusal.

Pre-distalization Lateral Cephalogram.

Post-distalization Intraoral Left Side.

Post-distalization Intraoral Right side.
Post-distalization Intraoral Upper Occlusal.
Post-distalization Lateral Cephalogram.
Pre- and Post-distalization Records of Patient 1.
Pre- and Post-distalization Records of Patient 2.
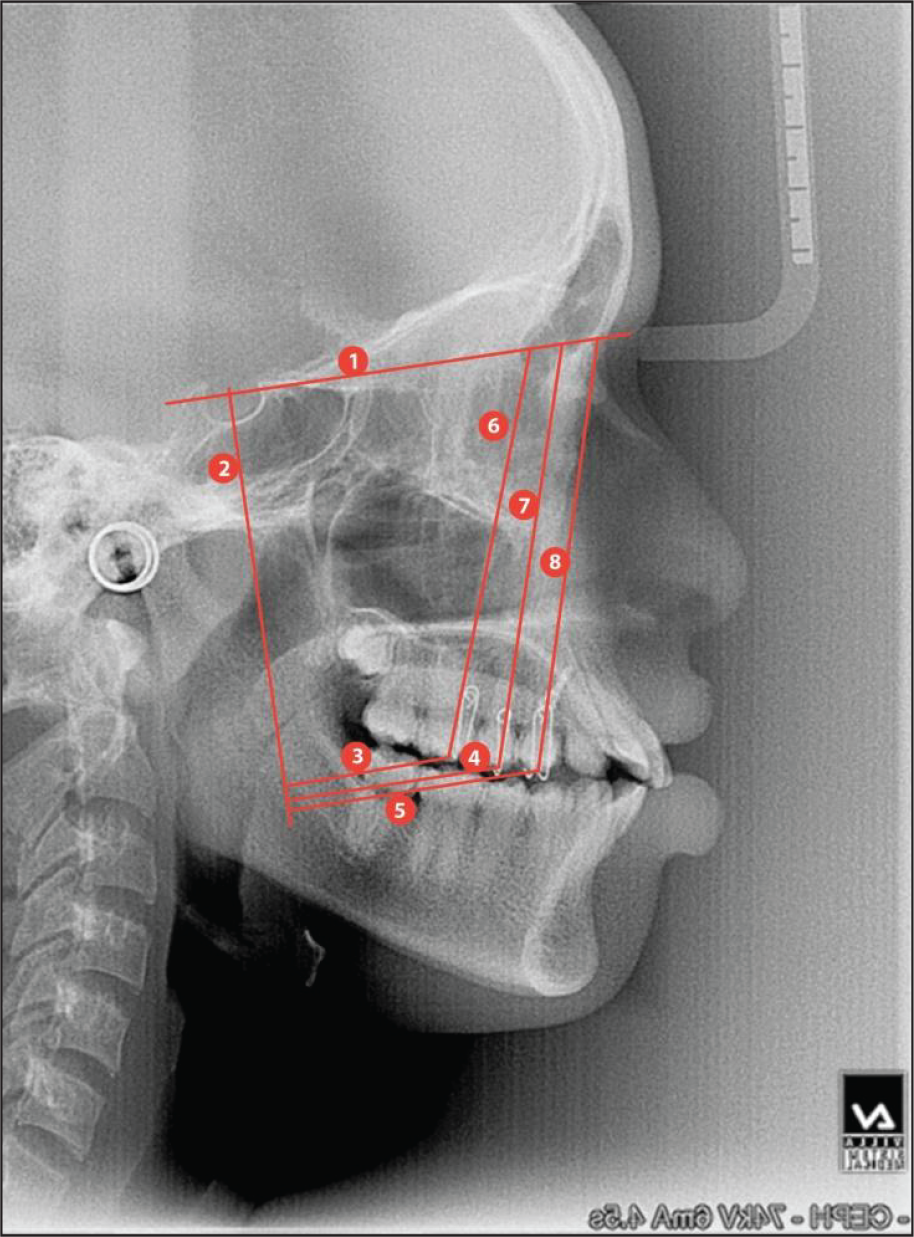
Cephalometric Markings.
Analysis
Pre- and post-distalization cephalograms were analyzed and compared. The orientation of the wire marker is considered as “Long axis,” and apex of the wire marker at the occlusal surface is considered as “cusp tip” for cephalometric parameters. Measurements on pre- and post-distalization cephalograms were performed. Half of the cephalograms were randomly selected, landmarks were identified, and measurements were performed once again by the same operator to check for intra-operator measurement error using Dahlberg’s formula (Se2 = Σd2/2n). There was no statistically significant difference between both the measurements.
The reference planes used to assess the dental parameters are presented in Figure 17:
Horizontal reference line (HR)—Sella–Nasion plane (Figure 17: label 1).
Vertical reference line (VR)—line perpendicular to SN plane at Sella point (Figure 17: label 2).
Linear parameters assessed were:
VR to I molar cusp tip (Figure 17: label 3);
VR to II premolar cusp tip (Figure 17: label 4); and:
VR to I premolar cusp tip (Figure 17: label 5).
Angular parameters assessed were:
Results
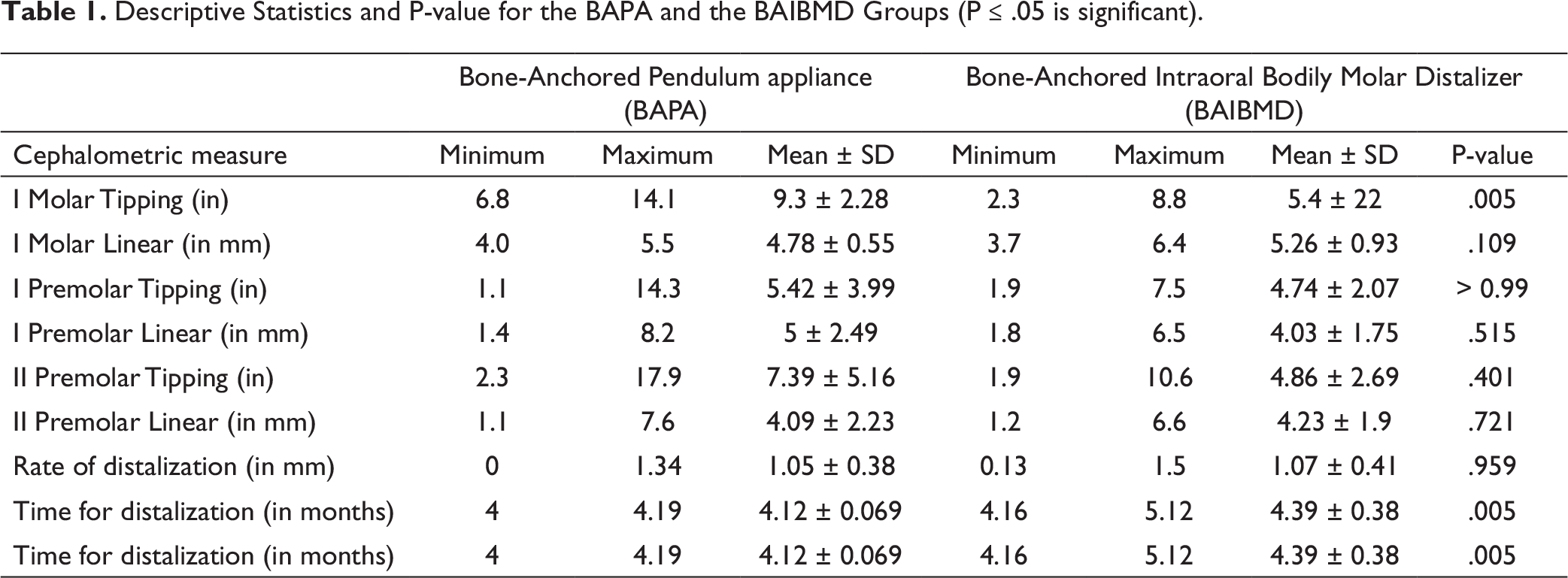
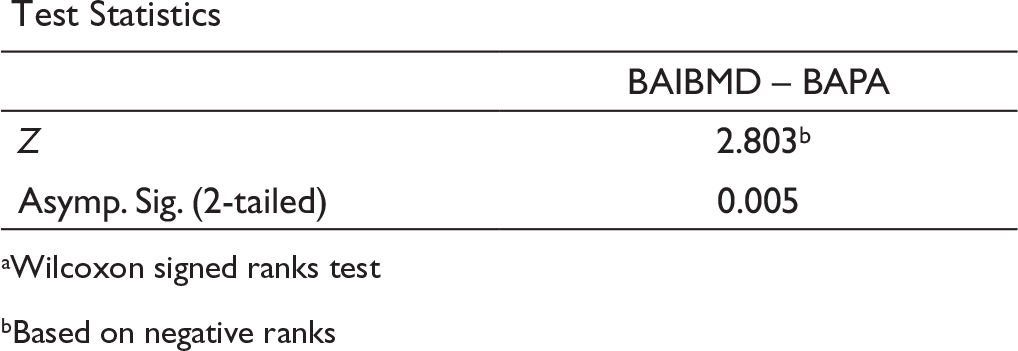
Clinically, successful distalization was achieved in both groups. Descriptive statistics (means, standard deviations) were calculated for the amount of distalization, duration of treatment, tooth angulation, and rate of distalization for both the groups. The descriptive statistics for the BAPA and the BAIBMD groups are shown in Table 1. The descriptive statistics for the linear values, time taken, and angular values of molar distalization are shown in Tables 2, 3, and 4 respectively.
Descriptive Statistics and P-value for the BAPA and the BAIBMD Groups (P ≤ .05 is significant).
Descriptive Statistics of Molar Linear Values.
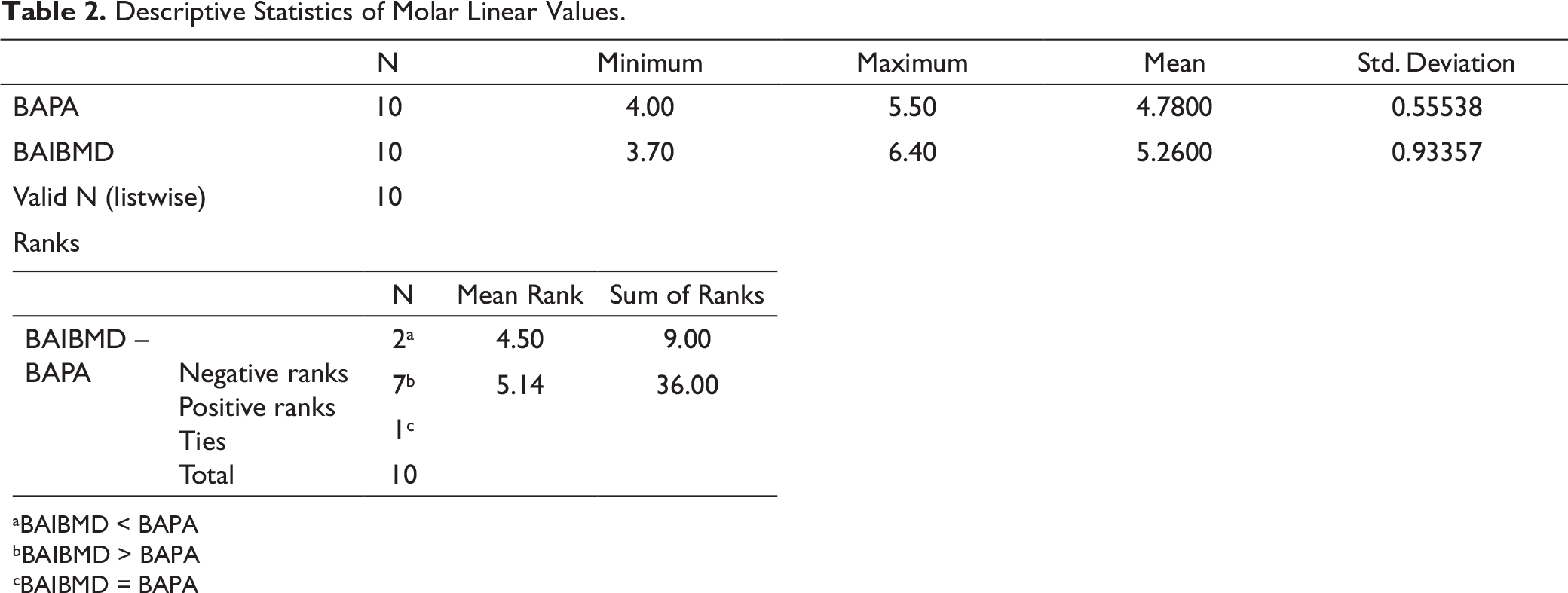
aBAIBMD < BAPA
bBAIBMD > BAPA
cBAIBMD = BAPA
Test Statistics
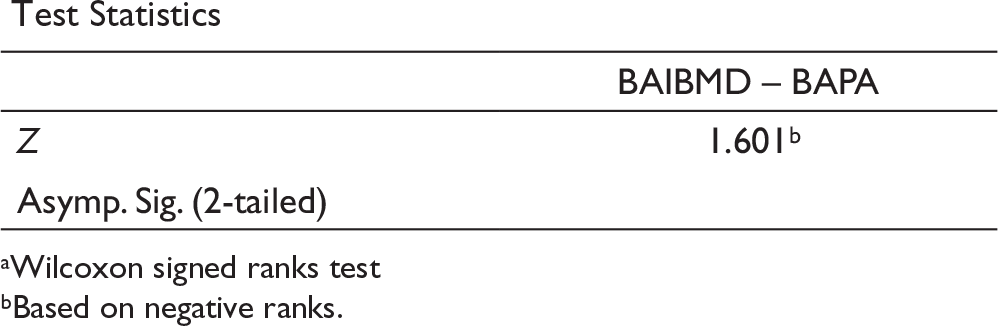
a[A]:Author: Please provide cue for “a” in the tabular column under the heading “Test Statistics” in Tables 2 to 4.Wilcoxon signed ranks test
bBased on negative ranks.
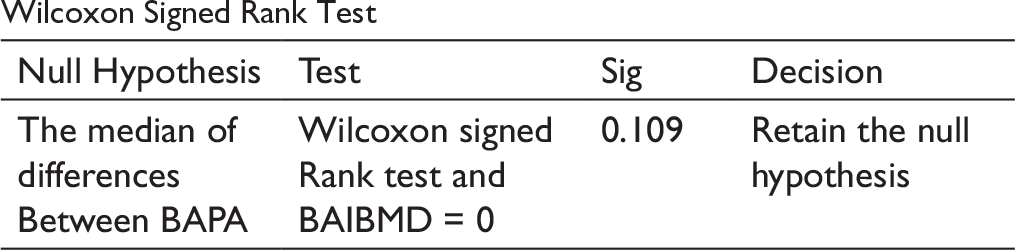
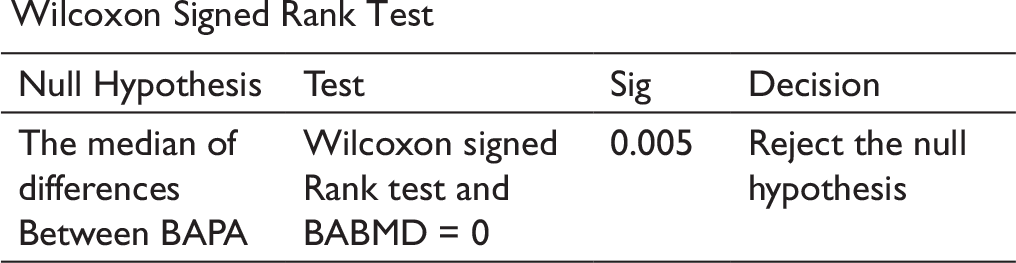
Wilcoxon Signed Rank Test
Wilcoxon Signed Rank Test
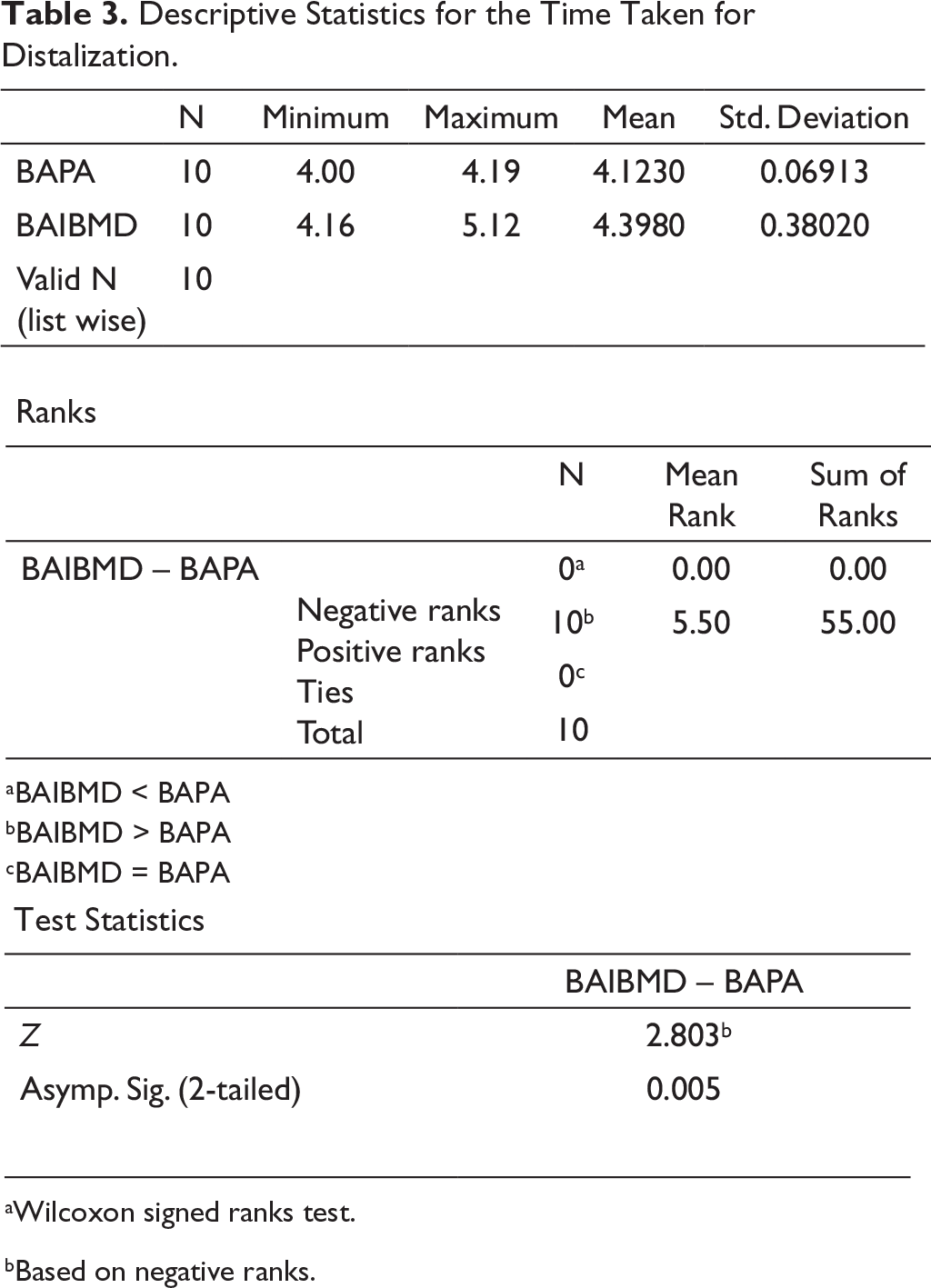
Descriptive Statistics for the Time Taken for Distalization.
aWilcoxon signed ranks test.
bBased on negative ranks.
Wilcoxon Signed Rank Test
Descriptive Statistics for Molar Angular Values.
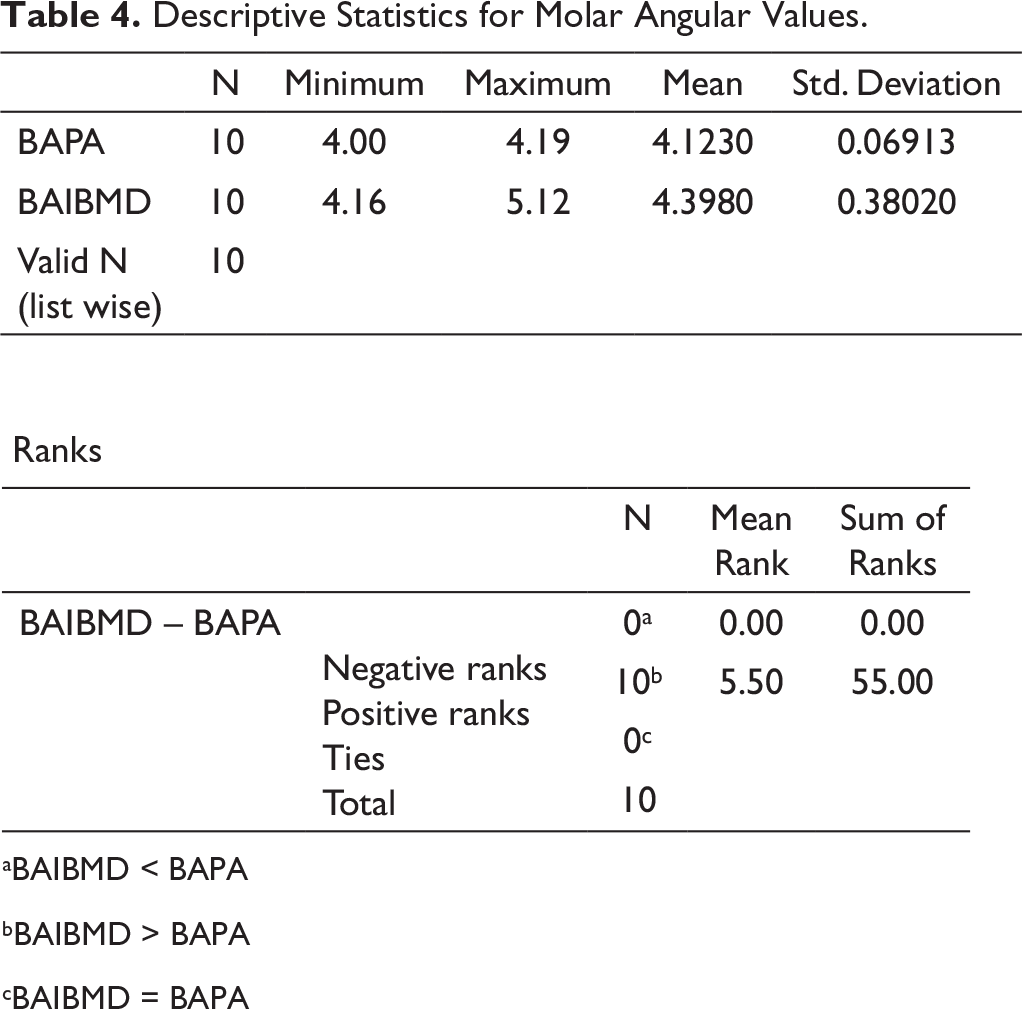
aBAIBMD < BAPA
bBAIBMD > BAPA
cBAIBMD = BAPA
Test Statistics
aWilcoxon signed ranks test
bBased on negative ranks
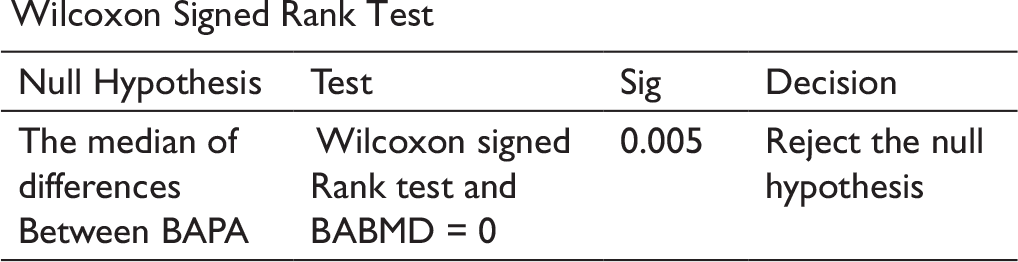
Wilcoxon Signed Rank Test
No statistical difference was found in the rate of distalization. Statistically significant molar tipping was observed in BAPA. The differences in the treatment duration between the two groups were statistically significant. In the BAIBMD group, the maxillary I molar, I premolar, and II premolar distalized by 5.26 ± 0.93 mm, 4.03 ± 1.75 mm, and 4.23 ± 1.9 mm, respectively. In BAPA group, the maxillary I molar, I, and II premolars were distalized by 4.78 ± 0.55 mm, 5 ± 2.49 mm, and 4.09 ± 2.23 mm, respectively. There was no statistical significance between both the groups for I and II premolar distalization (Table 1).
In the BAIBMD group, the maxillary I and II premolars were tipped by 4.74 ± 2.07 degrees and 4.86 ± 2.69 degrees, respectively. In the BAPA group, the maxillary I and II premolars tipped by 5.42 ± 3.9 degrees and 7.39 ± 5.16 degrees, respectively. There was no statistical significance between the groups for I and II premolar angular values (Table 1).
Discussion
Orthodontic treatment involving maxillary molar distalization is one of the means to address Angle’s Class II malocclusion. Appliances chosen for this purpose should be simple to fabricate and provide predictable distalization of maxillary molar without any loss of anchorage in the anterior segments.
The pendulum appliance introduced by Hilgers 1 is a simple appliance that is often used for distalization. The issue of some amount of tipping type of tooth movement achieved by this appliance and considerable unwanted anchorage loss of the anterior segment has been the concern with pendulum appliance. Unwanted round-tripping occurs because once the desired amount of distalization of molars has been achieved, the orthodontist has to again use these molars as anchor units to distalize segments mesial to it, which were the reactive units earlier during distalization.
Keles and Sayinsu 2 introduced intraoral bodily molar distalizer to address the issue of the tipping type of tooth movement associated with the pendulum appliance. While this appliance helped in controlling the type of tooth movement required, the issue of unwanted anchorage loss remains unaddressed.
The introduction of orthodontic mini-implants created new possibilities of bringing desired tooth movements without the concern of losing anchorage. Many applications have been implemented successfully in various orthodontic biomechanical situations, simplifying the previous appliance designs, which needed to depend on the patient’s compliance to leverage extra-oral anchorage.
Anterior paramedian region of the mid-palatal suture, 7 to 8 mm posterior to the incisive foramen and 3 to 4 mm lateral to the median line have been a preferred location for designs incorporating skeletal anchorage for maxillary molar distalization. BAPA 4 was introduced to use the advantage of a skeletal anchorage along with the pendulum appliance. The prospect of employing skeletal anchorage along with the intraoral bodily molar distalizer and evaluating the efficiency of this bone-anchored bodily molar distalizer was the key idea behind this study. This split-mouth study involved a comparison of the newly designed BAIBMD, on the one side, and BAPA, on the other side.
In this study, the maxillary molars in both the groups were distalized to Class I molar relationships without requiring much patient cooperation. The average distalization time to achieve Class I molar relationships was 4.39 ± 0.38 months for BAIBMD group and 4.12 ± 0.069 months for BAPA. The force system offered by the distalization spring design in BAIBMD, which provides simultaneous uprighting and the distal force, could be the reason for the increased average distalization time. Kircelli et al, 4 Pseiner et al, 9 Escobar et al, 5 Oncag et al, 6 and Gelgor et al 10 reported similar average duration for maxillary molar distalization achieved with pendulum appliance anchored by mini-implants.
In the present study, the molars were distalized at an average of 4.5 mm in 4 months in the BAPA group, translating to a rate of distalization of 0.88 mm/month. The rate of distalization was similar in both groups. There was no statistical difference found in terms of the rate of distalization (P > .05). The average amount of molar distalization and distal tipping in BAIBMD group was 5.26 ± 0.93 mm and 5.39 ± 2.2°mm, respectively, whereas the average amount of molar distalization and distal tipping in the BAPA group was 4.78 ± 0.56 mm and 9.3 ± 2.28°mm, respectively. Wilmes and Drescher 11 reported a mean mesial rotation of 3.4 ± 1.2°mm with the Beneslider appliance used.
In the present study, the amount of molar tipping was more in the BAPA group (9.3 ± 2.28 degrees) compared to the BAIBMD (5.39 ± 2.2 degrees). This was statistically significant (P = .05). Joseph and Butchart 12 reported a mean change in molar angulation of 15.7 degrees while using the pendulum appliance. As the distalization force was generated with 60 to 70 degrees posterior activation of the pendulum springs from the crown level and because no control mechanism related to the tipping of the upper molars was present in the BAPA group, distal tipping at the maxillary molars was more. This type of tipping was compensated by an uprighting component of the bodily molar distalizer appliance. Hence, the amount of molar tipping was higher in the BAPA group. Our study also showed that there was a spontaneous distalization of premolars. The average distal movement of the first and second premolars on the BAPA side was 5 mm and 4 mm, respectively, while, on the BAIBMD side, it was 4 mm and 4 mm, respectively. The average distal angulations of the first and second premolars were 5 degrees and 9 degrees, respectively, on the BAPA side, while, on the BAIBMD side, it was 4.9 degrees and 4.5 degrees, respectively. These findings are consistent with the findings of earlier studies of Obeti et al, 13 Byloff and Darendeliler, 14 and Keles and Sayinsu. 2 This distal movement of premolars is reported to be associated with the transeptal fibers in earlier studies of Carano and Testa, 15 Ngantung et al, 16 and Fudalej and Antoszewska. 17 In a study conducted by Cambiano et al, 18 in BAPA, the correction of the Class II molar relationship resulted from a distal movement of 3.45 mm and tipping of 11.24 degrees of the first maxillary molars. In the present study, the BAPA side showed 4.78 mm distalization and 9.3 degrees distal tipping.
About the clinical advantages and disadvantages of the two systems, the fabrication of both appliances was simple. Insertion of the distalization spring in BAPA into the lingual sheath was easier than that of the BAIBMD.
Conclusion
Both BAIBMD and BAPA provided a similar rate of distalization.
BAIBMD group took more duration than BAPA.
BAIBMD produced a predominantly translatory type of distal tooth movement.
BAPA produced more tipping type of distal toot movement.
BAIBMD offers clinically successful distalization. Incorporating skeletal anchorage in the design of bodily molar distalizer helped prevent unwanted effects on anterior anchor teeth by eliminating reactive forces.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.