
Abstract
Abstract
Background: Despite improved oral hygiene regime and availability of preventive formulations, dental caries continues to be a global dental problem. Calcium sucrose phosphate (CaSP) is a remineralizing agent with cariostatic action, which is commonly available in the form of tooth cream. Considering the paucity of evidence, this systematic literature review aims to evaluate the remineralizing efficacy of CaSP.
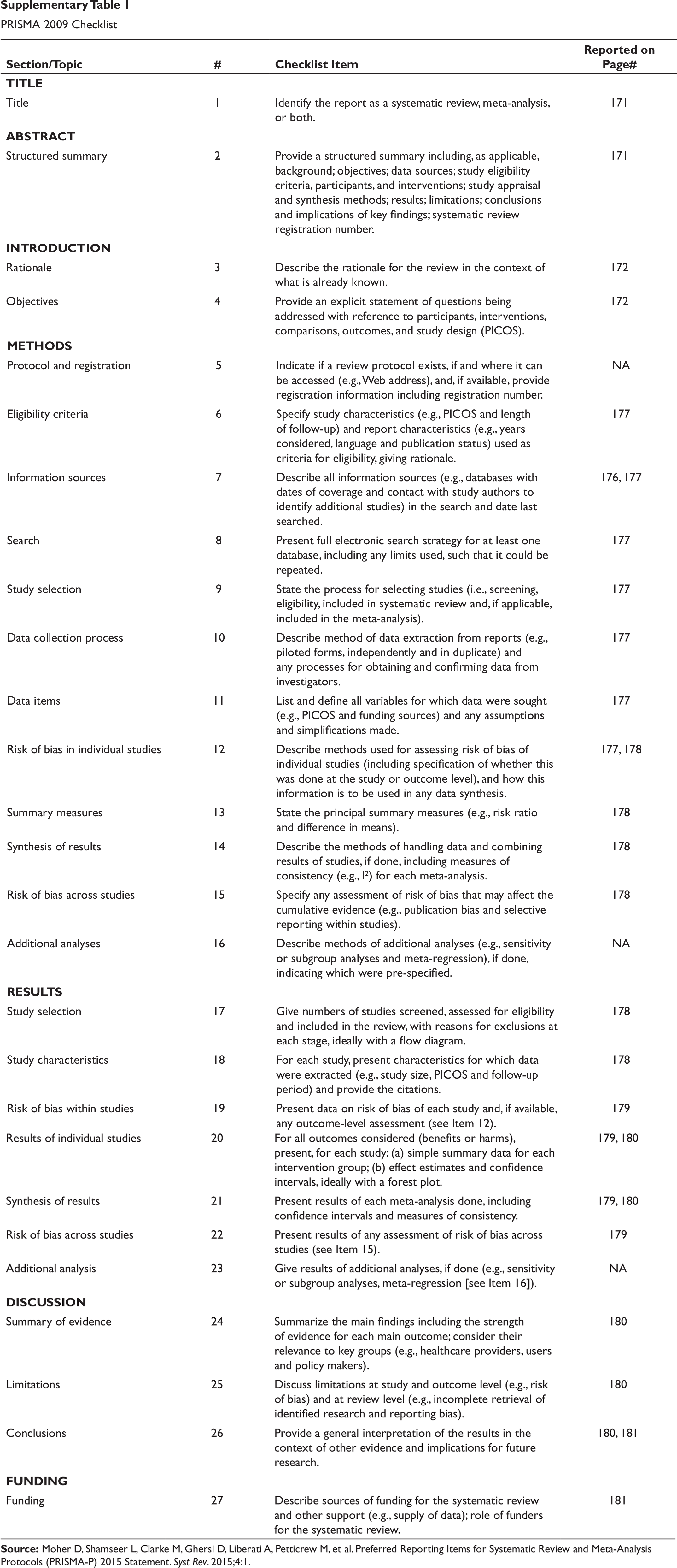
Methodology: The review was conducted as per Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines. Various databases, including PubMed, Cochrane Central, and Google Scholar, were searched until March 15, 2018 and were assessed for inclusion by two independent reviewers. The primary outcome was to assess the remineralizing efficacy of CaSP, and the secondary outcome was to assess the potential of CaSP in arresting white spot lesion(s) on enamel.
Results: Out of 2,876 articles, only 13 were qualified for inclusion. Included studies presented a low risk of bias for the following items: caries-free teeth or restoration, and adherence to manufacture’s instruction for the usage of remineralizing agent in the risk of bias scale. Ten studies reported an increase in the microhardness of enamel after CaSP application, and three studies reported the effect of CaSP on arresting white spot lesion(s). CaSP was found to be a better remineralizing agent in comparison to casein phosphopeptide-amorphous calcium phosphate (CPP-ACP), casein phosphopeptide-amorphous calcium phosphate with fluoride (CPP-ACPF) and other remineralizing agents in terms of increasing microhardness of enamel. In addition, CaSP application was also found to have a beneficial effect in restoring the color of white spot lesion(s) to that of normal enamel.
Conclusion: CaSP tooth cream was found to be an effective remineralizing agent, compared to others, such as CPP-ACP and CPP-ACPF, in terms of increasing the mean microhardness of enamel and arresting white spot lesion(s).
Keywords
Introduction
Dental caries (or cavities) refers to demineralization of enamel, dentin or cementum due to acid production by bacterial communities of Streptococcus mutans, Lactobacillus species, Bifidobacterium, etc. 1 These acids are produced due to the metabolism of dietary carbohydrates which dissolves the mineral component of the tooth and releases calcium and phosphate ions (demineralization). 2 It continues to be a major oral health problem with a global prevalence of 35%.3, 4 National oral health survey reported an overall prevalence ranging between 50% and 84.7% in Indian population. 5
Multiple factors like smoking, tobacco use, bad oral hygiene, diet, brushing habits and inadequate preventive dental care are associated with high incidence of caries. 3 The use of bleaching agents (hydrogen peroxide, carbamide peroxide, etc.) and iron drops constitutes the other common reasons for enamel demineralization.6, 7 Consequently, demineralization enhances the porosity of enamel and results in white spot lesion(s) on tooth surface. 6
Remineralization of enamel, that is, diffusion of calcium and phosphate ions back into crystal voids (created by demineralization) helps in the prevention of dental caries. 8 Saliva has the ability to remineralize enamel by neutralizing acids produced by dental plaque and maintaining an environment rich with calcium and phosphate ions. However, the remineralization by saliva is a slow process and is insufficient to produce net mineral gain. 9 Additionally, natural remineralization through saliva has little improvement on the aesthetics and structural properties in the deeper lesions. 10 Hence, there has been a lot of emphasis on enamel remineralization using agents such as calcium sucrose phosphate (CaSP)–calcium orthophosphate complex, casein phosphopeptide–amorphous calcium phosphate (CPP-ACP), calcium sodium phosphosilicate, nano-hydroxyapatite, seed extract, and galla chinensis, which are presently available in different formulations. 11
The CaSP, also known as anticay, provides both calcium and phosphate ions in a soluble form in high concentrations.2, 6, 12 It is a mixture of 85% by weight of calcium salts of phosphoric acid esters of sucrose and 15% by weight of inorganic calcium orthophosphate.2, 13 This combination has a high water solubility index which releases more free calcium and phosphate ions as compared to saliva. Anticay reduces the rate of demineralization of enamel, increases the rate of remineralization by a common ion effect and actively neutralizes the plaque acids.6, 13
Several in vitro studies have compared CaSP with other remineralizing agents and have shown encouraging results with regards to its remineralization potential.6, 9, 14 However, no published systematic review explicitly evaluated the remineralizing efficacy of CaSP. Hence, the current systematic review was sought to determine the potential of CaSP as a remineralizing agent in increasing the microhardness of enamel and arresting the white spot lesion(s).
Methods
Characteristics of Included Studies
PRISMA 2009 Checklist
Data Sources and Search Strategy
Risk of Bias Assessment Among Included Studies
Electronic Database Searches (PubMed [Inception-2018.03.15]; Google Scholar [Inception-2018.03.15]; Cochrane Central [Inception-2018.03.15])
Study Selection
We have included studies which had evaluated the following parameters: (a) remineralizing efficacy of CaSP either alone or in comparison with other agents; (b) microhardness of enamel after CaSP application; and (c) arrest of white spot lesion(s).
Reviews, commentaries, letters to the editor, study protocols, and editorials were excluded. Studies with incomplete information, insufficient data, or evaluating properties other than remineralizing efficacy or assessing the remineralizing efficacy of agents other than CaSP were excluded. Two reviewers independently assessed the suitability of articles before inclusion in this systematic review. In case of any differences of opinion pertaining to the inclusion of articles, the first step was to resolve the differences by discussion and reaching a consensus. If a consensus was not reached, then an arbitrator was consulted for a final decision.
Data Extraction and Quality Assessment
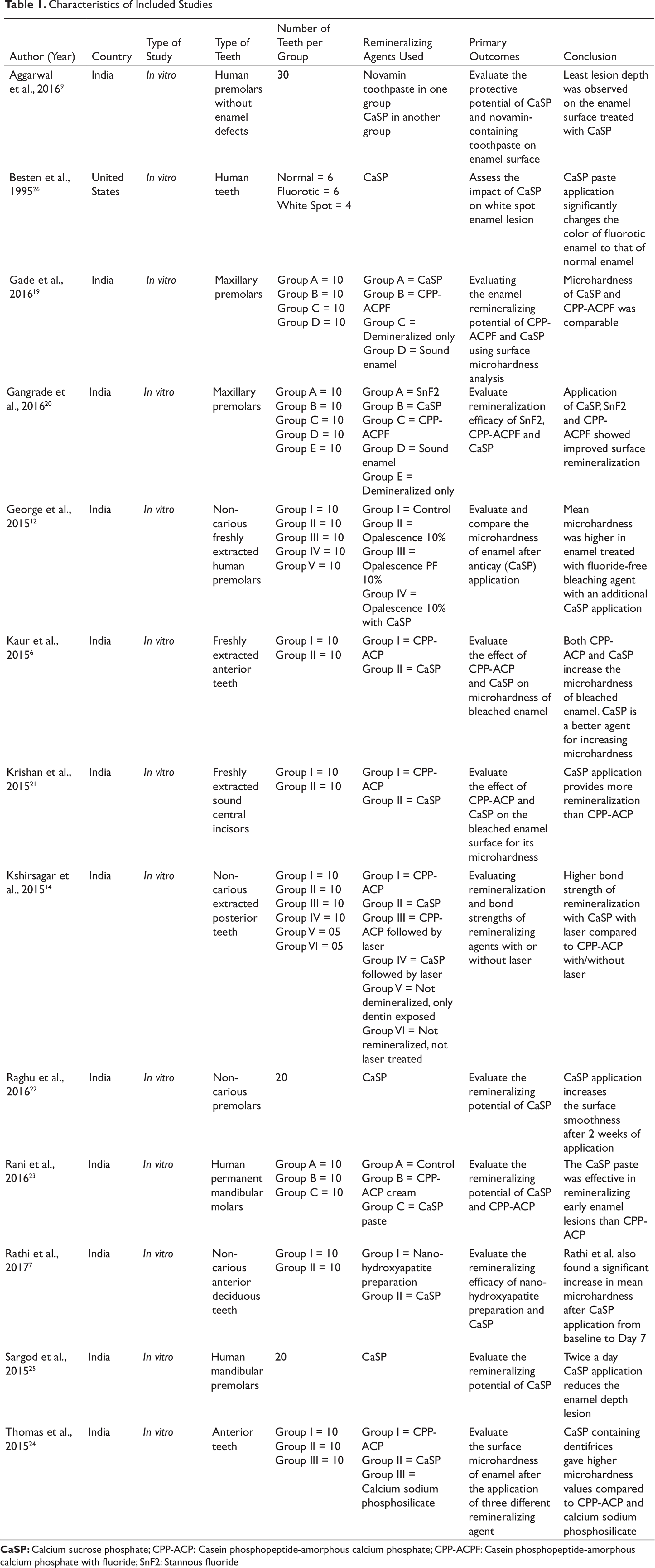
Common parameters were compiled in a pre-designed data table from selected literature for further assessment. The parameters included study author, country, type of study, number of teeth per group, remineralizing agents used, and the primary outcomes (Table 1).
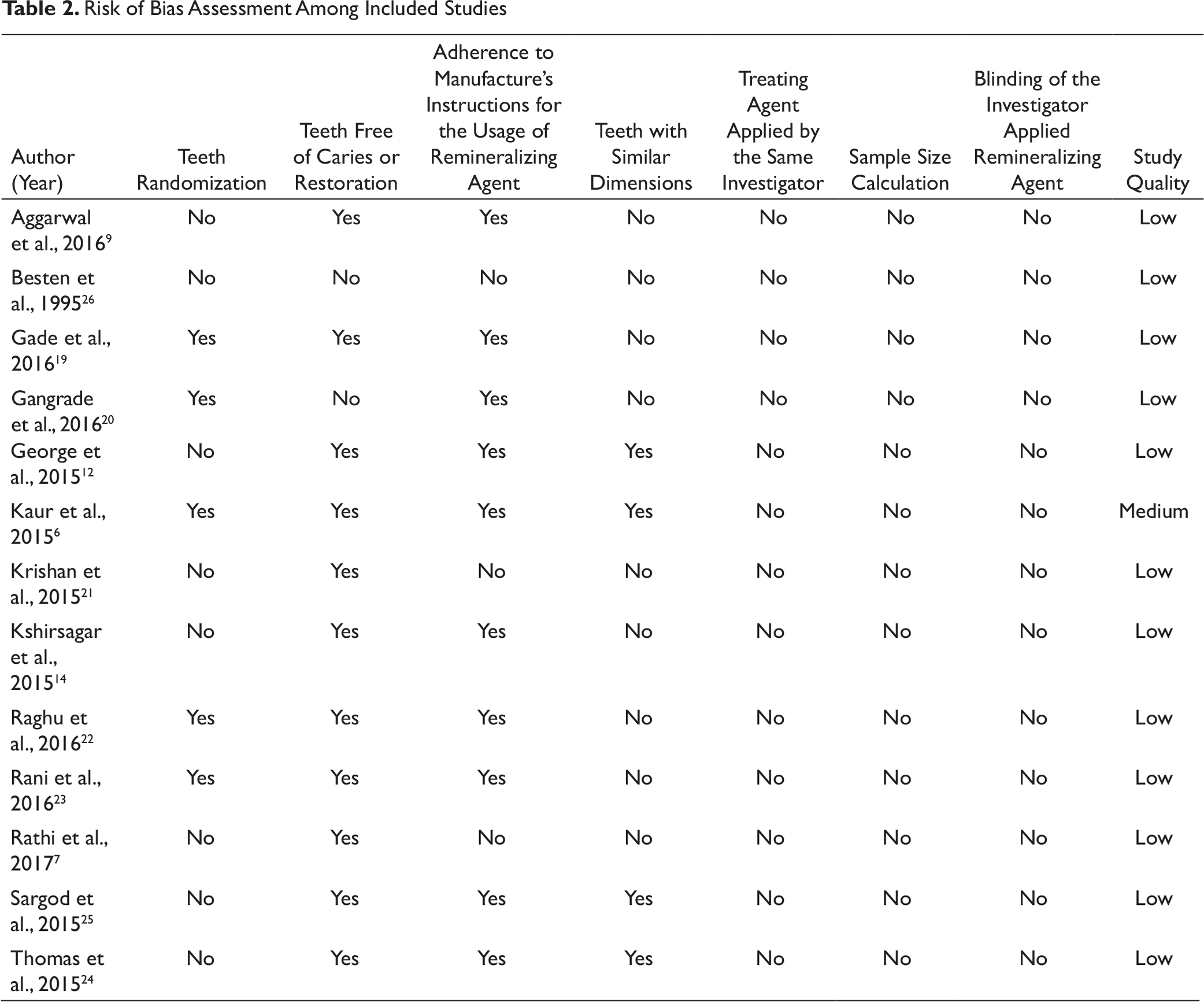
Selected literature were assessed for quality using the risk of bias (RoB) tool as described in earlier published studies.16, 17 Quality of each included article was assessed by calculating a total score based on the presence (or absence) of the following parameters: randomization of teeth, restoration or use of caries-free teeth, adherence to manufacture’s instructions for the usage of remineralizing agent, similar dimensions teeth, treating agent applied by the same investigator, sample size calculation, and blinding of the investigator applying remineralizing agent. Presence of each of the aforementioned parameter would earn a “Yes”, while the absence would earn a “No” for every article being assessed. Articles having six to seven “Yes” (i.e., total score for article) were considered having a high quality, those having four to five “Yes” were considered to have a medium quality, while those with less than or equal to three “Yes” were considered to have a low quality. Two independent reviewers independently assessed the quality of all the included articles.
Outcome Measures and Statistical Analyses
The primary outcome of this study was to assess the remineralizing efficacy of CaSP by determining the change in microhardness of enamel after CaSP application. The secondary outcome was to assess the potential of CaSP in arresting white spot lesion(s) on the enamel. The articles included in this systematic review were not eligible for meta-analysis due to heterogeneity amongst them. So, only qualitative analysis was done and described in the form of qualitative synthesis. 18
Results
Search Output
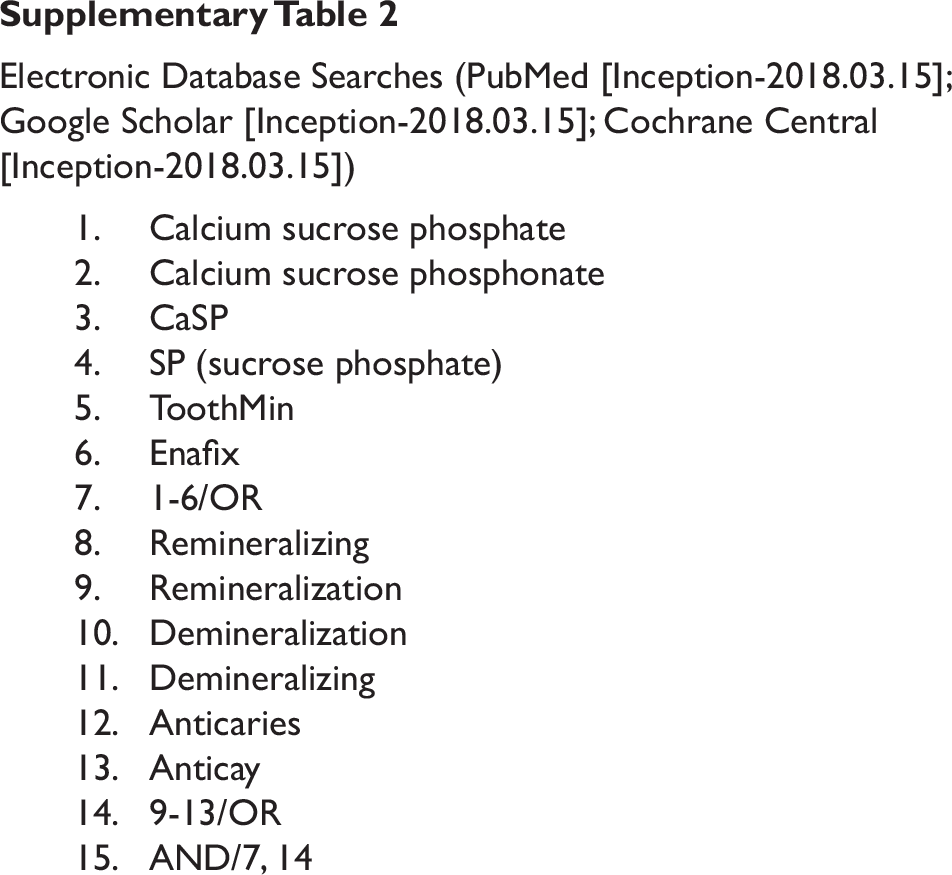
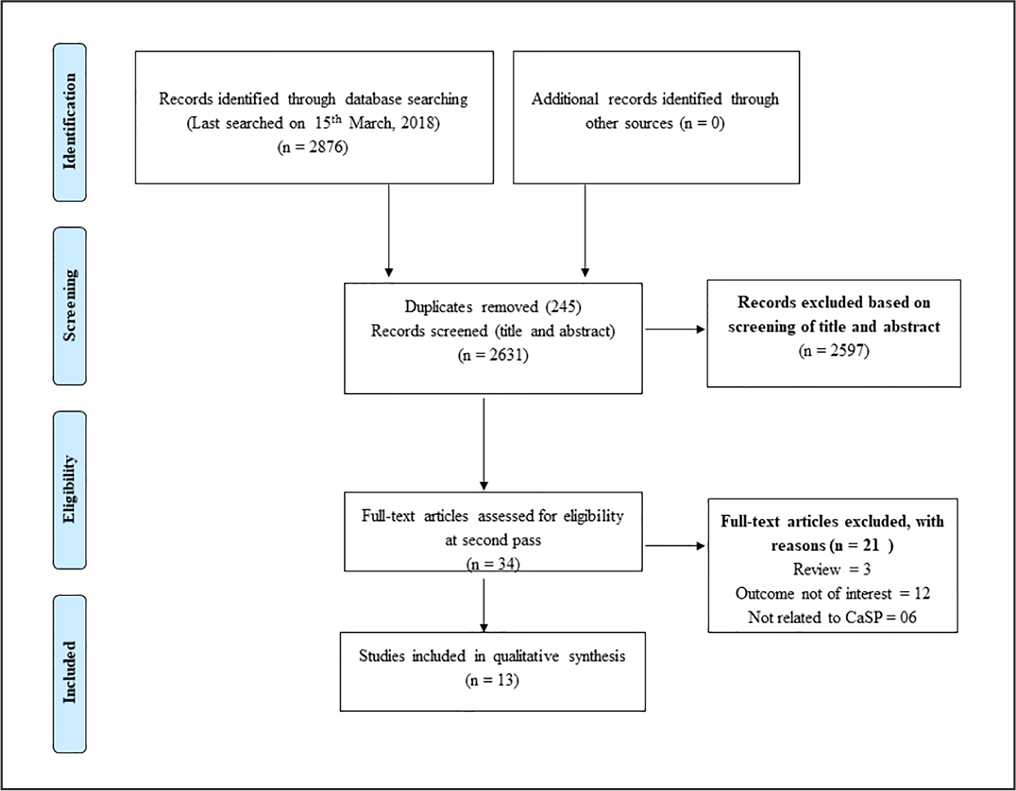
The search strategy identified 2,876 articles after running the pre-specified MeSH terms in different databases. Two independent reviewers assessed the suitability of the articles for inclusion in the study based on screening of the title and abstract in the “first pass”. A total of 2,597 articles were excluded on the basis of title and abstract. The articles selected in the “first pass” were further assessed by conducting a full-text review in the “second pass (n = 34)”. Finally, 13 articles were selected for inclusion in this systematic review. Figure 1 shows the study selection process in detail.
Study Description
All the studies were conducted in India6, 7, 9, 12, 14, 19-25 except one study by Besten and Giambre, 26 which was conducted in the United States. The studies were published between 1995 and 2017 and were in vitro in nature.6, 7, 9, 12, 14, 19-26 Majority of the studies compared the remineralizing potential of CaSP with CPP-ACP. The minimum number of teeth used in any group for comparing the remineralizing potential was four. Microhardness was considered as an important parameter for evaluating the remineralizing potential of CaSP and its comparator in 10 of 13 studies.6 7 12, 14, 19-24 Majority of the studies6, 7, 12, 14, 19-22 assessed the remineralizing potential of CaSP versus its comparator after 7 days of remineralizing agent application, while four studies reported the remineralizing potential of CaSP at 12, 14, 15, and 21 days.21-24
PRISMA Flow Diagram Showing Study Selection Process
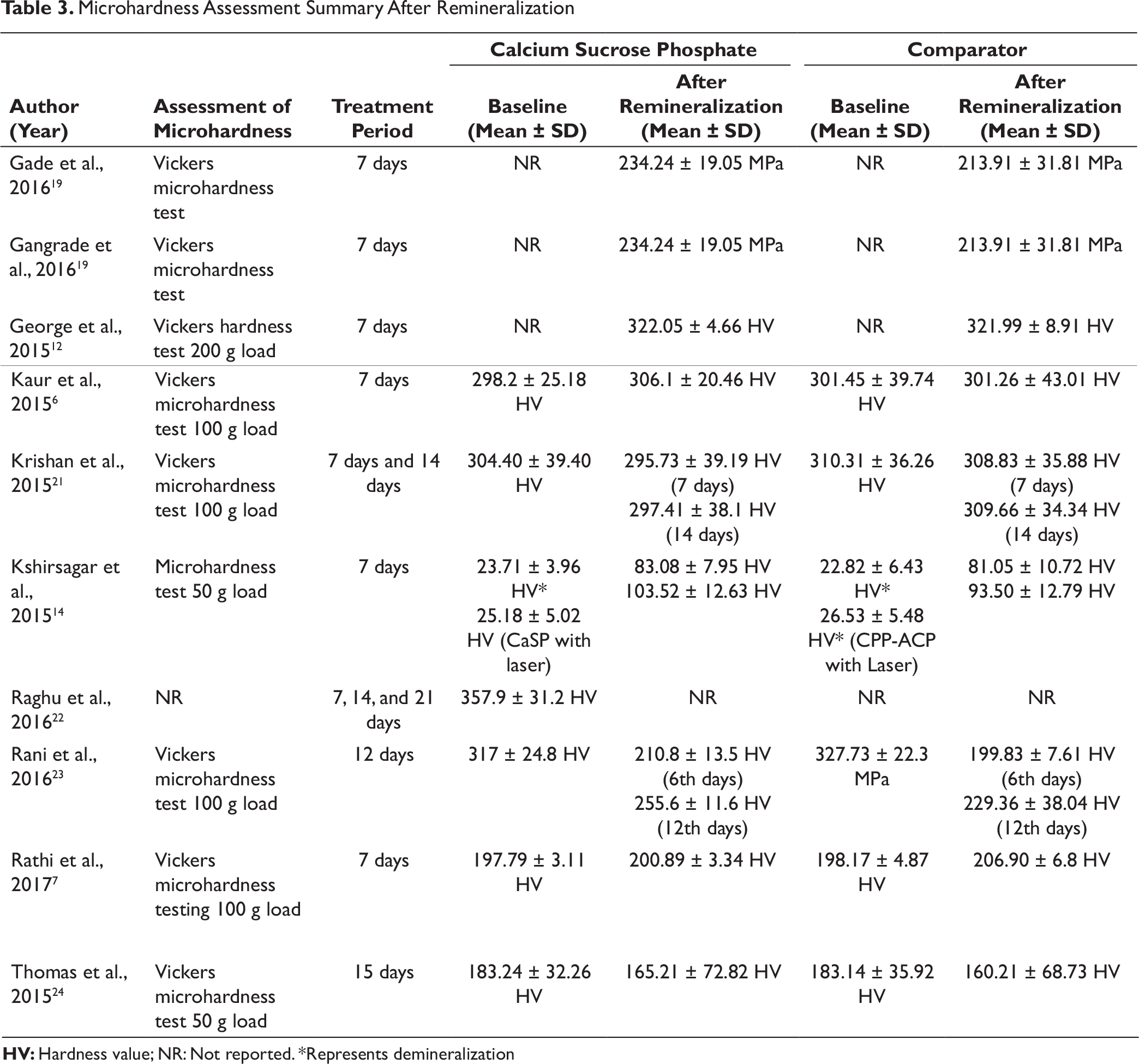
Microhardness Assessment Summary After Remineralization
Quality Assessment
Concerning the quality assessment, none of the studies reported about sample size calculation or blinding of the investigator applying remineralizing agent. Low RoB was observed in the following items: caries-free teeth or restoration, and adherence to the material usage as instructed by the manufacturer (Table 2).
Outcomes
Microhardness Assessment
A total of 10 studies reported the impact on microhardness of enamel after CaSP application (Table 3). Gade et al. 19 reported a higher mean change in the microhardness of enamel following CaSP application, compared with CPP-ACP with fluoride (CPP-ACPF) (between-group difference: 20.33; P = 0.42) and control group (between-group difference: 48.11; P = 0.001). Gangrade et al. 20 compared the remineralizing efficacy of CaSP with CPP-ACPF and suggested a higher mean microhardness of enamel following CaSP application (234.24 ± 19.05 MPa vs. 213.91 ± 31.81 MPa; P > 0.05). However, this difference did not reach statistical significance. George et al. 12 studied the microhardness of enamel with and without fluoride-containing bleaching agent and observed a higher mean microhardness in enamel treated with fluoride-free bleaching agent with an additional CaSP application (322.05 ± 4.66 hardness value [HV] vs. 310.70 ± 1.16 HV).
The CaSP was found to be superior to CPP-ACP in increasing the mean microhardness of bleached enamel (306.1 ± 20.46 HV vs. 30.1.26 ± 43.01 HV; P < 0.01). 6 The percentage increase in microhardness of enamel was higher in CaSP-treated group as compared to CPP-ACP-treated group (6.34% vs. 3.27%). Krishan et al. 21 reported a highly significant increase in the microhardness of enamel after the first (2.87%) and second (2.27%) cycle of remineralization following CaSP administration (P < 0.001). However, the increase was observed only after the first cycle of remineralization with CPP-ACP (P < 0.05).
In an in vitro study, Kshirsagar et al. 14 found a significant difference in microhardness after 7 days of remineralization in CPP-ACP, CaSP, CPP-ACP with laser and CaSP with laser groups (P < 0.05). The remineralization effect was higher when enamel was treated with CaSP with laser compared to CPP-ACP with laser (311.17% vs. 255.42%). The topical application of CaSP tooth cream twice daily for 2 weeks increased the surface smoothness from 2.32 ± 0.09 (when demineralized) to 2.44 ± 0.20 at 21 days of remineralization, as reported by Raghu et al., 22 The authors further concluded that CaSP has a potential to increase the surface microhardness of enamel even after 14 days of brushing. 22
Rani et al. 23 and Thomas et al. 24 demonstrated the superiority of CaSP in increasing the mean surface hardness as compared to CPP-ACP at 12th and 15th day of remineralization. Likewise, Rathi et al. 7 also showed increase in mean microhardness of enamel after CaSP application.
Arresting White Spot Lesion(s) and Restoring of Enamel Colour
Three studies9, 25, 26 assessed the efficiency of CaSP in arresting the white spot lesion(s) on enamel. Besten and Giambre 26 found a significant impact of CaSP paste (either alone or in combination with sodium hypochlorite) in changing the colour of fluorotic enamel to that of normal enamel based on the L* values of fluorotic enamel (L* value is an indicator for the color gradient from white to black). The results reported a decrease in L* values of fluorotic enamel from 79.1 ± 6.6 (pre-treatment) to 72.8 ± 2.7 after CaSP paste application. Similar results were observed when CaSP paste in combination with sodium hypochlorite was used (81.4 ± 4.0 pre-treatment to 70.6 ± 3.40 post-treatment). Moreover, the beneficial effect of CaSP application in restoring the colour of white spot lesion(s) to that of normal enamel was also demonstrated.
In another study, Aggarwal et al. 9 evaluated the protective potential of CaSP as compared to calcium sodium phosphosilicate in controlling the lesion depth. The study revealed that the enamel surface treated with CaSP paste exhibited least lesion depths than the comparator (21.88 µm vs. 35 µm) group. 9 Sargod et al. 25 also found a significant reduction in enamel depth lesion (demineralized: 147.52 ± 11.50 to remineralized: 141.80 ± 13.50) with CaSP application while evaluating its potential on artificial carious lesions.
Discussion
The present systematic review is based on 13 studies assessing the efficacy of CaSP as a remineralizing agent. The results showed a significant improvement in the mean microhardness of enamel post-application of CaSP, compared to CPP-ACP, CPP-ACPF and other remineralizing agents. An increase in the mean microhardness of enamel was evident in all the studies, post-application of CaSP.6, 7, 12, 14, 19-24 In addition, CaSP was also found to be effective in restoring the color of white spot lesion(s) and fluorotic enamel to that of normal enamel. 26 CaSP was also proven to be superior to other remineralizing agents in controlling the lesion depth.9, 25
The CaSP is a white, non-hygroscopic powder with a bland, neutral taste and high water solubility.2, 27 The mechanism by which anticay acts as a cariostatic agent is explained in three pathways: (a) it reduces the rate of demineralization of enamel and increases the rate of remineralization by common ion effect, (b) the sucrose phosphate anion adsorbs directly onto the enamel surface, thereby further inhibiting the process of demineralization, and (c) it actively neutralizes plaque acids.13, 27 The remineralization potential is generally determined by the mean change in microhardness of the enamel and restoration of enamel color to that of normal on application of a remineralizing agent. 22 Besten and Giambre (in 1995) reported that treatment of enamel with 5.25% sodium hypochlorite, followed by CaSP application, and subsequent placement in artificial saliva was effective in returning both white-spot and fluorotic lesions to a normal color. 26 Various studies have reported the pivotal role of CaSP in accelerating the dental enamel remineralization process. In 2016, Raghu et al. reported that twice daily usage (for 14 days) of tooth cream containing CaSP as the main ingredient resulted in an improvement in the surface smoothness. 22 Kaur et al. also found an increase in enamel remineralization after CaSP application and cited high water solubility of CaSP as the primary reason for its remineralization potential, owing to the increased release of free calcium and phosphate ions in comparison to saliva. 6 The remineralization potential of CaSP in terms of significant increase in microhardness after 7 days of use was reported by Kshirsagar et al. 14 CaSP was also found to be a superior remineralizing agent than CPP-ACP in increasing the surface microhardness. 23 CaSP was also found to have plaque-reducing ability. 28
The result of systematic review was in corroboration with the findings of published in vitro studies, which evaluated the remineralizing potential of CaSP and had reported a significant improvement in enamel remineralization after CaSP application. The present review has few strengths and limitations. The strengths being that an exhaustive literature search was done in major databases in addition to hand searching of relevant articles. Second, we have included all the data related to primary outcome and have an unbiased quality assessment using the appropriate tool. The limitations of the study were that all the included studies were in vitro in nature. Also, majority of the studies were conducted in India. The study protocol was not registered in any database. Further, we express our inability to search the grey-literature, and the search was restricted to English language only.
Conclusion
This systematic review suggests that CaSP is an effective remineralizing agent compared to others, such as CPP-ACP and CPP-ACPF, in terms of increasing the mean microhardness of enamel and arresting white spot lesion(s). However, to make the evidence more robust and to generalize the findings, there is a need for well-designed randomized controlled trials, assessing the remineralizing potential of CaSP in vivo conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
Writing support was provided by GCE Solutions through academic funding from Abbott Healthcare Pvt Ltd.