
Abstract
Background
Perceiving a need for orthodontic treatment is a heuristic process usually conditioned by the interplay between motivational factors and influencing factors in a community with orthodontic awareness and a history of already ongoing or completed orthodontic treatments. Using a verbally assigned index to elicit candid responses, the current study aimed at assessing reluctance toward orthodontic treatment in adolescents with clinically ascertained malocclusion in a community with no prior history of orthodontic treatment.
Objectives
Tribal adolescents from two regions with clinically ascertained malocclusion but no previous access to orthodontic treatment were evaluated for willingness or reluctance to undergo orthodontic treatment using a verbally assigned Simplified Malocclusion Index for Layperson Evaluation (SMILE index).
Methods
2,835 tribal adolescents belonging to the tribal regions of Paderu and Parvathipuram in Andhra Pradesh were questioned to analyze factors related to reluctance toward orthodontic treatment in those with malocclusion. Necessary permission and consent were obtained from the institutional ethical clearance committee, tribal authorities, school authorities, and parents or guardians. Clinical screening employing appropriate infection prevention protocol under natural daylight was used to determine the presence of malocclusion. A verbally assigned SMILE index in the vernacular language of the students with malocclusion was used to record candid responses to analyze possible reluctance toward treatment. Specific reasons for reluctance to undergo treatment were documented and tabulated separately. Pearson chi-square statistical analysis of the data was performed to determine if there was any gender bias.
Results
At Paderu, of the 68% of the tribal adolescents presenting with malocclusion, the verbally assigned SMILE index revealed that 84.03% of the adolescents were reluctant. The chi-square statistical analysis of the data indicated a gender bias (X2 (1, N = 2,016) = 35.99, p < .0001). At Parvathipuram, of the 93% of the tribal adolescents presenting with malocclusion, the SMILE index assigned revealed that 93.05% of the adolescents were reluctant. The chi-square statistical analysis of the data indicated a gender bias (X2 (1, N = 819) = 6.42, p = .11).
Conclusion
The use of the SMILE index allows for a qualitative analysis of reluctance based on the candid subjective inputs from each individual. The study reveals a high degree of orthodontic awareness among the tribal adolescents, and any reluctance toward orthodontic treatment is mainly related to difficulty in access to treatment.
Introduction
The self-perceived treatment need of a patient is usually a nonspecific heuristic decision, as has been highlighted by Hicks and Kluemper, based on a complex interplay of a multitude of influencing factors that may either reinforce acceptance or trigger reluctance. 1 Authors like Shaw and Freeman have indicated that the patient’s desire, usually aimed at an enhanced quality of life, may not always concur with the clinical decision, in that, a patient clinically ascertained with malocclusion may actually be reluctant to undergo treatment as against the possibility of a patient with clinically ascertained ideal occlusion perceiving a presumed insecurity based treatment need.2–5 Of importance in such decision-making is also the influences of the community, parents, and friends or peers, and such influences are missing in regions with no history of prior orthodontic treatment services having been rendered to the community. Tuncer, de Sousa, Wedrychowska-Szulc, and Prabakaran are among the researchers who proposed that decision-making for orthodontic treatment by an individual is based on a varying weightage of perceived psychological or functional benefits.6–9
In the assumption that the endogamous traits and dietary habits of the tribal populations being screened would have helped preserve a phenotype presenting with near-ideal growth and development of jaws, it was anticipated that the prevalence would be with a majority of ideal occlusion and Angle’s Class I malocclusion with minor derangements in alignment.10–15 Abdel-Kader emphasizes that the psychosocial perception of what is normal within a closed community may influence what is perceived as esthetic or not, and this can influence decision-making. This may be in the form of reluctance toward minor derangements that are common within the community with no prior history of orthodontic treatment. 16 This study aimed at eliciting reasons for reluctance among the population after first performing a routine screening to ascertain the prevalence pattern of malocclusion, followed by verbally assigning the Simplified Index for Malocclusion Evaluation.
Doğan et al., attributing a cultural basis, highlighted the difference in perception of esthetics and treatment needs by adolescents and laypersons as against trained clinicians. 17 Trulsson et al. highlighted that most adolescents would finally assume that the decision made was their own with not much of a realization of any external influences, like those of friends or family, and would actually not truly be by their own consent. 18 Decision-making and compliance with treatment are largely influenced by parental support and attitudes, and are often thought to be the single most important influencing factor as highlighted by Lewit and Virolainen. 19 These studies shed light on the ambiguity of the final decision-making process, which may in fact be largely heuristic with only a subconscious conditioning by influencing factors thus requiring proper counseling of both the adolescents and the parents.
Most quantitative and qualitative orthodontic indices evaluate the need for orthodontic treatment solely from the clinician’s standpoint with no correlation with the patient’s quality of life. 20 As these indices evolved, there has been an emphasis on the inclusion of patient-indicated preferences and inputs, further reinforcing the process of informed consent. 21 The SMILE index allows unbiased and candid subjective inputs of the patient to be included, thus making it a patient-centric orthodontic treatment need index. 22
Aims and Objectives
The study aimed to clinically assess any reluctance toward orthodontic treatment based on their own perception of their dentofacial esthetics employing a verbally assigned Simplified Malocclusion Index for Layperson Evaluation (SMILE index). The study also evaluated the interplay of factors responsible for the acceptance or reluctance toward treatment within the community.
Methods
The present study was in adherence to the STROBE statement as per the guidelines highlighted by von Elm et al. 23 Prior announcements were made so that all students were aware of the screening camp to ensure a majority would attend. As almost all adolescents in the region attend school, the sample was a purposive sample. Permissions and consent were obtained from the institutional ethical clearance committee (ANIDS/IEC/2019020), tribal welfare and school authorities and parents or guardians.
Among school-going adolescents belonging to the tribal regions of Paderu and Parvathipuram, present on the day of screening, aged between 13 and 19 years only those presenting with normal growth and development, with no nutritional deficiencies or metabolic disorders were enrolled in the screening process for this study. A final total of 2,835 children present in the schools of both regions were thus enrolled as a purposive sample.
The clinical screening under natural daylight, adhering to infection prevention protocol, helped categorize the observed occlusion into ideal occlusion or o Angle’s three categories of malocclusion and the results were tabulated in Microsoft Excel (Microsoft, USA). While being screened a SMILE index was assigned verbally in their vernacular language while interacting with each adolescent in Telugu to survey the candidates for candid responses related to awareness, self-perceived esthetics and reluctance toward treatment (Tables 1 to 4). Reasons expressed as reluctance toward orthodontic treatment were categorized, documented, and tabulated (Table 5). Students deemed to benefit by way of orthodontic treatment were identified and their responses to the SMILE index were specifically evaluated to analyze their willingness or reluctance toward treatment. The responses were subsequently analyzed based on the score grid of the SMILE Index. 22 A Pearson chi-square statistical analysis was performed using IBM SPSS statistics for Windows (Ver. 25, IBM, New York, USA).
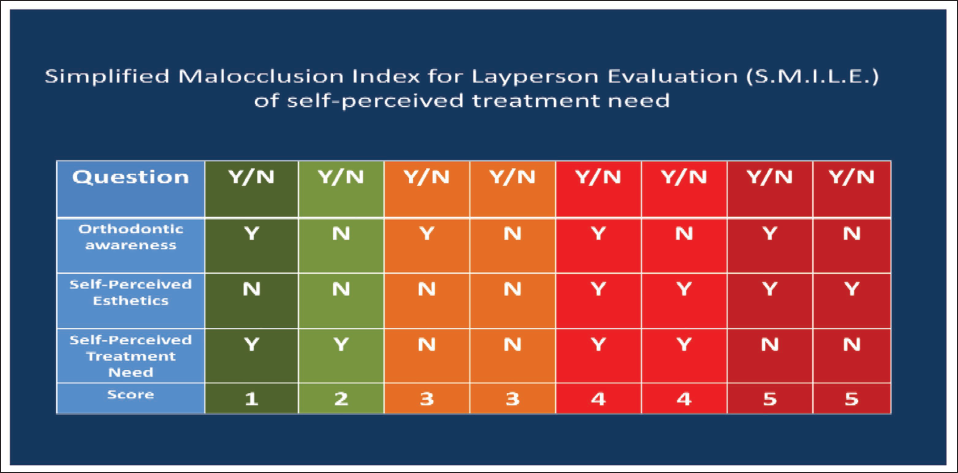
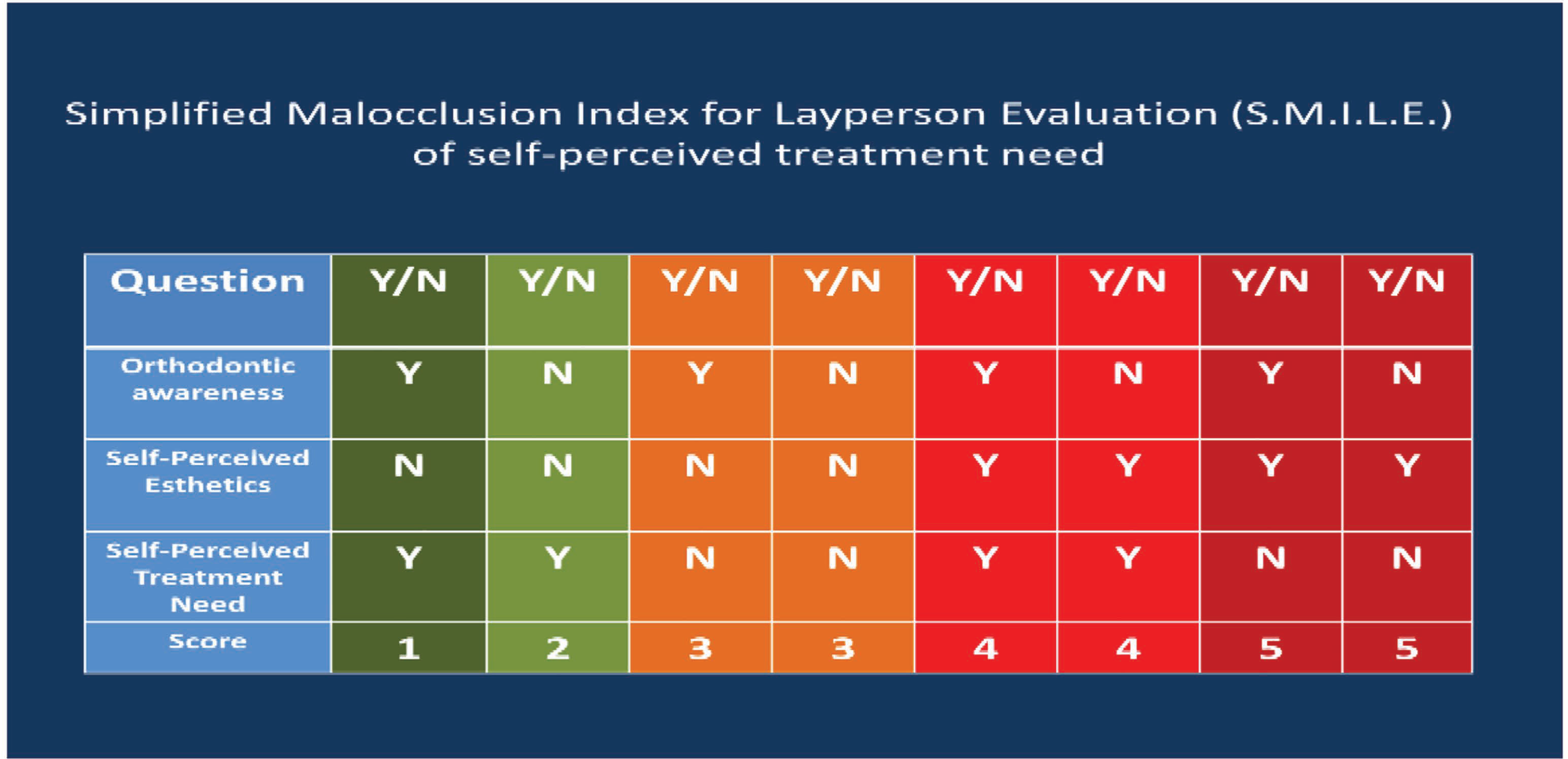
SMILE Index Scoring Grid.
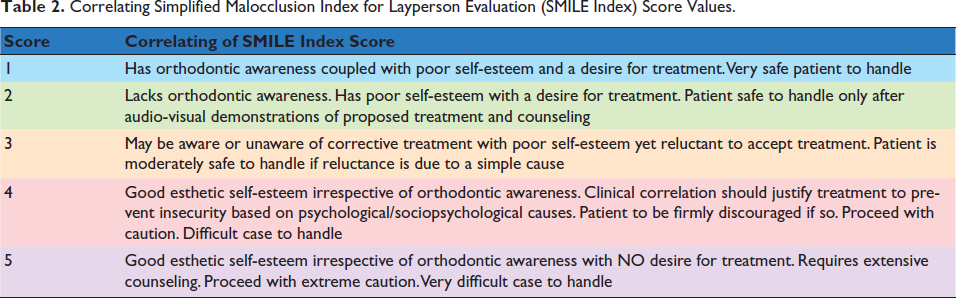
Correlating Simplified Malocclusion Index for Layperson Evaluation (SMILE Index) Score Values.
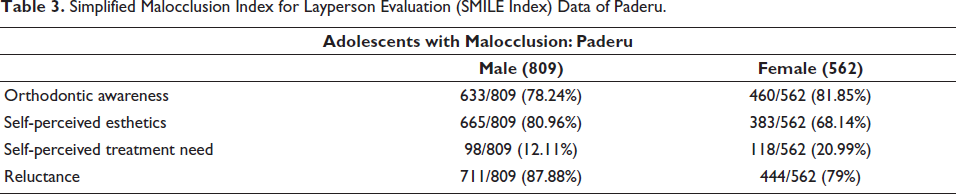
Simplified Malocclusion Index for Layperson Evaluation (SMILE Index) Data of Paderu.
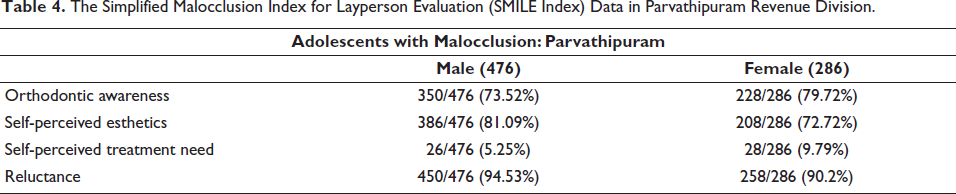
The Simplified Malocclusion Index for Layperson Evaluation (SMILE Index) Data in Parvathipuram Revenue Division.
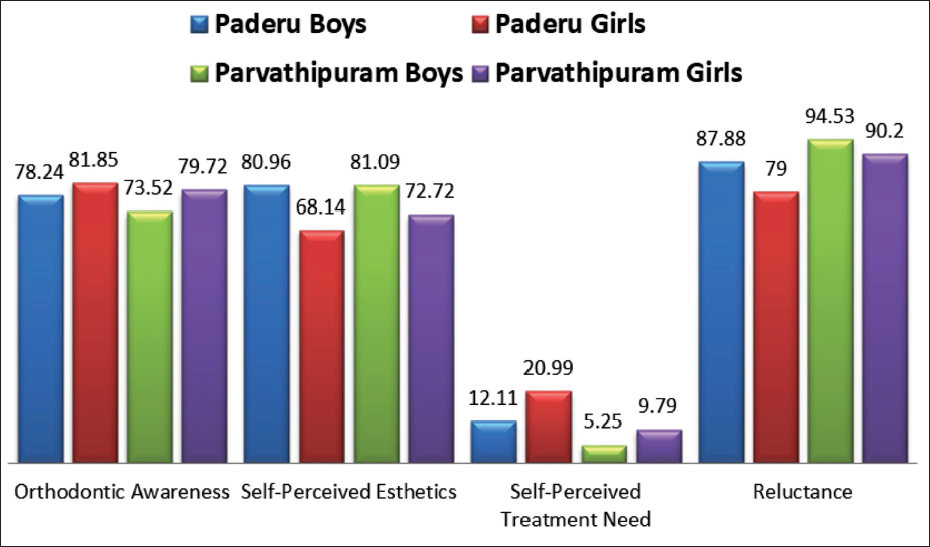
SMILE index: The verbally assigned SMILE index helps elicit unbiased responses from adolescents, and by way of forcing the operator to compare the pattern of answers against a grid to assign a score, elimination of operator bias to an extent is also achieved (Tables 1–4). The index was prior validated against 31 random adolescents with a Cohen’s kappa of 0.93 indicative of very good intraoperator agreement. The percentage distribution of responses is depicted in Figure 1. The data were finally subjected to a Pearson chi-square statistical analysis.
Gender-based Distribution of Simplified Malocclusion Index for Layperson Evaluation (SMILE Index) Response Percentages.
Results
At Paderu, of the 68% of the tribal adolescents presenting with malocclusion, the verbally assigned SMILE index revealed that 84.03% of the adolescents were reluctant. The chi-square statistical analysis of the data indicated a gender bias (X2 (1, N = 2,016) = 35.99, p < .0001).
At Parvathipuram, of the 93% of the tribal adolescents presenting with malocclusion, the SMILE index assigned revealed that 93.05% of the adolescents were reluctant. The chi-square statistical analysis of the data indicated a gender bias (X2 (1, N = 819) = 6.42, p = .11).
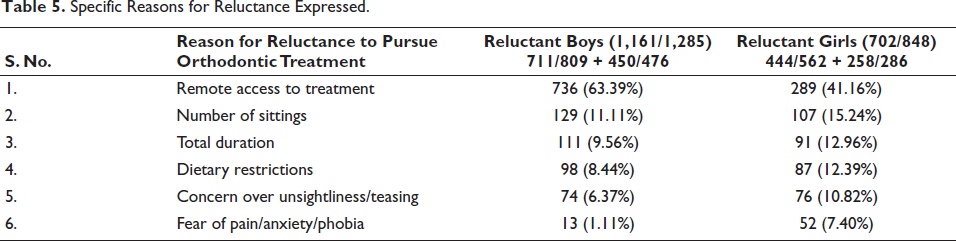
The percentage distribution of various causes of reluctance tabulated indicated the highest percentages for reluctance due to difficulty in accessing treatment with the boys showing higher reluctance (63.39%) than the girls (41.16%).
Discussion
Angle’s Class I malocclusion had a higher prevalence than other classes of malocclusion. The results indicated high levels of reluctance among the adolescents with a slightly higher reluctance expressed by the boys. This might be attributed to the high levels of self-esteem evidenced by way of expressed self-perceived esthetics.
Freeman has highlighted the complexity behind decision-making as related to acceptance or reluctance of treatment in a dental setting. The SMILE Index elicits basic yes or no types of responses related to awareness, perceived esthetics and treatment needs while gleaning information specific to their reluctance if expressed.3–5 Literature indicates that it is not always that parents are truly aware of what their children truly desire, and this is the basis for eliciting unbiased candid opinions from the patients using the SMILE index. 24
The results indicate a good degree of orthodontic awareness, almost equal between the boys and girls, due to the media, information shared by teachers and the dental screening camps conducted in the region and this influence has been highlighted in literature. 25 The results of the SMILE index indicated good levels of orthodontic awareness and esthetic self-esteem resulting in almost no self-perceived need for treatment. The results show that the higher self-esteem as expressed by the boys indirectly influences the low perceived need for orthodontic treatment. So the higher self-esteem resulted in lower perceived treatment needs among the boys. In contrast, the lower self-esteem as compared to the boys influenced a higher self-perceived need for treatment among the girls with lower reluctance toward treatment than the boys. This gender bias has been highlighted in a study by Bleidorn et al. and Phillips et al.26, 27
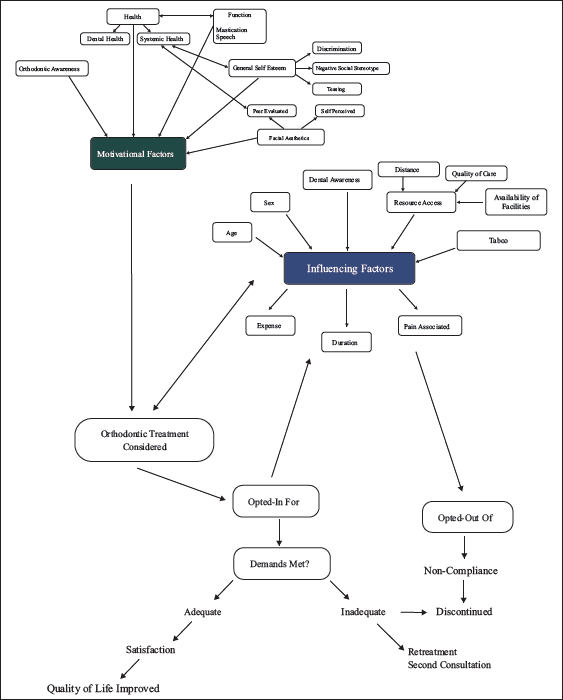
Tung and Kiyak, Tulloch et al., and Russello stressed that children and their accompanying elders seek orthodontic treatment most often for an improvement of appearance with a certain emphasis on improvement of function like speaking or chewing.28–30 The self-perceived need for orthodontic treatment is based on a complex interplay of the primary motivational factors with the negative and positive influences of other factors like prior dental experiences, anxiety or phobia toward dental treatment, or information from peers undergoing orthodontic treatment as summarized in Figure 2. The fine balance between a desire for treatment or reluctance toward the same is related to very simple reasons that include uncertainty, apprehension, worry about the treatment duration or number of visits required, and concern about expenses. The key factor in favor of treatment is that orthodontic treatment can help provide a certain degree of enhancement to both appearance and function, be it speaking or eating. Most adolescents and parents seemed more interested in how best the treatment might influence future social interaction.31–37
Interplay of Factors Related to Acceptance and Reluctance.
Of importance in orthodontic service is for the clinician to offer choices along with balanced advice as to the pros and cons of the choices. Ideally, patient education is aimed at ideal outcomes like patient compliance with a better understanding of both outcomes, inconveniences, and consequences thus minimizing needless anxiety, but it has been documented that there seems to exist a communication gap between the treatment providers and patients in proving this information to its adequate best.
Decision-making is based either on a systematic analysis of pros and cons or may just be essentially based on a heuristic processing influenced by a multitude of conditioning factors. The final decision to undertake orthodontic treatment is usually based on certain influencing factors that modify the patient’s preconceived notions. It is the duty of the clinician to lay emphasis on treatment that addresses the somatic needs of the patient rather than satisfying psychological or social needs. Adolescence witnesses the processes of mental maturation with the concomitant strengthening of certain set patterns of opinions and preferences that are influenced by cultural norms and these vary depending on gender and age.38–42 Any deviation from what is perceived as the accepted norm within a community is usually a negatively perceived aspect of oral health quality of life and thus the prime cause for orthodontic treatment needs.43–45 de Sousa et al. have indicated that there may be a conflict between the clinically assessed treatment need and the patient’s self-perceived need.7, 46
Of interest is the process by which the clinician has to convince both the adolescent and parent about the merits of orthodontic treatment after the clinical detection of malocclusion. If the child and parent can be made suitably aware of the existing malalignment and how the treatment can remedy this by way of explanation and graphic examples, most often by using pre- and posttreatment casts and photographs in conjunction with animated video clips or educational phone applications, then the first obstacle toward orthodontic treatment is cast aside with ease. 47
The main causes of reluctance toward orthodontic treatment, as expressed by the adolescents (Table 5), seem to highlight problems related to accessing treatment more than the fear of treatment. As orthodontic treatment was new to the community, the questions posed were very practical as each adolescent tried reasoning with themselves as to whether it would be feasible or not. To make it easier for the children, the query posed during the interaction with them was to question their willingness to come forward for treatment if two obstacles could be taken care of. One is making the treatment facility available close at hand and the second is the possibility of the treatment being offered for free or at a highly subsidized price. Poverty has been stressed upon as one of the key reasons for neglect of a child’s health and the same can be said to be true with regard to either interceptive or regular orthodontic treatment. 48 Once the question of access and expense were removed from the equation, there seemed to be a very high willingness to undergo orthodontic treatment.
Specific Reasons for Reluctance Expressed.
Among other barriers toward undergoing treatment, as discussed by researchers, there is a stark difference seen within groups that have had a prior experience as compared to groups with no prior experience. The same can be seen as related to the role played by peers. In a community where almost all adolescents undergo orthodontic treatment at a given age, there is most often a reassurance provided by peers and a certain degree of peer pressure that adds to the motivation to undergo treatment.2, 19 This would be lacking in communities where not many children undergo treatment, and the child desirous of undergoing treatment may in fact express reluctance based on the fear of ridicule from peers. A certain degree of fear, apprehension, and anxiety with no specific reason is bound to be there among children interacting with a clinician most often related to queries about teeth needing to be removed and the related pain. In communities where orthodontic treatment is commonplace, a common question would also relate to discomfort and pain related to orthodontic treatment but this would not feature as a priority question in communities where orthodontic treatment has not become commonplace.
Literature highlights a multitude of factors influencing decision-making, and this interplay of factors has been highlighted as the complexities behind self-perceived orthodontic treatment need in Figure 2.2, 18, 25 Of main interest here, from an ethical standpoint, is not one of taking up a child for treatment just because the parent strongly believes the child has a need for correction when none is required.25, 35 It is rather a scenario in which a child who has been clinically judged as requiring treatment is being guided and counseled in a way to reinforce willingness and acceptance. The next step would be to form a connection with the parent or guardian by way of a very honest and clear discussion thus enhancing the domestic support and reassurance factor for the child as a powerful reinforcement of motivation.18, 24 As with any long-term venture, successful treatment starts with efficient clinical documentation and detailed discussions with the adolescent and parent or guardian first individually and then together to be able to smoothen out any wrinkles that might exist due to apprehension based on uncertainties. Patient desires and expectations are to be kept in mind as orthodontic treatment follows a sequence or schedule and requires reinforcement of encouragement and highlighting of positive results at each checkpoint.
Conclusion
This article has aimed at highlighting critical causes for reluctance toward orthodontic treatment among adolescents in two tribal communities with no history of prior completed or ongoing orthodontic treatments within the community. A community with a history of prior treatments usually has the influence of peer pressure among adolescents. The SMILE index aims at eliciting a candid response from the adolescent without parental pressure or peer influences. Gaining in-roads into such communities requires the identification of points of reluctance that can be easily remedied by appropriate actions. The points of reluctance highlighted in this study were the difficulty of access to orthodontic treatment and the apprehension regarding expense both of which could be addressed. Of added importance is to be able to gather an unbiased opinion pertaining to the treatment needs decision from both the adolescent and the parent or guardian to help render better services with informed consent of the parent or guardian and informed assent of the minor all through the process of orthodontic treatment. No child who deserves treatment should be left untreated. Ensuring that such treatment needs are met while overcoming various barriers is one of the biggest skills a clinician can possess in the pursuit of serving a community.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Permissions and consent were obtained from the institutional ethical clearance committee (ANIDS/IEC/2019020).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.