
Abstract
Retaining teeth in their ideal functional and aesthetic positions following orthodontic treatment is known as orthodontic retention. The use of fixed retainers presents challenges in certain cases where veneer crowns need to be applied after orthodontic treatment. Bonding a lingual retainer on the veneer crowns needs special bonding agents. It has questionable bond strength, causes frequent deboning, and requires tedious bonding procedures. Inventory problems also exist. This present article describes an innovative method to handle such special clinical scenarios.
Introduction
In the 19th century, occlusion was considered the most crucial factor for maintaining the stability of teeth following orthodontic treatment. Kneirim 1 was the first person to introduce fixed retainers for orthodontic retention in 1973. It is widely accepted that a retention phase is essential for maintaining the stability of treatment outcomes in recent times.
Additionally, lifelong retention is recommended in certain cases. 2
In some cases, special bonding techniques are needed to bond a lingual retainer on prosthetic crowns, which require additional armamentarium and chairside time. In recent years, bonded retainers have been produced using CAD–CAM systems. CAD–CAM technology has been utilized in dentistry for over 30 years. 3 Research in this field is still scarce, given that the technology is quite new and has only recently emerged. CAD–CAM technology can be utilized to bond veneer crowns efficiently.
Aim
The aim of this article is to present innovative, simple, and cost-effective techniques for bonding a lingual bonded retainer to prosthetic crowns after orthodontic treatment.
Materials and Methods
The materials used are commonly used in clinical practice and are cost-effective (Figure 1):
Lingual retainer wire Light wire plier Etching gel Bonding agent Adhesive Light cure unit Prosthetic crown with a modified ring on the lingual surface Luting cement
Technique
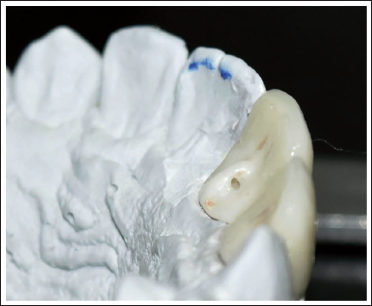
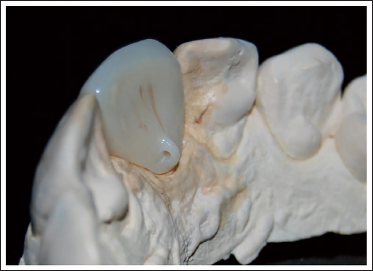
The tooth preparation is done for those teeth that require veneer crowns. A digital impression of the entire arch is taken with the help of an intraoral scanner (Shining 3D Aoralscan 3 Neo) or manual impressions are poured, and the casts are scanned with Medit Identica Hybrid 3D dental scanner. The data are imported as an .stl file into the software (exocad) to design a zirconia crown. While designing the crown in the software, a small tubercle-like attachment is added to the lingual surface of the crown (Figures 1 and 2), and the design is sent for milling, sintering, and layering. After the crown is prepared, a small hole is made in the tubercle area with a handpiece such that it facilitates the passage of the lingual bonded retainer wire through it. Now it is sent for glazing. The crown is cemented onto the prepared tooth with luting cement. The lingual bonded retainer wire is fabricated, passed through the ring first, adapted to the lingual surfaces of anteriors, and then bonded (Figures 3 and 4). The ring is sealed with composite and cured to prevent the free movement of the wire within the ring.
Modified Zirconia Crown with Ring (Case 1).
Modified Zirconia Crown with Ring (Case 2).
After Placement of Lingual Retainer Wire (Case 1).

After Placement of Lingual Retainer Wire (Case 2).

Results
Good stability of orthodontic treatment outcomes was observed with this technique after regular follow-ups for many years.
Discussion
Bach et al., in a systematic review on ceramic bonding, concluded that the most effective protocol is etching with 9.6% hydrofluoric acid (HFA) followed by silane application. 4 Conversely, a study by Kwak et al. examining various conditioning methods on glazed zirconia revealed that aluminum oxide combined with silane offered greater retention than HFA with silane. 5 When bonding to porcelain, applying a silane primer after HFA etching results in strong resin bond strength by forming covalent bonds with both the ceramic and resin.6, 7 In contrast, for bonding to zirconia, alternative methods such as air-particle abrasion and the use of zirconia primers are recommended (Z-Prime Plus, Monobond-S), or adhesive luting cements are needed because zirconia is not readily etched by HFA due to its high crystalline content, and such silane chemistry is ineffective with zirconia.8, 9 Panah et al. have suggested the use of patient-oriented protective measures such as neutralizing agents and rubber dams 10 while using HFA. Since special bonding techniques and bonding agents are needed to bond the veneered crowns and also safety measures like neutralizing agents for HFA and rubber dams are required, the overall cost of the treatment and chairside time will increase. Inventory problems (the need to buy special bonding material for cases which will come once in a while) exist in daily clinical practice because such clinical scenarios are very rarely encountered. In such cases, the techniques described in this article will play a pivotal role in cutting off the cost burden and reducing chairside time.
Advantages
Simple and easy
Economical
Reduced chairside time
Less armamentarium
Stabilization of the retainer wire
Minimal patient discomfort
Reduced bond failure since special bonding techniques are not needed
Less iatrogenic damage to soft tissues
Good patient cooperation can be achieved
Disadvantages
Technique-sensitive
Use of advanced aids like CAD–CAM technology
Conclusion
The authors declare that there are no conflicts of interest regarding the publication of this article.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was taken from the patients.