
Abstract
Cephalograms regularly disclose clinically noteworthy incidental findings to orthodontists who maintain a vigilant approach. In recent years, we have consistently identified a specific occurrence in the majority of lateral cephalograms, namely, the occipital spur. This refers to an enlarged external occipital protuberance, a protrusion at the rear of the skull which may manifest in either a smooth, crest, or spine-shaped configuration. Research suggests potential links to factors like brain expansion, adaptation to light levels, relief of neck muscle stress, and the influence of modern habits like smartphone usage in External occipital protuberance enlargement. Studies show a gender predilection, with smooth occipital spur more common in women and spine type more common in men, potentially aiding sex determination in forensics. Occipital spur influences on craniofacial measurements and the potential for causing occipital neuralgia, a condition characterized by pain in the posterior scalp. Management options range from conservative measures to surgical intervention, depending on symptom severity. Hence, this literature review compiles information concerning various types, prevalence, suspected etiology, clinical significance, and approaches to managing occipital spurs.
Keywords
Introduction
As the French philosopher Henri Bergson has quoted “The eye sees only what the mind is prepared to comprehend,” it is widely acknowledged that lateral cephalogram often reveals incidental findings of clinical significance to orthodontists who are keen observers.
1
In recent years, we have consistently observed one such finding in the majority of lateral cephalograms: the occipital spur. In light of our observations and subsequent literature research, we aim to present a comprehensive review on this topic. An occipital spur, known by various terms such as occipital bun, occipital knob, enlarged external occipital protuberance (EOP), enthesophyte, and chignon hook, refers to a distinct bulge or projection of the occipital bone located at the rear of the skull.
2
The tubercle has been known to induce occipital headaches, particularly in individuals engaged in activities like tree climbing or sports such as basketball and volleyball that involve vertical neck movements.
3
Broca initially categorized the enlarged EOP into six anatomical subtypes. Gülekon later simplified this classification into three subtypes. Similarly, Shahar and Sayers
4
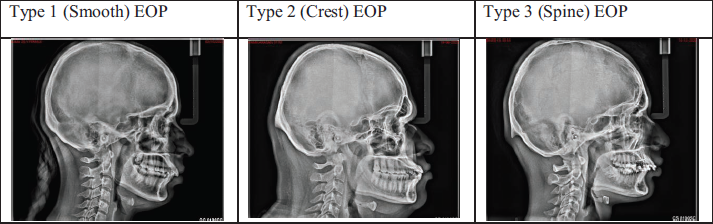
classified an enlarged EOP as one that exceeded 10 mm in size. The three main subtypes are (Figure 1):
Type 1 (smooth) EOP: Natural curvature of the posterior skull, exhibiting a smooth surface without any noticeable protrusion. Type 2 (crest) EOP: Distinct ridge or crest along the posterior aspect of the skull. Type 3 (spine) EOP: Exaggerated or more prominent spine like protrusion at the back of the skull.
Various studies are available in literature with regard to their prevalence. Starting from fossilized Homo sapiens of Europe to current-day modern humans, such as the Sámi, the bushmen of South Africa, and native Australians, have some prevalence of occipital spur. 2 Srivastava et al. 5 found occipital spur in 10% of 30 cadaveric skulls, with average dimensions of approximately 13.40 mm in width, 13.45 mm in length, and 2.43 mm in thickness. Shamsundara et al. 6 identified occipital buns in 22.5% of 213 human skulls, with a higher prevalence of Type 1 among women. Gunacar et al. 7 observed occipital spurs in 11.9% of 1,312 patients through lateral cephalograms. A cross-sectional study conducted in Jordan by Al-Ryalat et al. 8 reviewed thousands of CT scans taken over 2 years, involving 4,409 patients, 1,210 (27.4%) presented with enlarged EOP. There are studies showing sex predilection of occipital spur. Gülekon’s study in 2003 9 involved the examination of 1,000 lateral cephalograms and 694 dry skulls. The radiographic analysis revealed that Type 1 (less prominent) EOP was prevalent in 85.4% of females but only 17.8% in males. In contrast, Type 3 (spine) EOP was found in 63.4% of males but only 4.2% of females. Dry-skull examinations showed a similar pattern, with Type 1 EOP occurring in 67.5% of females and Type 3 EOP in 55.2% of males. Type 2 (crest) EOP, on the other hand, had a relatively equal distribution between sexes and was less valuable for sex determination. These findings highlight a significant gender-based variation in the prevalence of EOP types, with Type 1 being more common in women and Type 3 being more common in men. Similarly, Jacques et al. utilized CT scans to assess EOP volume and detected gender-related differences in occipital spur types. Type I has been found to be more common in women, while Type III is more common in men. Similarly, Shamsundara et al. observed that Type 1 occipital spur was shown to be 67.5% more prevalent in women. Conversely, Gunacar et al. showed spine-type spurs (66.7%; 18/27) were the most common in females, while flat-type spurs (45.2%; 42/39) were the most common in males. Nonetheless, in future research endeavors, it appears that the spine-type EOP could serve as a useful indicator for sex determination in the context of forensic and anthropological studies. Regarding spur length, Cheng et al. made the determination that males tend to have longer spur lengths compared to females, and individuals under 18 years of age exhibit shorter spur lengths than adults. However, it is worth noting that Gunacar et al. pointed out that spur length remained unaffected by age and sex in their findings. Consequently, further studies are warranted to explore the potential utility of spur length in age estimation and sex determination.
The suggested etiology for such a finding is, some researchers suggest that occipital buns might be related to the expansion of the visual cortex in the brain. 10 Another hypothesis proposes that occipital buns could be an adaptation to lower light levels in regions with higher latitudes. 10 Occipital buns may also serve to relieve stress on neck muscles and balance the weight of a heavier facial structure. Multiple studies, including those by Porrino et al., 11 Shahar and Sayers, 13 and Jacques et al. 12 examined the prevalence of an enlarged EOP in relation to smartphone use and digital device engagement. Contrary to expectations, Porrino’s study found no significant connection between iPhone accessibility and EOP enlargement. Shahar suggested that screen-based activities across all age groups, including children, might explain EOP enlargement. 14 Jacques’ research from 2011 to 2019 did not find a significant correlation between smartphone usage and changes in EOP size, despite some enlargement observed in millennials. Intriguingly, the presence of occipital spur in ancient skulls suggests that this phenomenon is not exclusively linked to modern factors, raising questions about its historical prevalence and potential causes.
Clinical Implications of Enlarged Occipital Protuberance
Occipital Spur Influence on Craniofacial Metrics
Cheng et al. 15 revealed that individuals with enlarged EOP tend to exhibit increased linear craniofacial measurements which include anterior and posterior cranial base length, effective length of the maxilla and mandible, ramus height, mandibular body length, facial height index, and lower anterior facial height.
Occipital Neuralgia
The EOP functions as a site of attachment for the nuchal ligament, and the greater occipital nerve penetrates deeply, piercing the trapezius aponeurosis below the superior nuchal ridge. This nerve is responsible for providing sensory innervation to the skin on the posterior scalp. In close proximity, the third occipital nerve runs within 3 mm of the EOP, featuring smaller branches that extend beneath and innervating the C2–C3 facet joint.
Enlarged EOP could potentially exert pressure on these nerves, leading to the condition known as occipital neuralgia. Pain associated with this condition can manifest both at rest and during neck movements. Occipital neuralgia often emerges in late adolescence, coinciding with growth spurts. As the protuberance continues to enlarge, it can result in subperiosteal stretching, leading to tenderness in the affected area.16, 17 Sattur et al. 18 highlighted a case report concerning a traumatic occipital spur fracture, as described in their study. Additionally, Gómez Zubiaur et al. 19 reported an unusual subcutaneous scalp pseudotumor in adolescents, using ultrasonography.
Management of Occipital Spur
People with occipital buns may encounter various symptoms, with the most prevalent ones being tenderness at the rear of the skull, particularly when lying down or moving the neck. 20 Typically, these symptoms can be effectively managed through conservative approaches such as the use of mild pain relievers and soft pillows. However, for cases where symptoms persist and conservative measures are insufficient, a surgical procedure may be considered as a viable option for the reduction of occipital spur and alleviate the associated symptoms.
Conclusion
Lateral cephalograms, routinely utilized by orthodontists for comprehensive assessments, consistently unveil clinically significant incidental findings, with recent attention directed toward the occipital spur observed in the majority of the cephalograms. This distinctive feature, manifesting as an enlarged EOP with a smooth or spine-shaped configuration, prompts a deeper exploration of its potential applications in forensic age estimation and sex determination. Beyond anatomical considerations, the suggested biomechanical role of occipital buns in alleviating neck muscle stress and contributing to facial balance. Surprisingly, studies examining the prevalence of occipital spur in relation to modern habits, such as smartphone use, have yielded unexpected results, challenging assumptions about its exclusive association with contemporary factors. Individuals with an enlarged protuberance tend to exhibit increased linear craniofacial measurements, and as it continues to enlarge, subperiosteal stretching may lead to tenderness. A simple finding from a lateral cephalogram could be of potential benefit to the patient when sufficient knowledge exists in identifying the anomalies related to it. Further studies are needed for their exact evolutionary and functional implications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The authors of this review article have made every effort to adhere to ethical standards and ensure that all information presented is accurate and for images in this review article, appropriate credit is given as required.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
I hereby provide consent for the publication of the manuscript detailed above, including accompanying images contained within the manuscript.