
Abstract
White spot lesions (WSLs) present a significant challenge in orthodontic practice, particularly in India, where they exhibit high prevalence rates. Despite the increased intricacy and notable surge in WSL occurrences among orthodontic patients in recent years, there is still a lack of sufficient preventive measures and effective management strategies. This expert opinion article synthesizes evidence from literature and expert insights to delineate the clinico-epidemiological factors, diagnosis, prevention, and treatment modalities for WSLs in the Indian context. Notably, the use of calcium sucrose phosphate (CaSP), known as Anticay, emerges as a promising remineralizing agent due to its multifaceted benefits, including remineralization and plaque acid neutralization. A comprehensive approach integrating patient education, regular monitoring, and customized treatment plans is crucial for optimal outcomes. In vivo/clinical trials are necessary to explore the optimal concentration of CaSP, alongside investigating potential synergistic effects with fluoride and other remineralizing agents. Incorporating CaSP into existing protocols represents a promising avenue for addressing WSL challenges in orthodontic practice in India.
Introduction
India’s diverse cultural and geographical landscape is also home to a significant dental concern: white spot lesions (WSLs), characterized by subsurface porosities, clinically appearing as milky-white opacities on smooth surfaces. 1 These subtle enamel demineralization lesions, an early stage of caries progression, pose a significant risk for dental morbidity and are commonly observed in orthodontic patients.2–5 Their formation is primarily attributed to prolonged plaque accumulation resulting from inadequate oral hygiene, further exacerbated by Streptococcus mutans and Lactobacillus colonization during fixed appliance therapy, salivary factors, increased carbohydrate intake, and changes in the oral environment. 6
A global meta-analysis indicated an incidence of 45.8% and a prevalence of 68.4% for WSL, 7 with the National Oral Health Survey in India reporting a prevalence between 50% and 84.7%, 8 highlighting the urgent need for preventive and therapeutic strategies. Managing WSLs effectively requires a multifaceted approach that prevents demineralization and biofilm formation while promoting remineralization.
In this expert opinion, we explore the diagnostic and therapeutic paradigms pertaining to WSLs within the Indian context. Against the backdrop of a nation where the awareness of dental treatment, especially orthodontic treatment, is on the rise and where dental infrastructure varies markedly across regions, we elucidate the challenges and advancements encountered in addressing this ubiquitous dental concern.
Methodology
Considering the increasing prevalence and associated risks of WSLs among orthodontic patients in recent years,9, 10 a focused group discussion was convened in February 2024. The primary objective was to evaluate prevailing clinical practices and facilitate knowledge exchange among experts to address the unmet needs of WSL management in the Indian context. The panel, comprising eight experienced orthodontists and two endodontists with over 15 years of experience in their respective fields, developed tailored recommendations through expert discussions and a thorough review of existing literature. Special emphasis was placed on the use of remineralizing agents, particularly calcium sucrose phosphate (CaSP), to improve prevention and treatment outcomes.
Literature Review and Expert Opinion
Clinico-epidemiological Factors Defining WSLs
Prevalence
Literature Evidence: Age: Approximately 67.6% of individuals under 18 undergo orthodontic treatment, reflecting a cultural norm of early dental alignment, likely driven by an increased focus on aesthetics during formative years. 11 This age group’s engagement suggests a broader societal wellness perspective, where orthodontic treatment is a part of personal and social development.
Gender: Studies show a higher incidence of WSLs in males, suggesting greater susceptibility.5, 12 Additionally, 61.1% of females report orthodontic use, potentially influenced by societal emphasis on women’s appearance. 13
Site: WSLs are most commonly found on the buccal surfaces around the brackets, particularly in the labiogingival region of lateral incisors, 14 with the maxillary posterior segments showing the least common occurrence. 4
Expert opinion:
Orthodontic treatment is most sought by patients aged 12-16 years, followed by those aged 16 and above. The experts have observed a prevalence of over 40% of patients developing WSLs during or after treatment bonding. Adolescents aged 12-19 are predisposed to developing WSLs due to factors like poor oral hygiene, dietary habits, and molar band usage. Factors such as age group, gender, and tooth location significantly impact the prevalence of WSLs. A higher prevalence of WSLs is observed in males. WSLs are frequently observed on upper incisors and canines, owing to anatomical location and tooth size. Screening for susceptibility to WSLs should be conducted at primary consultations, incorporating dental examinations, recording of family history, dietary charts, and oral hygiene maintenance protocols. Early identification of non-compliance with oral hygiene instructions can aid in determining alternative treatment plans. Additionally, maintaining digital records with photography before treatment initiation enables the detection of pre-existing WSLs.
Risk Factors
Evidence: WSLs during fixed orthodontic treatment result from a combination of factors: undisturbed plaque, fermentable carbohydrates, a susceptible tooth surface, and adequate time necessary for the lesion to develop. 15 Microbial factors, such as S. mutans and Lactobacillus colonization on plaque around orthodontic attachments,16–18 along with reduced salivary pH and flow, contribute to enamel demineralization. 19 Poor oral hygiene and restricted saliva access due to orthodontic appliances, combined with a high carbohydrate intake, further increase the risk.15, 20, 21 Plaque deposition is particularly high on resin-bonded materials and the gingival side of brackets.20–22
About 40%-79.3% of patients develop WSLs during or after orthodontic treatment.16, 23 Some individuals may experience increased salivary flow, which may help mitigate demineralization. 24 Therefore, assessing patient susceptibility to enamel demineralization at the start of orthodontic treatment is advisable. Factors to consider include salivary flow, caries history, plaque scores, caries activity tests, dietary habits, and fluoride exposure 15 (Figure 1).
Guzmán-Armstrong et al. highlight the importance of evaluating dietary habits, as factors like inadequate oral hygiene, frequent carbohydrate intake, recent caries history, and high decay-missing-filled surfaces indicate a higher risk for WSL formation. 25
Risk Factors Leading to White Spot Lesions (WSLs).
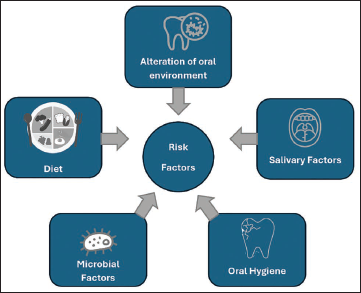
Expert Opinion: Poor oral hygiene (infrequent brushing, neglecting to floss) and sugary/low-fiber diets greatly increase WSL risk. Family history, malocclusion, and misalignment can also contribute. Over 40% of patients develop WSLs during treatment.
Early intervention is critical. Assess susceptibility, screen regularly, and educate patients on proper hygiene (brushing twice daily, using interdental aids). Water flossing, warm saline rinses, and tailored mouthwashes can be beneficial. Pre-treatment screening (45 days) assesses hygiene compliance, and salivary pH testing helps identify high-risk patients. Baseline photos (dehydrated and wet enamel) aid in early detection. Regular monitoring, ongoing education, and managing calculus buildup are crucial. The “3 Cs” approach (conveying decay severity, encouraging habit changes, and confirming hygiene plans) promotes successful WSL management.
Classification System for WSLs
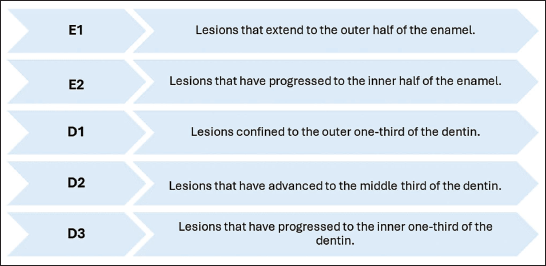
Literature Evidence: WSLs are categorized using various methods, with the International Caries Detection and Assessment System (ICDAS) classification being the most employed (Figure 2). This classification system was developed by Ekstrand et al. by amalgamating successful features from various caries detection and evaluation systems. 20 However, it became evident over time that ICDAS I was insufficient in assessing lesion activity. Consequently, in 2004, modifications were made, leading to the introduction of ICDAS II. 21
ICDAS II incorporates radiographic images of enamel and dentin lesions into its classification system. It delineates lesions into five classes:
International Caries Detection and Assessment System (ICDAS) Classification for White Spot Lesions (WSLs).
An alternative classification system by Gorelick et al. for WSLs focuses on their size and intensity to aid diagnosis 2 (Figure 3).
Gorelick Classification Based on Size and Intensity.
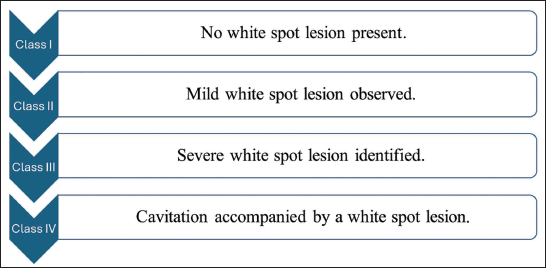
Expert Opinion: In day-to-day clinical practice, the application of ICDAS and Gorelick classification systems, particularly in Indian contexts, is minimal. Prevention and prompt management upon lesion detection are recommended. The experts opined that both classification systems held more value in clinical research for determining various stages of WSLs and evaluating treatment efficacy. A new classification system is needed, which should be based on severity, simple to use, and easy to implement in clinical practice.
Diagnosis of WSLs
Literature Evidence
Diagnosis of WSLs can be challenging due to their submerged enamel demineralization. 22 Clinically, WSLs appear opaque, white, and soft lesions on the tooth surface, often developing rapidly around the 4th week after initiating treatment due to poor oral hygiene.1, 4, 26
Expert Opinion
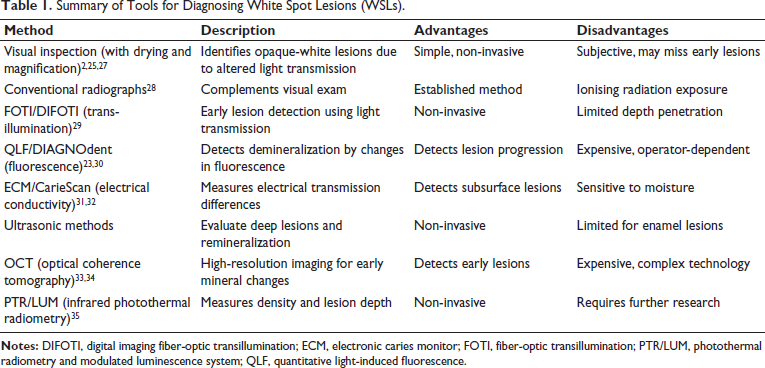
WSLs are typically detected 6-12 months into orthodontic treatment, highlighting the need for sustained patient motivation and regular prophylaxis. For improved accuracy, visual diagnosis is subjective, and experts recommend using digital photography, FOTI-DIFOTI, or Itero 5D scans (Table 1). Electronic caries monitor (ECM) and Caries Scan Pro are less commonly used for WSL diagnosis.
Summary of Tools for Diagnosing White Spot Lesions (WSLs).
Prevention and Treatment for WSLs
Literature Evidence
Orthodontic care prioritizes WSL prevention through two key strategies: (a) arresting demineralization or promoting remineralization and (b) preventing future enamel demineralization. Methods to achieve these goals in orthodontic patients include improved oral hygiene compliance, regular professional cleanings, topical agents, and fluoride-releasing adhesives.36, 37 Evaluating the pH of the saliva is also vital for identifying high-risk patients since degradation of minerals in enamel following acid attacks, the extent of demineralization, and the initiation or duration of remineralization are all closely linked to the pH level of saliva.37, 38
To prevent WSLs in orthodontic patients, prioritize education and motivation for a healthy diet and meticulous hygiene. Twice-daily fluoride toothpaste brushing targeting biofilm areas is fundamental.39, 40 Power toothbrushes or daily water irrigation alongside manual brushing can enhance plaque reduction compared to manual brushing alone. 41 Professional prophylactic cleaning, ideally two to three times a year, reduces bacterial load, enhances brushing efficacy, and aids patient cleaning efforts. 42 Fluoridated pastes and polishing tools can improve oral health. 42 Factors such as brushing frequency, patient age, time since appliance removal, treatment duration, and tooth type influence improvement in WSLs areas. 43
Expert Opinion
For successful orthodontic treatment, experts advocate pre-treatment screening (45 days) to assess hygiene compliance. Choosing between fixed appliances or aligners should consider oral hygiene, diet, and family history. WSL management involves patient education with visual aids (photographs) and reinforcement of hygiene protocols. These protocols include twice-daily brushing (soft bristle/sonic), interdental cleaning (flossers), warm saline/antimicrobial rinses, and regular prophylaxis. Additionally, motivation for healthy habits and periodic module replacement are crucial.
Treatment of WSLs Based on the Severity
Literature Evidence
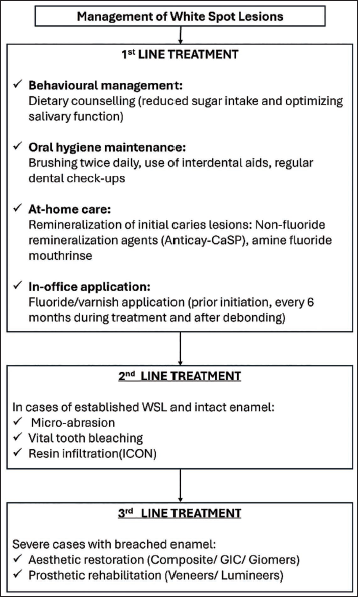
Various treatment options exist for WSLs, tailored based on severity. 44
First-line treatments:
Behavioral management: Behavioral modifications encompass dietary counseling, emphasizing reduced sugar intake, and optimizing salivary function. Oral hygiene maintenance: Brushing twice daily with a soft bristle, manual or sonic/ultrasonic toothbrush, adequate brushing technique, and use of interdental aids like water flosser to be advocated. Additional sessions for high-risk individuals, supported by regular dental checkups to reinforce adherence.45,46 At-home: Use of a potent remineralizing agent like Anticay is recommended instead of fluoridated toothpaste twice daily.47 Consider adding a fluoridated mouth rinse, such as amine fluoride, to enhance remineralization.48 In-clinic: Application of fluoride varnishes, 2-4 times yearly for continuous fluoride release.49–52
Second-line treatments: In conjunction with first-line treatments: Microabrasion: Acidic and abrasive compounds are applied to enamel surfaces to remove WSLs by compacting calcium and phosphate into interprismatic spaces. Followed by 2% sodium fluoride treatment for optimal results.53,54 Vital tooth bleaching: Ambulatory methods using trays or in-office procedures under professional supervision for effective enamel bleaching54,55 followed by application of remineralizing agent line Anticay. Resin infiltration (ICON system): A minimally invasive approach to camouflage white spots without removing tooth tissue, enhancing cosmetic appearance.54, 56
Third-line treatments: In conjunction with first-line treatments:
Expert Opinion
Fluoride toothpaste with at least 1,000 ppm significantly reduces dental caries in both primary and permanent dentition. 57 Amine fluoride effectively prevents demineralization and promotes remineralization by releasing high quantities of fluoride, aiding mineral reprecipitation as fluor-hydroxyapatite at lower pH levels, and shows superior enamel microhardness restoration compared to inorganic fluoride.58–60 Professionally applied fluoride treatments (gels, varnishes) are effective, especially in high-risk patients, with sodium fluoride varnish (5% and 2.26%) recommended for children under six due to minimal adverse effects. Application frequency should be tailored to caries risk.45, 50, 57, 61 In addition to fluoride therapy, non-fluoride agents, such as Anticay, have shown promise in promoting remineralization of initial carious lesions by increasing ion saturation in the oral cavity.47, 62, 63
Remineralizing agents are first-line treatments for WSLs, used both in-office and at-home, before and during orthodontic therapy. For established WSLs, microabrasion, vital bleaching, and resin infiltration serve as second-line interventions. Severe cases with breached enamel may require third-line management through aesthetic restorations (composite, GIC, giomers) or prosthetic rehabilitation (veneers, lumineers) (Figure 4).
Place in the Therapy of Fluoridated and Antibacterial Mouthwashes
Literature Evidence
Recent studies have highlighted the efficacy of chemical plaque control in managing gingivitis.64, 65 Adjunctive use of antibacterial mouthwash alongside mechanical brushing significantly reduces gingival inflammation and plaque indices. 66 Clinicians should consider recommending these mouthwashes for daily oral hygiene, especially for patients struggling to remove undisturbed plaque through mechanical means alone.65, 66 Amine fluoride mouthwashes have demonstrated superior efficacy in enhancing enamel remineralization and microhardness compared to inorganic fluorides.67, 68 Chlorhexidine, while effective, is less favored due to adverse effects like staining, bad taste, dry mouth/throat, tongue irritation, and wheezing. 69 Octenidine mouthwash offers a favorable alternative with superior efficacy, tolerability, and fewer adverse effects.70–73
Expert Opinion
Experts opined that fluoride agents exhibit bactericidal properties, with amine fluoride recognized as the most effective due to its surfactant action, offering superior caries resistance compared to inorganic fluorides. Following amine fluoride, stannous fluoride is identified as the next most effective fluoride, with higher bioavailability observed in amine fluoride mouthwashes. Typically, antibacterial mouthwashes consist of chlorhexidine or octenidine, although chlorhexidine is less favored due to staining. There is a perceived need for combinational products incorporating octenidine and amine fluoride for enhanced patient outcomes. However, the experts emphasized that while mouthwash plays a crucial role in oral health maintenance, it alone may not suffice for biofilm eradication.
Place in the Therapy of Anticay in the Management of WSLs
Literature Evidence
Saliva supports remineralization by neutralizing acids, forming a protective barrier, and supplying vital minerals essential for assessing cavity risk. However, natural mineral levels may be insufficient, especially in acidic environments. Anticay (CaSP) releases soluble calcium and phosphate ions in saliva under oral pH conditions, contributing to its cariostatic properties and playing a crucial role in enamel repair. 74 Saliva enhances the effectiveness of Anticay by facilitating ion release, thereby averting WSL formation through multiple mechanisms.47, 73
Remineralization: CaSP releases calcium and phosphate ions into saliva, promoting remineralization through the common ion effect.
Acid inhibition: Sucrose phosphate ions in CaSP adsorb onto enamel surfaces, slowing acid dissolution and preventing demineralization.
Plaque acid neutralization: CaSP actively neutralizes plaque acids, providing additional protection against enamel erosion.
Its mechanism of action complements that of fluoride, as the release of calcium and phosphate ions from CaSP, in the presence of fluoride, aids in forming fluorapatite, reducing enamel solubility in acids. The multifaceted action of CaSP makes it an effective agent for preventing the development of WSLs and maintaining oral health.47, 75
In the study by Wani et al., CaSP tooth cream applied around orthodontic brackets demonstrates significantly superior remineralization effects compared to casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) 76 (Table 2). Another study by Sebastian et al. highlighted that CaSP demonstrated the most significant increase in enamel surface microhardness, followed by nano-hydroxyapatite (HAP) and CPP-ACP. The results from the study suggested that CaSP in toothpaste may offer superior enamel strengthening compared to nano-HAP and CPP-ACP. Consequently, it could be a potential alternative to fluoride toothpaste, particularly in pediatric dental care. 77 This is significant because excessive fluoride intake, particularly in children under 8 years old, can increase the risk of dental fluorosis when the fluoride level in drinking water exceeds 1.5-2.0 ppm, as highlighted by the US Center for Disease Control and Prevention (CDC). 78
A Summary of In Vitro and In Vivo Studies on the Efficacy of CaSP.
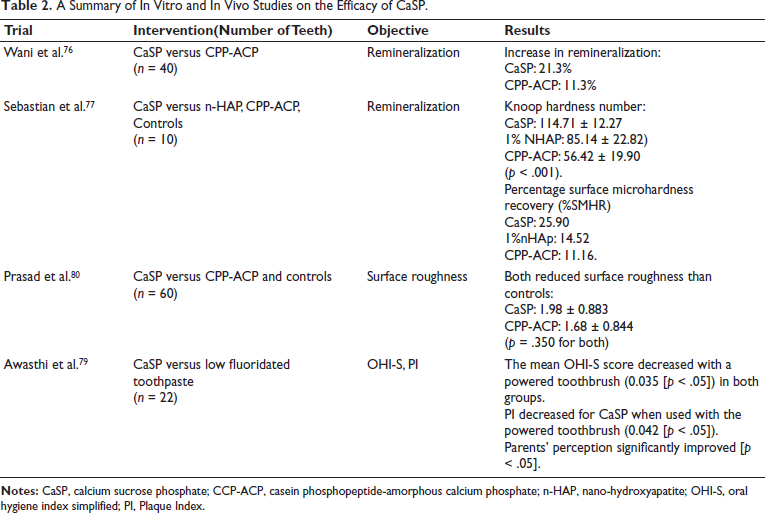
The study by Awasthi et al. also highlighted similar findings where a significant reduction in the Plaque Index (PI), specifically for CaSP, when combined with a powered toothbrush (0.042 [p < .05]). 79 In another study by Prasad et al., CaSP and CPP-ACP both effectively reduced the surface roughness when compared with the control groups, thereby preventing demineralization. 80 Karad and Dhole’s review of 13 articles found CaSP tooth cream more effective than CPP-ACP and casein phosphopeptide-amorphous calcium phosphate with fluoride (CPP-ACPF) in increasing enamel microhardness and arresting WSL. 8
Expert Opinion
Experts propose a multifactorial approach to dental remineralization. While low-dose fluoride prevents demineralization, high-dose fluoride and agents like Anticay and CPP-ACP may promote deeper remineralization. Anticay (CaSP), recommended for initial remineralization, can be used twice daily (e.g., as toothpaste or lozenges) alongside amine fluoride mouthwash. CaSP at 30% in trays is effective, with routine clinic application every 6 months suggested for ongoing management.
Limitations and Recommendations for Future Research
While the expert panel included orthodontists and endodontists nationwide, a larger group is recommended for more generalized findings, minimizing potential bias. A forthcoming real-world evidence study will evaluate CaSP’s efficacy in managing WSLs during orthodontic treatment. Future research should determine the optimal CaSP concentration for maximal efficacy and explore synergistic effects with fluoride or other remineralizing agents to enhance therapeutic outcomes. Additionally, studies on patient acceptability, compliance, and long-term outcomes of CaSP-treated lesions are needed to inform its clinical application.
Conclusion
Effective management of WSLs in orthodontic patients requires a comprehensive approach combining prevention and treatment. Anticay, CaSP, shows promise for high-risk patients due to its remineralization properties, plaque acid neutralization, and cariostatic effects, all without the risk of fluorosis. CaSP offers a promising strategy for addressing WSL challenges in orthodontic care. A multifactorial approach integrating patient education, regular monitoring, and customized treatment plans is crucial for optimal outcomes. Further research is needed to fully understand and refine CaSP’s role in managing WSLs.
Footnotes
Acknowledgments
The authors extend their appreciation to Dr. Neal Kedia, Dr. Pranav Chandarana, Dr. Prashant Dhole, Dr. R.K. Jaiswal, Dr. Tanmay Mittal, and Dr. Tusar Kanti Nayak, who were part of the expert group discussion, as their valuable contributions were instrumental in the development of the recommendations and the final manuscript. The authors also thank IntelliMed Healthcare Solutions Pvt. Ltd., Mumbai, for medical writing support in assisting in the development of this manuscript.
Authors Contribution
Dr Balvinder Singh Thakkar, Dr N. R. Krishnaswamy, Dr P. D. Joshi, and Dr Nikhil Bahuguna contributed to the conception and design of the article, drafted the manuscript, and revised it critically for important intellectual content. Dr Pratibha Goswami facilitated the expert group discussion, collated key insights, and supported the medical writing process. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The expert group discussion was conducted in association with Abbott Healthcare Pvt. Ltd. This article is based on the views expressed during the expert group discussion. The views expressed and discussed in the meetings and stated in this consensus article are the independent views of the authors and not of Abbott Healthcare Pvt. Ltd. Dr Pratibha Goswami is an employee of Abbott and had no role in finalizing recommendations arising from views shared during the expert group discussion.
Ethical Approval
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The expert group discussion was funded by Abbott Healthcare Pvt. Ltd.
Informed Consent
Author verification forms and author agreement forms available as their consent to publication however no patient consent was sought as this cumulates expert opinion and existing literature evidence without involving patients.