
Abstract
Objective
To evaluate the changes in buccal corridor and smile index, with respect to age and gender, in a randomly selected sample of the North Indian population.
Materials and Methods
Perioral musculature of 195 subjects (divided into three age groups) was recorded using standardized videographic method. The frame representing subject’s “widest posed smile,” was selected and analyzed to evaluate selected smile parameters.
Results
Buccal corridor decreased significantly for overall as well as female sample population, whereas it was fairly unchanged for males. No significant variation was noted for smile index.
Conclusions
As a person ages, the smile gets narrower vertically as well as transversely, with the change being greater in the transverse dimension. Age-related changes must be considered for delivering long-lasting orthodontic results.
Introduction
Current times are witnessing an increasing number of adult patients seeking orthodontic correction for enhancement of dental and facial aesthetics. “Time” has been recognized and accepted as the fourth dimension, affecting smile dynamics, thereby changing the desired parameters of facial aesthetics with age.1–4 What appears normal at a given age is most likely to undergo substantial change in due course of time. Guidelines followed for a young/adolescent age group would not be appropriate when treating adults. Changes at the skeletal and soft tissue cellular level, as well as in muscle structure and function, have been shown to affect the human face with age.5, 6 Ethnicity, sex, and racial background are also known determinants of facial morphology.7, 8 This necessitates an in-depth knowledge of age-related and gender-specific changes in smile dynamics when planning orthodontic treatment for patients of varying age groups.
It is traditionally seen that smile/aesthetics is evaluated primarily in the vertical and anteroposterior dimension, with the horizontal dimension often neglected. Numerous studies have reported aging smile with focus on vertical changes.1–8 Not many studies have focused on the horizontal dimension of smile aesthetics. Two very important aspects, the “buccal corridor” and “smile index” which despite being integral to good facial aesthetics and potentially affected by orthodontic treatment, find little description in orthodontic literature.
The presence of buccal corridor spaces was originally appraised by Frush and Fisher. It is the space between the maxillary posterior teeth and the corner of the mouth, which is visible during smiling, as black or dark spaces. 9 Orthodontic opinion regarding desired buccal corridor aesthetics varies from minimal to moderate. Another important and often neglected component is the “smile index” which was introduced by Ackerman et al.10, 11 as a soft tissue determinant of smile. Nanda et al. 1 reported that with age, the smile gets wider in the transverse and narrower in the vertical dimension, with a significant increase in smile index. Pertinent knowledge of age-related changes expected in the buccal corridor and smile index can help the orthodontist deliver long-lasting results for patients of all age groups and augment dentofacial aesthetics for adult patients.
Thus, the present cross-sectional study was done to evaluate the age-related and gender-specific changes in buccal corridor and smile index on smiling, in a randomly selected sample of the North Indian population using dynamic video recording for documenting the smile.
Materials and Methods
Subjects were selected randomly from among the patients and guardians of patients presenting to various departments, as well as students, residents, and faculty of the institute.
Inclusion Criteria
Age between 15 and 55 years
No history of orthodontic treatment
Exclusion Criteria
Compromised dentition with missing teeth
Any cosmetic/prosthodontic dental work, visible when smiling
Any gross dental/facial asymmetry
Excessive attrition of teeth
Any irregularity or surgery done on lips
Inability to establish patient’s natural head position
The subjects who agreed to voluntarily participate were explained the nature of the study and a signed consent was taken. Study sample consisted of 195 subjects (96 males and 99 females), divided into 3 age groups (group I: 15–25 years; group II: 30–40 years; group III: 45–55 years). The subgroups consisted of 32 males and 33 females, respectively.
When taking a static photograph, subjects may sometimes not adequately hold the position in the widest posed smile for accurate capture. With a video recording of the posed smile, it can be later evaluated frame by frame to determine and select the widest posed smile to be used for the study. Videographic setup was used as subject tends to be less conscious. 12
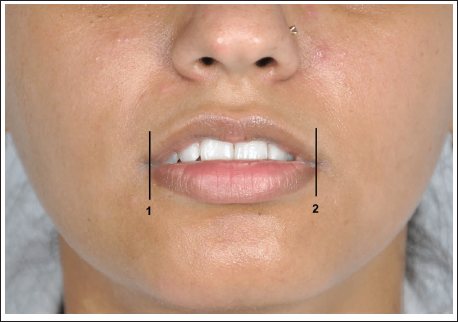
The lines drawn on the resting frame photograph (Figure 1) Right commissure of mouth Left commissure of mouth
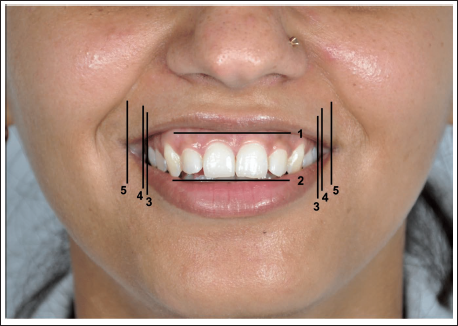
The lines drawn on the smiling photograph (Figure 2) Stomion superius: most inferior point of tubercle of upper lip Stomion inferius: most superior point of lower lip Right and left visible maxillary dental boundary Right and left inner commissures of mouth Right and left outer commissures of mouth
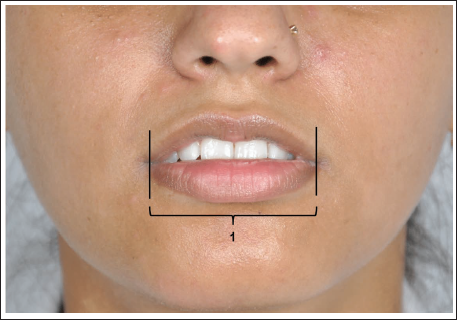
The following measurement was recorded on rest frame (Figure 3) Intercommissure width (ICW)
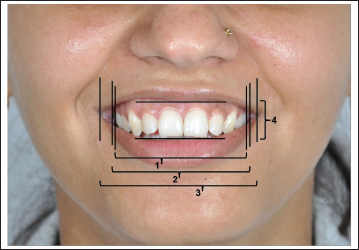
The following measurements were recorded on smiling frame (Figure 4) Visible maxillary dental width (VMDW) Inner intercommissure width (IICW) Outer intercommissure width (OICW) Interlabial gap (ILG)
Representative Photo (at Rest and Widest Posed Smile) of Group II and Group III.

Figures 1 to 4 12 depict study variables using photograph of age group I whereas Figure 5 shows representative photographs of age group II and III.
The following values were calculated from the above readings:
Buccal corridor: The percentage of inner commissure width occupied by the buccal corridor space.Buccal corridor = (IICW – VMDW)/IICW × 100 Smile index: Inner intercommissural width divided by the ILG during a smile.
12
Smile index = IICW/ILG Change in ICW: Difference between OICW on smiling and ICW at rest.
The data were analyzed using SPSS version 16 software. Analysis of variance (ANOVA) and post-hoc least significant difference (LSD) tests were done to evaluate the study parameters. Statistical significance was set at 5% (p < .05).
Results
Significant differences were noted in the pattern of variation of the study parameters with age for the male and female population (Tables 1–4).
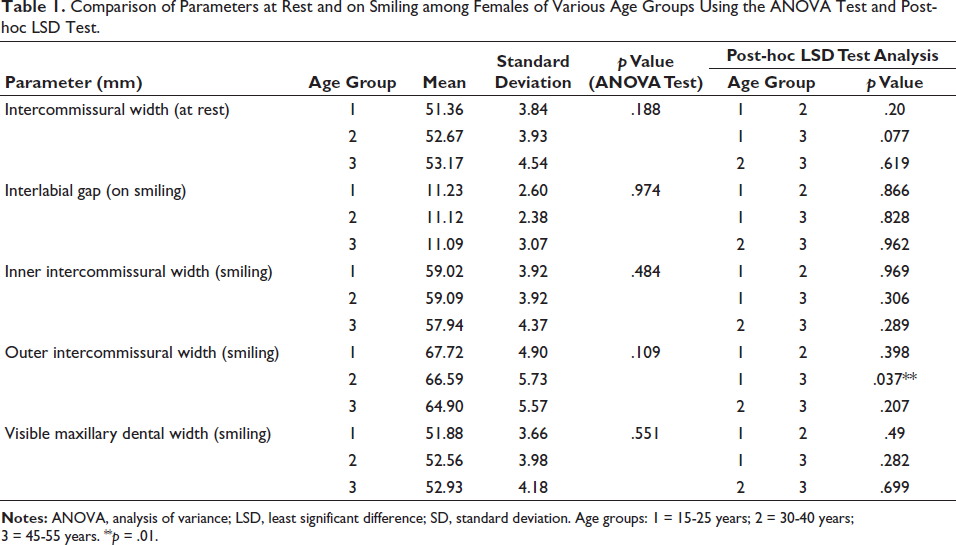
Comparison of Parameters at Rest and on Smiling among Females of Various Age Groups Using the ANOVA Test and Post-hoc LSD Test.
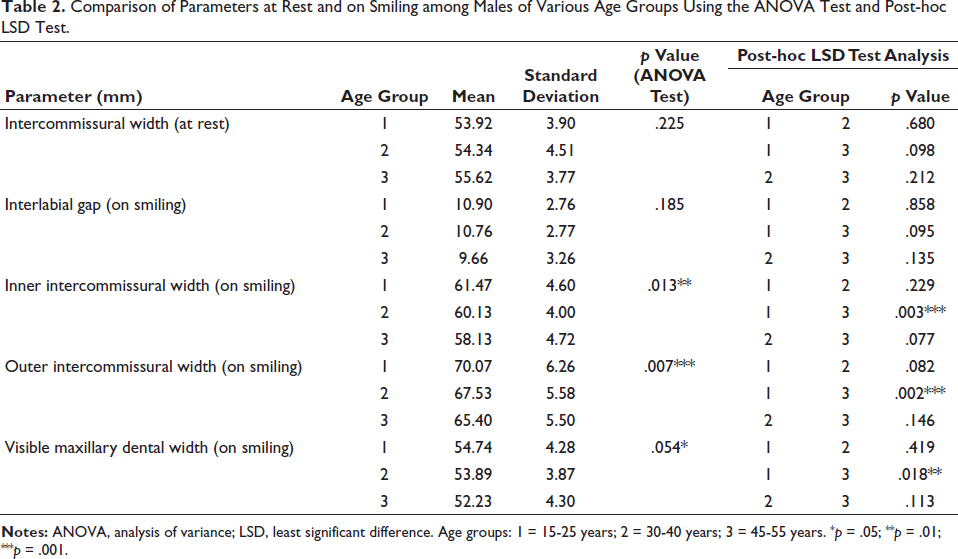
Comparison of Parameters at Rest and on Smiling among Males of Various Age Groups Using the ANOVA Test and Post-hoc LSD Test.
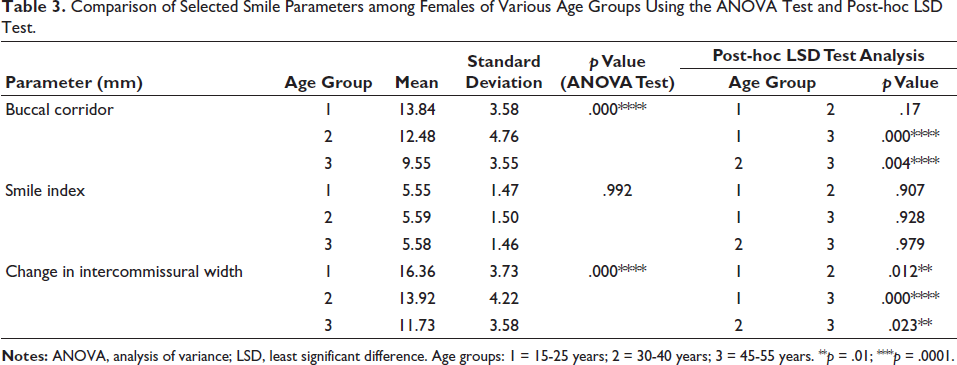
Comparison of Selected Smile Parameters among Females of Various Age Groups Using the ANOVA Test and Post-hoc LSD Test.
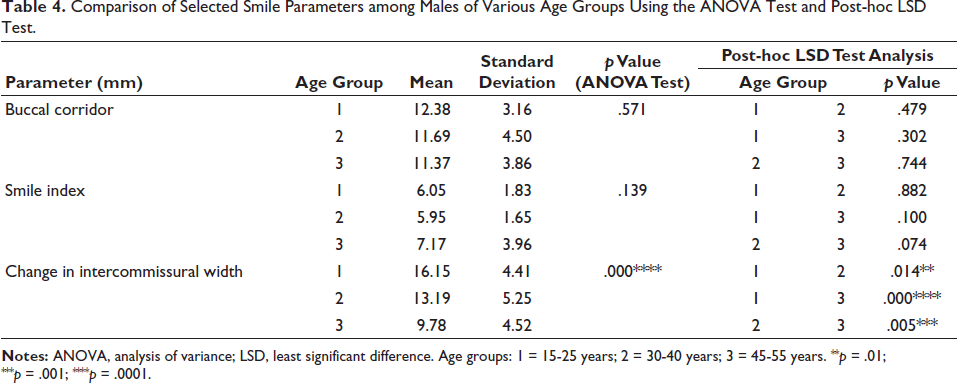
Comparison of Selected Smile Parameters among Males of Various Age Groups Using the ANOVA Test and Post-hoc LSD Test.
On the resting frame, the mean ICW showed a gradual nonsignificant increase with age for both sexes (Tables 1 and 2). On smiling frame, the ILG and IICW decreased nonsignificantly with age for both sexes (Tables 1 and 2). Mild significance was noted for IICW between group I versus group III for male subgroup (Table 2).
OICW for both sexes decreased considerably with age, which was significant for males (Change was mainly noticeable between group I vs group III) (Tables 1 and 2). The VMDW was fairly constant across all ages. Marginally significant reduction was noted among male subgroup, with mild significance between group I versus group III (Tables 1 and 2).
The mean buccal corridor % on smiling showed a significant decrease with age for the female study population. The decrease was significant between group II versus group III (p = .020) and highly significant between group I versus group III (p = .000). However, it was fairly constant for male population across all age groups (Tables 3 and 4).
The smile index varied nonsignificantly across different age groups for both sexes. In group III, smile index was greater for males than females (Tables 3 and 4). The change in intercommissural width for both sexes decreased significantly with age, with a similar level of significance for all intergroup comparisons (Tables 3 and 4).
Discussion
Increased patient awareness and availability of quality dental care have led to a constant surge in the number of patients opting for orthodontic correction, especially at later stages in life. Aesthetic and beauty perceptions tend to differ for young and adult patients. Orthodontists are required to deliver stable results that are acceptable not only at the time of treatment but will not lose relevance in due course of time as the person ages. This is possible only by having an in-depth understanding of the role of the fourth dimension, “time,” in the alteration of smile dynamics with age.
Maxillary and mandibular incisor display, gingival display, smile arc, and other dental parameters evaluated in the vertical dimension are usually more relied upon when judging smile aesthetics before/after, with/without orthodontic treatment. Changes in these parameters with age have been widely studied and reported.1, 2, 12
However, among the many aspects of smile dynamics, buccal corridor and smile index are two very important parameters in the horizontal dimension that have a significant bearing on smile aesthetics yet are often neglected and less talked about, especially the changes with age.
Buccal Corridor
Buccal corridor is one of the most important and integral aspects of smile attractiveness (assessed in the horizontal dimension), which finds mention in dental literature with varying definitions and significance.12, 13 The concept of appropriate buccal corridor has been emphasized over the years for denture aesthetics in prosthodontic literature. Too much buccal corridor results in large unaesthetic spaces, while too little looks artificial and is considered an indicator of bad aesthetics of prosthetic denture.
Buccal corridor space is an entity that falls within the ambit of orthodontic correction, and can easily be corroborated with other concepts of orthodontic diagnosis and treatment planning such as arch width and form, occlusal function, and the extraction/nonextraction controversy.
Regardless of the definition used, it is essential to be watchful for adequate and constant lighting while recording/evaluating the smile, as it affects the appearance of buccal corridor space. 10
Contrasting observations have been reported by various studies, regarding the significance of buccal corridor for attractiveness of smile. Moore et al. 12 found broader smiles (minimal buccal corridor) to be acceptable and appreciated as most attractive by laypersons; Parekh et al. 13 found that both orthodontists and laypersons rated excessive buccal corridors to be as less attractive whereas, Husley 14 found the buccal corridor ratio to be of no significance for an attractive smile; Roden-Johnson et al. 15 reported that buccal corridor spaces did not have an effect on the smile ratings of orthodontists, general dentists, and laypersons.
These studies have documented their results based on digitally altered images rated by clinicians and laypersons for attractiveness. Changes in the buccal corridor with age have been inadequately researched/documented. The present study was thereby undertaken to evaluate buccal corridor changes with age.
Studies have reported a nonsignificant decrease in buccal corridor with age. 16 However, the present study noted a significant decrease of 2.67% in buccal corridor, from the youngest to the oldest age group. The decrease was significant for females but nonsignificant for the male subgroup. Also, no significant intragroup difference among the sexes was found at any particular age.
The change in buccal corridor can be attributed to a change in either of its determinant boundaries, that is, dental arch width (which changes with age and can also be altered by orthodontic treatment) or the inner intercommissural width on smiling (which changes with age).
For the female population, the visible maxillary dental width increased with marginal significance whereas, the inner intercommissural width decreased nonsignificantly, resulting in a significant decrease in the percentage of buccal corridor for females with age. In contrast, the male population showed a decrease in both the visible maxillary dental width as well as the inner intercommissural width. This resulted in a nonsignificant decrease in buccal corridor with age.
Nanda et al. 1 have reported an increase in buccal corridor with age which they attributed to the fact that smiles grow wider transversely and narrower vertically. Observations of the present study, however, do not agree with the same.
Decreased OICW and IICW as well as ILG, all are indicative of the overall decreased inherent ability of perioral musculature in producing a smile. Lip activity appears to decrease both in vertical and horizontal dimension. Significant decrease in OICW concurrent with a nonsignificant decrease in IICW is indicative of thinning of lips.
Narrow maxillary arch and extraction in the upper dentition can be attributed as the primary cause of wide buccal corridor. 17 The anterior-posterior position of the maxilla and the rotation of the upper molars are other factors influencing the same. 18
Some orthodontists have advocated expansion of maxilla (even in the absence of crossbites) in order to reduce buccal corridor space. Others have recommended nonextraction treatment to maintain arch width, thereby maintaining the original buccal corridor space (Johnson and Smith were one of the first to propose this idea). 19 They found no difference in smile aesthetics between extraction and nonextraction cases. Kim 20 and Choma 21 reported that extraction of premolar neither leads to narrowing of arch width nor does it negatively impact the perception of smile aesthetics.
It can be inferred that extraction is not likely to change the buccal corridor space but expansion does increase maxillary arch width, thereby decreasing buccal corridor.
Arch expansion when chosen to treat narrow maxillary arch/crossbite is acceptable and improves aesthetics at any age. However, when considering the same for borderline space requirement considerations, it needs to be gauged differently in adolescents/young versus adult patients.
In adolescent borderline cases, rapid maxillary expansion (RME) to increase arch width is often preferred over extractions for creation of space. It is expected to match up well as the face matures into adulthood. On the contrary, for adult borderline cases, arch expansion should be opted with caution as the face has already reached maturity and is expected to undergo aging changes. Especially for adult females, expansion may not be the best option as the buccal corridor is expected to decrease further with age. For adult males, expansion could still be opted if needed, as the BC does not change much with age.
Smile Index
Smile index can be defined as the area framed by the lips during “social smile.” Ackerman et al. 10 introduced the concept of smile index as a soft tissue determinant of smile. It is derived as the smile width divided by the smile height, thus dependent on two variables: the IICW and interlabial gap on smiling. Nanda et al. 1 reported a significant increase of 2.42 mm from 15 to 50 years of age. According to them, as a person ages, the smile tends to get relatively wider transversely and narrower vertically.
However, the present study on the contrary found that smile index does not change significantly with age. A very mild and nonsignificant increase in smile index was noted, with age in males (increase by 0.57 mm). This could be attributed to the fact that with age, both the ILG and the intercommissural width decreased considerably.
By analyzing the results of the three determinant variables (ILG, intercommissural width, and smile index) together, it was concluded that with age, the smile of a person narrows both vertically as well as transversely, the magnitude of change being slightly greater in the transverse direction. However, its mean value is significantly greater for males than females, as females tend to smile more fully than males.
Change in ICW
The change in intercommissural width from rest to smile also decreased with age. From the youngest to the oldest age group, it decreased by 5.49 mm which was highly significant. This is partly due to increase in resting ICW (1.76 mm) and largely on account of decrease in the OICW on smiling (3.73 mm). These results were concordant with the idea that with age there is a decrease in both, the resting tone and elasticity as well as the activity and function of muscles involved in retraction and elevation of the corners of the mouth when smiling. The magnitude of decrease for change in intercommissural width with age was greater for males (decreased by 6.37 mm) as compared to females (decreased by 4.63 mm), indicating a greater loss of function of elevator muscles of the corner of mouth in males.
By and large, most orthodontic diagnosis and treatment is provided during late childhood to early adolescent years, with retention of orthodontic results through adult life. Patterns observed in this study can aid the orthodontist in delivering results that truly last and stay relevant for a lifetime. Sarver and Ackerman 10 have stated that aesthetic considerations are of paramount importance during treatment planning; however, rigid set of rules can certainly not be applied to this process because almost an infinite variety of faces can be aesthetic. As rigid aesthetic standards do not exist, the orthodontist must surely possess an eye for beauty, hand skills for art, and knowledge of an individual’s smile window anatomy and function relevant at various age brackets. It is important to have general age-related and gender-specific guidelines that aid the clinician to optimize dentofacial aesthetics while satisfying other treatment goals at any age. The present study establishes the general pattern of change in selected smile parameters (buccal corridor and smile index) that individuals of the North Indian population would be expected to undergo, with age.
Conclusion
North Indian population exhibits significant age-related and gender-specific changes in selected smile attributes with age.
As a person ages, the smile gets narrower both in the horizontal and vertical dimensions, the magnitude of change (decrease) being slightly greater in the horizontal dimension.
When treating borderline cases, if the ideal buccal corridor and smile index are not attainable, it would be acceptable to end treatment for females with marginally higher buccal corridor spaces, but not so for males.
For borderline adult female cases, arch expansion (instead of extraction) must be approached with caution (as further decrease in buccal corridor is expected with age, thereby leading to loss of relevance of orthodontic treatment results with time).
For borderline adult male cases, arch expansion if needed can be considered with acceptable long-term aesthetic results, as the buccal corridor does not undergo any significant change with age.
These suggestions hold relevance if and only where the ideal cannot be established. When deviating from the same, the expected age-appropriate and gender-specific changes must be borne in mind while deciding where to finish the case.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Approval was obtained from the Ethical Committee of Santosh University to conduct the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.