
Abstract
Abstract
Objectives: Treating white spot lesions (WSL) to create a sound and esthetically pleasing enamel surface is a question yet to be fully answered. The objective of this randomized controlled trial was to measure and compare the degree of regression of WSL during orthodontic treatment achieved by using three commercially available materials.
Methods: A single-blinded randomized prospective clinical trial, comprising 80 patients categorized into four groups (one control group and three experimental groups, with 20 subjects per group) using block randomization, was conducted. Group A (control group): Colgate strong toothpaste; and experiments groups were Group B: GC tooth mousse, Group C: Phos-Flur mouthwash and Group D: SHY-NM. Subjects were instructed to use the designated dentifrice/mouthwash and photographs were taken at baseline, third and sixth months, and white spot lesions were reassessed in the maxillomandibular anterior teeth.
Results: All the three groups had shown an improvement in WSL. But Group B has shown the greatest difference in mean values of decalcification index (DI) scores.
Conclusion: All three commercially available products showed a regression of WSL over a 6-month duration. GC tooth mousse proved to be the most effective means of treating WSL over other regimens.
Introduction
White spot lesion (WSL) is the earliest macroscopic evidence of enamel caries and is commonly seen during orthodontic therapy. 1 Fejerskov et al. 2 defined WSLs as ‘the first sign of a carious lesion on the enamel that can be detected with naked eye’.
After four weeks of orthodontic bonding, WSLs become noticeable and are commonly seen on tooth surface around the bracket, especially in the gingival areas. 3 Patients treated orthodontically showed broadly about 2% to 96% of white spot lesions. This large range is thought to be mainly due to the difficulty in standardizing clinical examinations. 4
Clinically visible white spot lesions were seen in patients under orthodontic treatment 1 month following the start of the treatment in studies done by O’Reilly et al. 5 and Ogaard et al. 6 . This is a very small estimated time interval between two successive orthodontic treatment sessions. WSLs that are crescent in shape are commonly seen near the bracket base; they are also seen under loose bands or as linear defects near the margin of the band.
Gorelick et al. 7 investigated the prevalence of carious white spots after removing bonded appliances and reported that about 50% of the patients reported with white spot lesions at least on a single tooth. In the same study, incidence of white spot lesions in the maxillary anterior segment was observed to be 15.3%, and the maxillary lateral incisor was the tooth with the highest percentage of WSL incidence (23%).
Remineralization of teeth can be brought about by various resolution procedures and products, such as saliva, mouth rinses and toothpaste, with various components such as increased fluoride concentrations, casein phosphopeptide-amorphous calcium phosphate (CPPACP) and calcium sodium phosphosilicate glass (CSPG). Microabrasion and composite restorations are aggressive techniques used to treat white spot lesions.8, 9
A decrease in the size of white spot lesion was noted over time mainly due to two mechanisms:
Fluoride acts as a remineralizing agent by depositing fluoroapatite in place of dissolved hydroxyapatite. 12 High fluoride concentration results in remineralization of WSL via hypermineralization, which usually gives unsightly tooth.13–15 The unsightly tooth appearance is because of surface remineralization which inhibits the movement of ions into the subsurface of the lesion, thereby affecting light reflection touching the tooth surface.16, 17
Materials that carry calcium and phosphate ions to enamel have been recommended to assist in remineralization with a more esthetically pleasing result. CPPACP is one such material12–18 that acts by binding itself to the tooth surface and the plaque coating it. This bond helps maintain a high concentration gradient of soluble calcium and phosphate ions, which in turn results in the stabilization of amorphous calcium phosphate, both of which play an important role in remineralization.12, 19, 20 These calcium and phosphate ions get deposited in the crystal voids present in the crystal structure of the enamel and promote crystal growth; this has a positive impact on the reflective properties of the enamel. 15 CSPG is marketed as a treatment for dentin sensitivity. 16 Its success and mechanism of action as a sensitivity-reduction agent promoted interest in it being used as a remineralization agent. 21 This product is believed to maintain high concentrations of calcium and phosphate on the enamel surface. NovaMin is composed of inorganic calcium phosphate minerals and silica. 20 The method of action is that the release of sodium ions through interaction with oral fluids results in an increase in pH, which in turn releases calcium and phosphate to form a layer of calcium phosphate.
This layer then crystallizes, producing a crystalline hydroxycarbonate apatite layer filling the crystal voids in the enamel. 22 Therefore, the aim of this in vivo study was to compare the regression of WSL treated with three commercially available products: GC tooth mousse (CPPACP), Colgate Phos-Flur mouthwash (flouride and amulated phosphorus) and SHY-NM (calcium sodium phosphosilicate glass).
Methodology
The in vivo study was carried out in the Department of Orthodontics and Dentofacial Orthopaedics. The study protocol was reviewed and approved by the institutional ethical committee (No. IERB/2015-16/01). Patients undergoing orthodontic treatment using fixed appliances in the postgraduate orthodontic clinic were included for the study.
Inclusion Criteria
Included in the study were patients:
aged between 12 and 25 years; with fair oral hygiene; with satisfactory general health; with a decalcification index (DI) score of 2 (visible white spot lesions), with at least 6 months of orthodontic treatment remaining; and with maxillary and mandibular anterior teeth bonded with fixed orthodontic appliance;
Exclusion Criteria
The exclusion criteria for the study were:
enamel hypoplasia amelogenesis imperfecta fluorosis active periodontal disease active dental caries
Sample Size
The mean changes in decalcification index and standard deviation estimates used for sample size calculations were from a previous in vivo study. 1 Twenty to 25 individuals were selected in each group, with a power greater than 85% to calculate the difference of 1.0 unit change in the decalcification index (assuming a standard deviation of 1.0) and a greater than 80% power to calculate the difference of 1.25 if the standard deviation was more than anticipated (1.3).
A total of 80 (20 per group) patients were enrolled in this prospective single-blinded randomized clinical trial categorized into four groups with the help of a computer as follows:
Control group
Group A: Colgate strong toothpaste
Experimental Group
Group B: GC tooth mousse (CPPACP)
Group C: Colgate Phos-Flur mouthwash (CPF)
Group D: SHY-NM (CSPG)
Before the start of orthodontic treatment, professional dental cleaning and oral hygiene instructions were given. Frontal intra-oral photographs were taken at the baseline for assessment of decalcification index. Decalcification index was measured on the anterior teeth.
Subjects were instructed to use the designated dentifrice/mouthwash. The follow-up photographs were taken at 3 months and 6 months for assessment of WSL in the maxillary and mandibular anterior teeth. All the photographs were taken using a standardized camera (Nikon D5300, with 90–100 mm micro lens, ISO of 200, F of 18 and shutter speed of 1/125) and the photographs were taken in a well-illuminated environment.
Measurement of Decalcification
Modified Gorelick et al.
5
DI, which is being currently used, scores each tooth as follows:
0: absence of a WSL 1: visible white spots without any surface interruption (mild decalcification) 2: visible white spot lesion with a roughened surface that does not require a restoration (moderate decalcification) 3: visible white spot lesion with surface interruptions (severe decalcification) 4: cavitation
For DI scoring, the photographs were taken at the beginning of the study for documentation purpose. The camera settings mentioned in the methodology were maintained throughout the study.
Statistical Analysis
Data were analyzed using SPSS version 23, and normality assumption was tested using Shapirowilk test. ANOVA and post-hoc Tukey tests were done for intragroup and intergroup comparisons, respectively.
Results
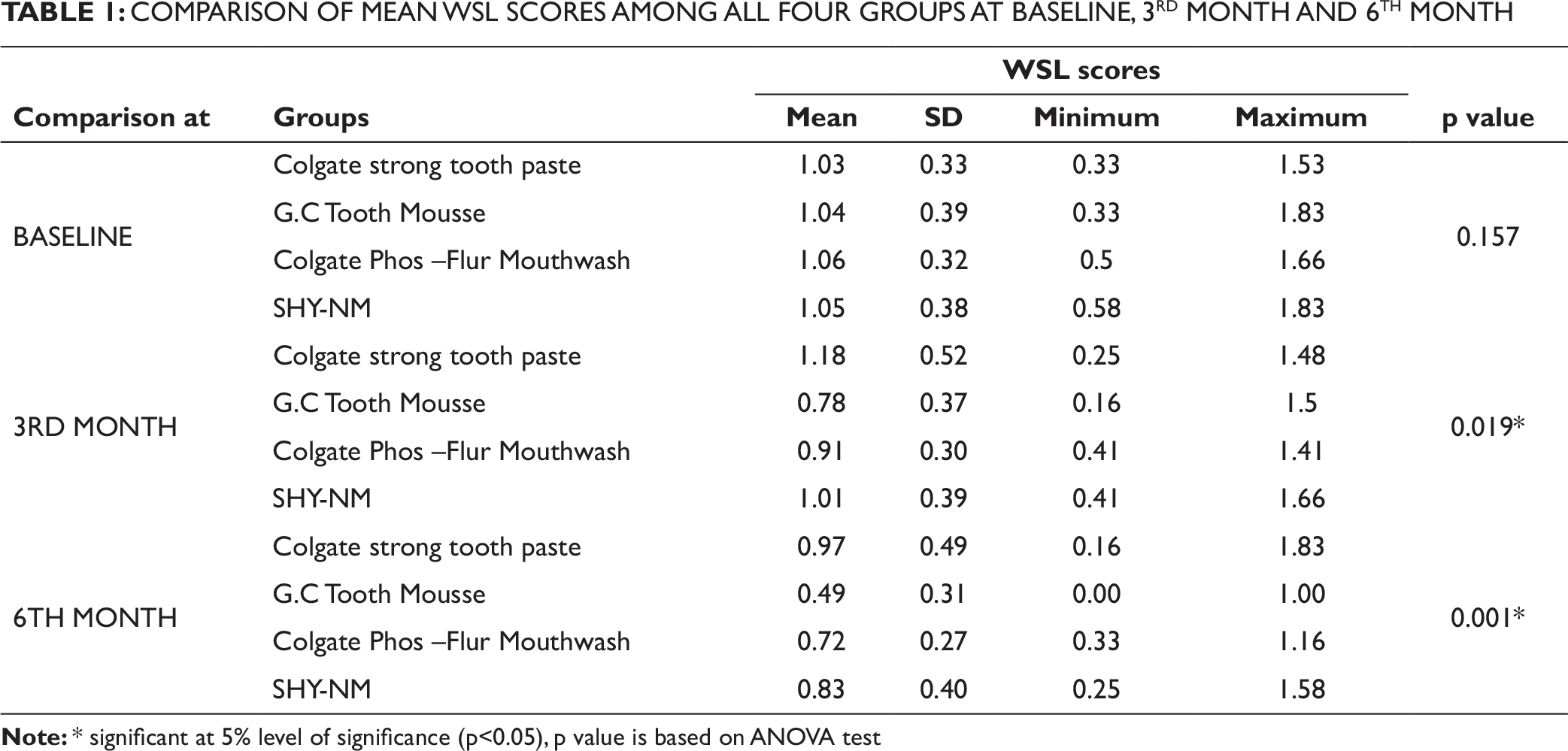
Mean and standard deviation (SD) of DI scores at baseline, 3 months and 6 months for the four groups are given in Table 1. The score in Group A at baseline is 1.03 ± 0.33, at 3 months is 1.18 ± 0.52 and at 6 months is 0.97 ± 0.49. The score in Group B at baseline is 1.04 ± 0.39, at 3 months is 0.78 ± 0.37 and at 6 months is 0.49 ± 0.31. The score in Group C at baseline is 1.06 ± 0.32, at 3 months is 0.91 ± 0.30 and at 6 months is 0.72 ± 0.27. The score in Group D at baseline is 1.05 ± 0.38, at 3 months is 1.01 ± 0.39 and at 6 months is 0.83 ± 0.40.
Results of ANOVA at baseline showed statistical insignificance as p > 0.05, and statistically significant differences were seen at third month and sixth month as p < 0.05.
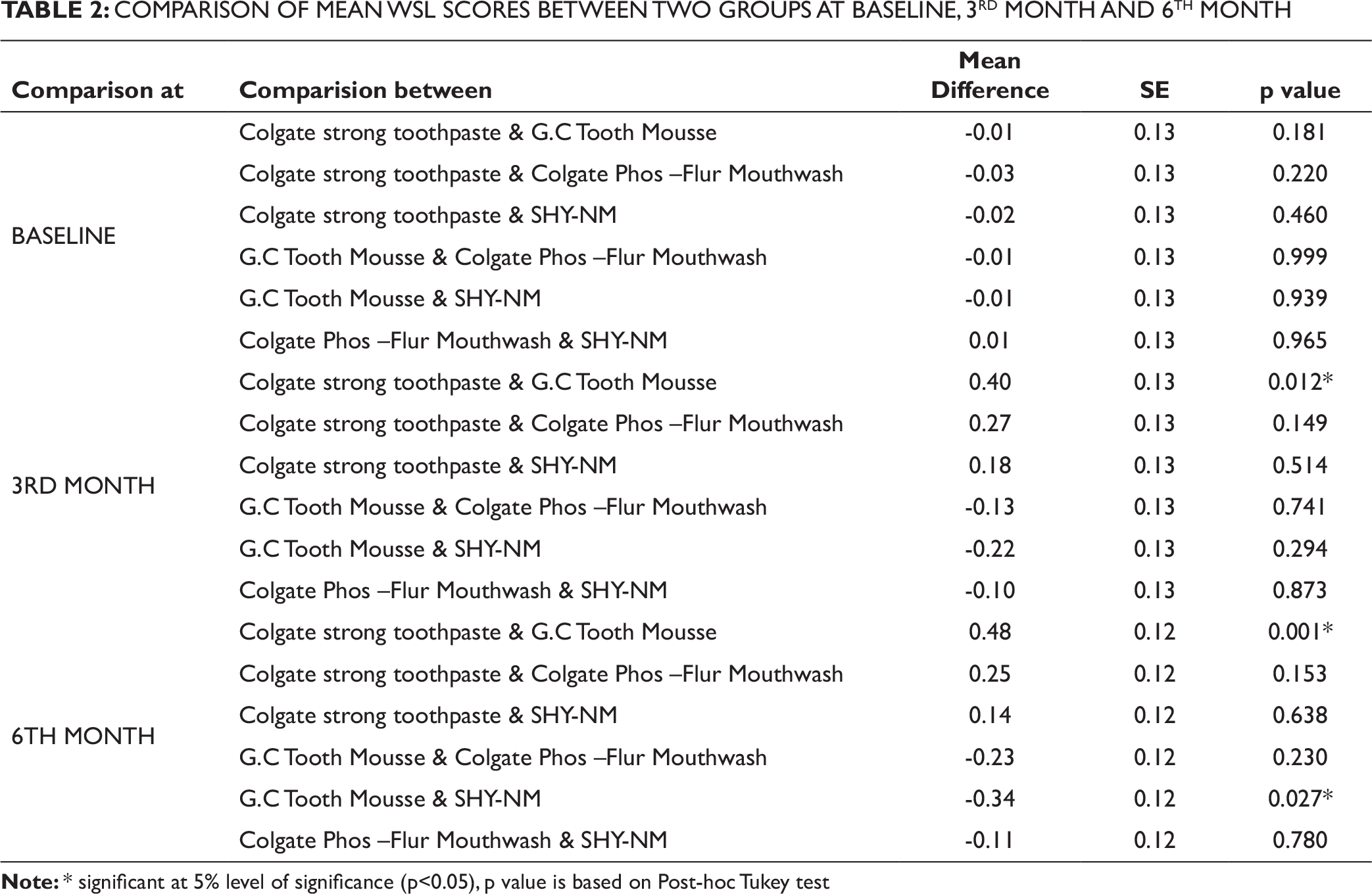
Post-hoc Tukey test showed a statistically significant difference between Colgate strong and GC tooth mousse at the third month and between Colgate strong toothpaste and GC tooth mouse, and GC tooth mousse and Novamin at the sixth month, while the rest of the comparisons were insignificant, as shown in Table 2.
Discussion
Many studies have been done to evaluate the ability of remineralizing agents to remineralize enamel in an artificial environment; this in vivo study illustrates the importance of oral environment and gives patient-centered outcomes. The products that claimed to resolve white spot lesions were selected for this study, and each of them influences the enamel surface and substrate in a different manner. Studies done by previous researchers have shown a reduction in the size of WSL with the use of the calcium and phosphorous.17, 19, 23
The outcome of our study, which utilizes four delivering systems for calcium and phosphorous compounds, shows subsequent remineralization of white spot lesions with all the delivery systems. The remineralization of the demineralized enamel was the greatest with CPPACP, followed by Colgate Phos-Flur mouthwash, CSPS and least with a general fluoridated toothpaste.
The results of our study showed statistically significant difference in remineralization of enamel with all the four groups at the end of 3 months and 6 months.
When comparing the DI scores between demineralization products, normal fluoride toothpaste and GC tooth mousse showed a statistically significant difference at the third and sixth months, whereas GC tooth mousse and Novamin showed statistically significant difference only at the sixth month.
COMPARISON OF MEAN WSL SCORES AMONG ALL FOUR GROUPS AT BASELINE, 3RD MONTH AND 6TH MONTH
COMPARISON OF MEAN WSL SCORES BETWEEN TWO GROUPS AT BASELINE, 3RD MONTH AND 6TH MONTH
Anderson et al. 27 reported that a combination of CPPACP with 0.05% sodium mouthwash and fluoridated dentifrice demonstrated a significant improvement in WSLs. However, the authors reported that the CPPACP group was associated with a greater number of WSLs that totally disappeared over the period of 12 months compared to 0.05% sodium fluoride mouthwash and fluoridated dentifrice combination. Robertson et al., 19 from a randomized clinical trial, reported a greater regression of white spot lesions during the initial period of orthodontic treatment with CPPACP.
However, there are studies in contrast to our results which have reported an insignificant change in the size of WSLs over time in groups using the fluoride delivery systems.13, 28, 29 Beerens et al. 28 concluded that the use of the CPPACP with fluoride paste supplementary to oral hygiene over the period of 4 months had no clinical advantage.
In a randomized trial 29 conducted, 60 adolescents were given daily application of either CPPACP (tooth mousse) or standard fluoride toothpaste to treat WSL. The study was carried out for a period of 1 month, then the results were analyzed by laser fluorescence and visual scoring (Gorelick scale) from the digital photographs. The results showed 26–58% reduction in the mean area of the lesion, but no significant differences were found between the CPPACP and the control groups. Another randomized trial 13 compared WSLs treated with a low-fluoride mouth rinse (50 ppm) to those treated with a non-fluoride mouth rinse. At the end of 12 weeks, the lesions decreased by 40% (SD, 14.5) in the treatment group and by 51.5% (SD, 12.3) in the control group, thus indicating no significant benefits from the low-level fluoride.
The results of this current study have shown that CPPACP was superior in its ability to remineralize WSLs. The multifactorial anti-cariogenic mechanism for CPPACP has a three-fold mode of action: (a) Remineralization of enamel is brought about by preserving the supersaturated state of enamel minerals calcium and phosphate in plaque; (b) It slows down the initiation of biofilm and suppresses bacterial adherence to the tooth surface; and (c) It reduces the pH in the oral environment by acting as a buffering agent. 28
A limitation of our study was the lack of use of laser fluorescence and quantitative light–induced fluorescence to assess WSLs, which could have provided another superior method of assessment. However, the use of this technology in our trial was not feasible due to our budget limitations.
Conclusion
All the three commercially available products—GC tooth mousse (CPPACP), Colgate Phos-Flur mouthwash (flouride and amulated phosphorus) and SHY-NM (calcium sodium phosphosilicate glass), showed regression of WSL over a period of 6 months. GC tooth mousse proved to be the most effective means of treating WSL over other treatment regimens.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.