
Abstract
Background
The purpose of this research was to compare the adhesive residual score/adhesive remnant index (ARI) and shear bond endurance between the two orthodontic bonding systems for zirconia surface bonding: Self-etch (Scotchbond Universal) and total-etch (Transbond XT).
Materials and Methods
Color-coded acrylic blocks embedded with zirconia slabs were prepared, and the orthodontic brackets (ceramic) were bonded using either the total-etch or self-etch system. Group 1, represented by pink-colored blocks (N = 12), accommodated 12 zirconia surfaces using the total-etch system, while Group 2, represented purple-colored blocks (N = 12), also housed zirconia surfaces using the self-etch system. The shear bond strength was evaluated using an Instron Universal Testing Machine, and ARI scoring was done upon debonding. The statistical software SPSS was used for the analyses.
Results
The average bonding strength for the Scotchbond Universal etch system was 6.21 ± 0.76 MPa, while for the total-etch system, it was 5.59 ± 1.37 MPa. The ARI scores revealed that 83% of surfaces bonded with the self-etch system had no adhesive residue (ARI score 0), compared to 66% for the total-etch system.
Conclusion
The self-etch bonding agent demonstrated superior bond strength (6.2 MPa) compared to the total-etch system (5.6 MPa). Furthermore, it exhibited better ARI scores, indicating minimal adhesive residue. These findings suggest that the self-etch system is preferable for bonding ceramic brackets to zirconia crowns, offering improved bonding efficacy and ease of clean-up.
Introduction
The use of fixed appliances by adult patients has increased significantly in the area of orthodontics in recent years. This trend is attributed to various factors, including the growing emphasis on aesthetics throughout orthodontic treatment. As a result, ceramic brackets have gained widespread popularity, aligning with the increasing prevalence of ceramic prosthetic teeth among adults seeking orthodontic care. 1 It is now typical to directly bind ceramic brackets to ceramic surfaces, which calls for a careful analysis of the bond strength between these elements.
The development of one-step adhesives with 10-methacryloyloxydecyl dihydrogen phosphate (MDP) as the monomer is a noteworthy development among the many bonding agents available for direct bonding in orthodontics. The absence of additional primers simplifies bonding to prosthetic surfaces, while the presence of aqueous components in the primers ensures efficacy even in a moist oral environment. 2
Any material that is employed for direct bonding in mechanotherapy with fixed appliances must first achieve a suitable shear bond strength. Typically, adhesive solutions on enamel have bond strength values of 8-30 MPa, 3 which can withstand the stresses that are present in the oral environment. Additionally, the material should facilitate easy removal without residue, protecting both the enamel and prosthetic crowns from damage. 4 For bonding brackets on enamel surfaces, a shear bond strength of 4-10 MPa is recommended. 5 To avoid a significant amount of bracket debonding, the shear bond strength of prosthetic surfaces and restorative materials must be equal to or greater than that of enamel.
In light of this, selecting the bonding technique that provides the best adhesive remnant index (ARI) score and adequate bonding strength is essential. While much research has examined the bonding efficiency of metallic brackets on the surfaces of prosthesis using various adhesives,6–8 none have specifically examined the bonding efficacy of ceramic brackets on zirconia crowns. This research gap underscores the need for a comprehensive study to evaluate the bond strength of two different bonding agents (Scotchbond, the universal bonding agent, and Transbond XT primer), which were used for bonding ceramic brackets on zirconia surfaces.
In addition to determining the bonding efficacy, the study also aims to evaluate the adhesive residual score upon debonding the ceramic brackets when using the two bonding agents. The ARI score provides valuable insights into the mode of bracket failure and the amount of adhesive/residues left on the tooth or any prosthetic surfaces after the removal of brackets. Understanding the residual adhesive score is crucial for optimizing bonding protocols and minimizing potential damage to tooth enamel or prosthetic crowns during bracket removal.
Materials and Methods
The Institutional Review Board evaluated the study and approved (approval number: 0420/DE/2017). The Pannes et al. 9 study was used to compute the sample size, which came out to be 24, with a power (1-β) of 99%, a significance level of 0.05, and a margin of error of 1%.
Specimen Preparation
Two sets of colored and neatly labeled acrylic blocks were made to carry out this investigation. One surface of each set of acrylic blocks had prefabricated zirconia slabs implanted in it. The use of color coding made it easier to distinguish between different groups in later testing processes. Specifically, Group 1, represented by pink-colored blocks (N = 12), accommodated 12 zirconia surfaces using a total-etch system for bonding, while Group 2, represented by purple-colored blocks (N = 12), also housed zirconia surfaces using self-etching for bonding.
Bonding Procedure
Group 1 uses a total-etching technique comprising 3M Unitek Transbond XT adhesive (Monrovia, California) employed for bonding brackets (ceramic) to zirconia surfaces. The bonding process commenced with the application of hydrofluoric acid etchant to the zirconia surface for 30 seconds, rinsing with water, and subsequent drying. A ceramic primer was then meticulously added to the prepared surface and cured using light for 20 seconds. Subsequently, the adhesive (Transbond XT) was added to both the zirconia surface and the base of the bracket; then, each layer was individually light-cured for 20 seconds using a CU 100 ADENTSPLY curing unit.
In Group 2, a self-etching, that is, no-mix system featuring 3M Unitek Scotchbond, the universal adhesive (Monrovia, California, USA) was utilized for fixing ceramic brackets to the zirconia surfaces. The bonding procedure in this group involved the direct application of Scotchbond Universal adhesive to the zirconia surface and the bracket base. Each layer of adhesive was cured for 20 seconds using the same CU 100 ADENTSPLY curing unit.
Subsequently, Transbond XT adhesive was utilized to bond the ceramic bracket to the cured zirconia surface in both groups. The bonding process was completed by light-curing the composite material for an additional 20 seconds using the same light source.
Storage and Testing
After the bonding procedure, all specimens were kept in a saliva substitute for a standardized duration of 24 hours to simulate oral conditions. Using an Instron Universal Testing Machine (No. 3382), the specimens were tested for shear bond strength following the storage period.
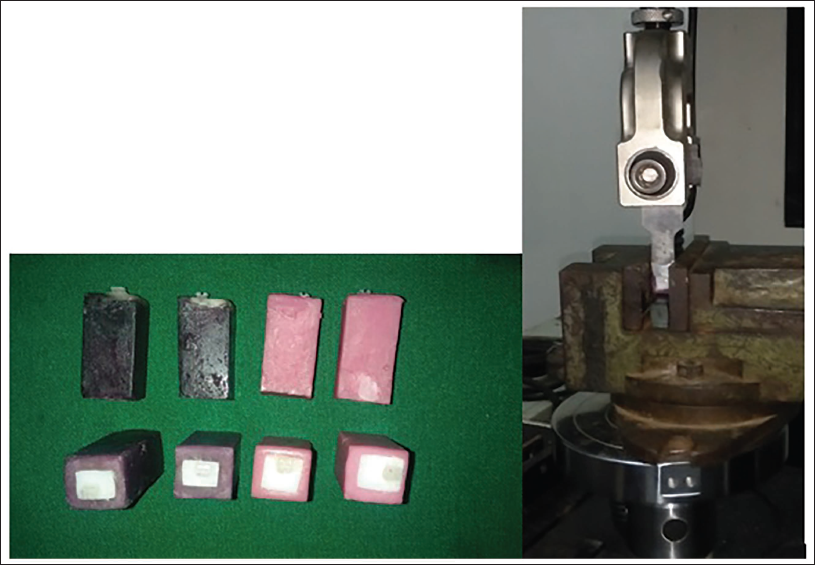
The formula for converting the force needed to debond each bracket from Newtons to Megapascals (MPa) is Bond strength = Breaking load/bracket base area (N/mm2 or MPa). The bond strength was noted and tabulated (Figure 1).
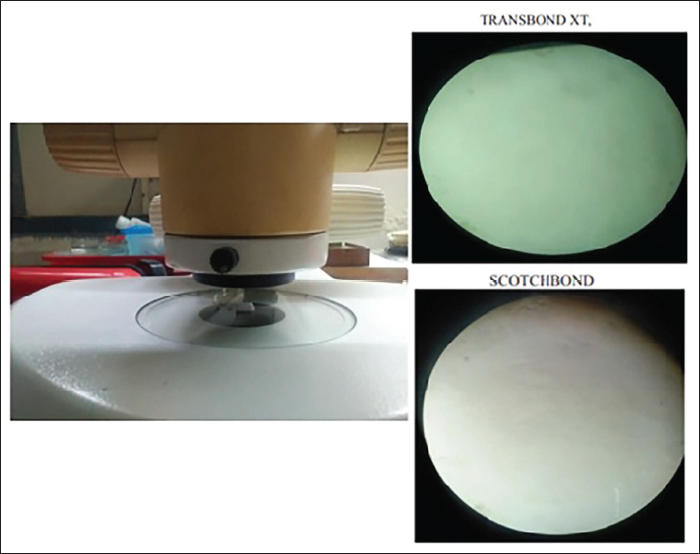
Instron Machine and Groups of Samples for Testing.
Evaluation of Adhesive Residual Score/ARI
Each specimen was carefully viewed under a stereomicroscope with 40× magnification to determine the adhesive residual score. The categorization of the bracket failure mode and the quantity of adhesive residue left on the zirconia surface was made easier by the ARI score. This assessment provided valuable insights into the effectiveness of the bonding systems and the potential impact on zirconia surface integrity.
This standardized methodology ensured precise specimen preparation, consistent bonding procedures, and comprehensive evaluation techniques, facilitating a robust comparative analysis of the bond strength and adhesive residual score between the two orthodontic bonding agents.
Results
Analysis of Shear Bonding Strength
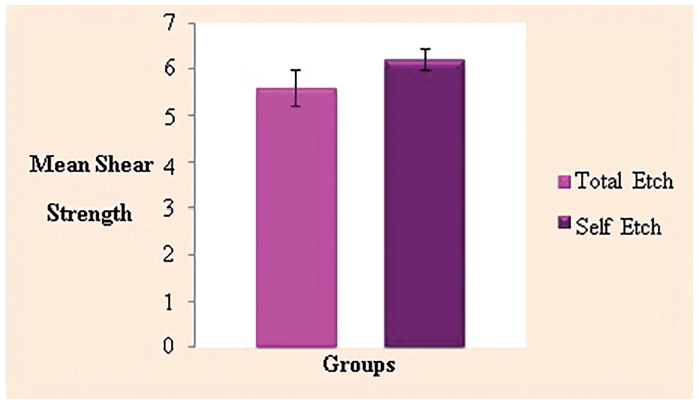
In both the total-etch and self-etch groups, the shear bond strength measurements (in MPa) of each sample were compiled and statistically analyzed. The data were shown to be regularly distributed using the Shapiro–Wilk test, and the findings supported this theory. Consequently, an independent samples t-test was employed to determine the significance of the two groups. Data displayed in Table 1 and Figure 2 indicate that the self-etch group’s mean bond strength (6.21 ± 0.76 MPa) was marginally (10.51%) greater than the whole etch group’s (5.59 ± 1.37 MPa).
Shear Bond Strength (in MPa) between the Two Groups.
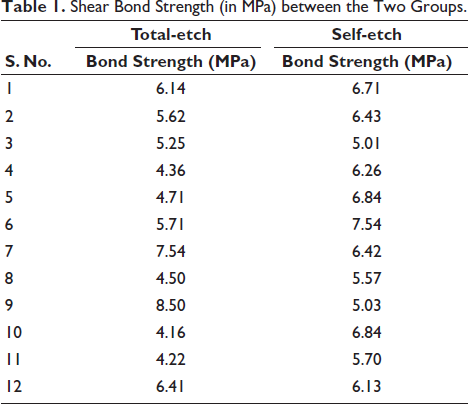
Shear Bond Strength (in MPa) between the Two Groups.
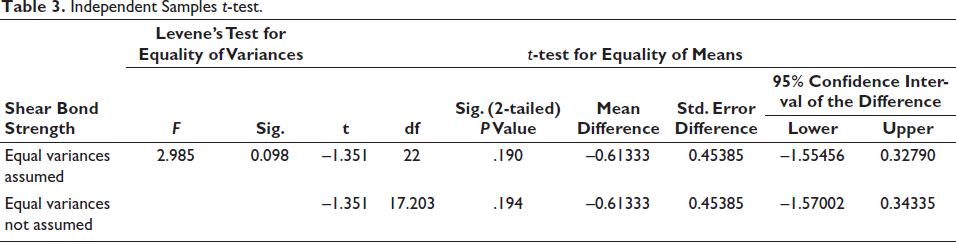
The two groups showed a homogenous variance (p = .098), according to additional analysis using Levene’s test for homogeneity of variances (Table 2). The independent samples t-test yielded a p value of .190 (>.05) and showed a statistically significant difference between the two groups (Table 3).
Independent Sample t-test—Shear Bond Strength between Two Groups.

Independent Samples t-test.
ARI Analysis
Each sample in both groups had its ARI scores tallied using the scoring guidelines set by Årtun and Bergland. 10 To ascertain the type of bond failure, the amount of adhesive residue still present on the tooth surface, and the distribution of scores among the groups, these were evaluated.
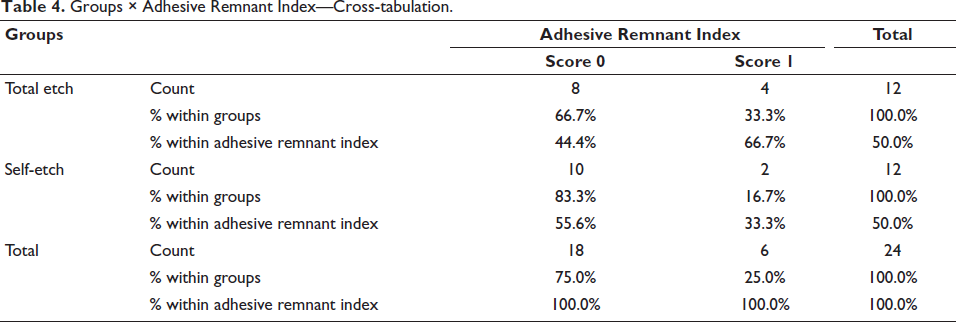
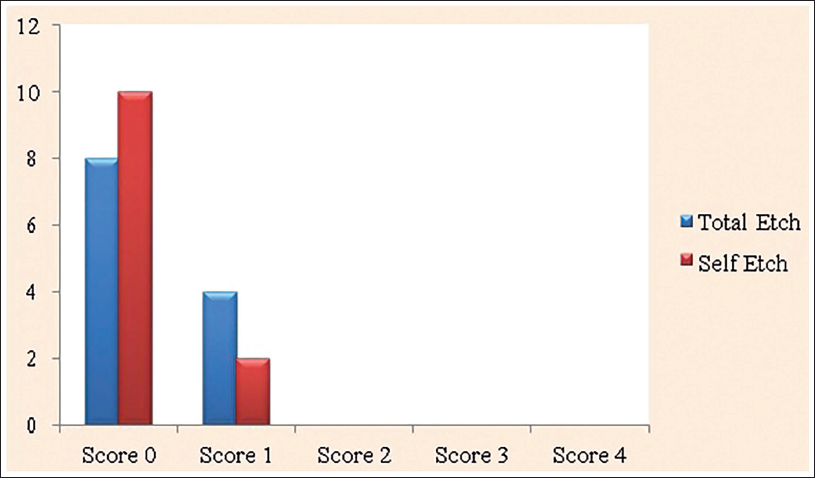
The majority of samples in both groups showed no traces of adhesive remaining on the tooth surface (score 0), showing signs of breakdown of the bond at the tooth surface-resin contact, as indicated by Table 4 and Figure 3. Furthermore, in certain samples, the resin adhesive left on the tooth surface was less than half (score 1), indicating a coherent breakdown within the resin. The surface of the debonded zirconia is seen in a stereo microscope view in Figure 4.
Groups × Adhesive Remnant Index—Cross-tabulation.
Adhesive Remnant Index between Groups.
Stereo Microscope View of the Debonded Zirconia Surface.
Interestingly, no sample in either group obtained a score of 2 or 3, meaning that the link between the adhesive resin and tooth surface was weaker than the binding between the adhesive resin and bracket interfaces.
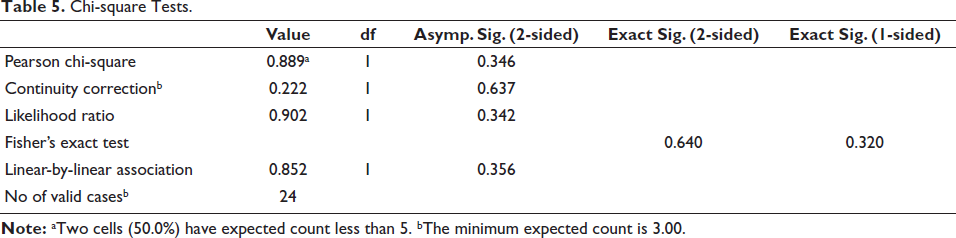
The score distribution of 0 and 1 across the two groups showed an insignificant difference statistically (p = .640), indicating that there was no discernible difference in the manner of bond failure between the total-etch and self-etch groups, according to statistical analysis using Fisher’s exact test (Table 5).
Chi-square Tests.
Discussion
The rise in demand for adult orthodontics and the increasing focus on aesthetic outcomes during orthodontic treatment have led to the widespread adoption of ceramic brackets over metallic ones. 11 Furthermore, good bonding between ceramic brackets and ceramic surfaces is required due to the high number of adult patients having ceramic crowns.12, 13 In this study, we assessed the shear bond strength of two adhesive systems for zirconia surfaces: The self-etch system, Scotchbond Universal, and the total-etch method, Transbond XT–singlebond, when used to bond polycrystalline ceramic brackets.
A common orthodontic adhesive method is the whole etch bonding system with Transbond XT, comprising adhesive resin, bonding agent, hydrofluoric acid, porcelain conditioner, and porcelain primer. 14 Conversely, self-etch systems—such as Scotchbond Universal—have surfaced as an all-in-one adhesive solution that eliminates the need for separate etching and priming procedures, saving time and minimizing mistakes during the process.
Ceramic brackets that are directly bonded to the zirconia surfaces are preferred for orthodontic patients with monolithic zirconia crowns. Improving mechanical retention and bond strength requires surface treatment of the bonding surfaces. While sandblasting, followed by hydrofluoric acid etching, is recommended for various ceramic types, minimal roughening is preferred to avoid microcracks in ceramic surfaces, as noted by Zachrisson and Buyukyilmaz. 15
Both the total-etch and self-etch systems’ mean shear bond strengths from our investigation fell within the range that is considered clinically appropriate. Notably, the self-etch system demonstrated marginally higher bonding strength in comparison to the total-etch system, albeit not statistically significant. These findings align with previous studies reporting comparable shear bond strengths for self-etch adhesives and slightly higher values for total-etch systems.
Our results differ from those reported by Abu Alhaija et al., 16 who achieved higher shear bond strengths using Transbond XT with hydrofluoric acid-etched ceramic crowns. This variation could be attributed to differences in surface preparation techniques, as our study did not involve sandblasting of the ceramic surfaces. Furthermore, compared to our results, Hellak et al. 14 found lower shear bond strengths for total-etch systems on ceramic surfaces, possibly as a result of different bonding agents and types of ceramic materials.
The superior bond strengths observed with self-etch adhesives can be attributed to their hydrophilic nature, which facilitates bonding in a moist environment. 17 Furthermore, phosphate monomers, such as MDP present in Scotchbond universal, form chemical bonds with zirconia surfaces, enhancing adhesive properties.18, 19
The ARI offers information on the method of bond breakdown and ease of clean-up after debonding, even though shear bond strength is still vital. In our investigation, the majority of adhesive failure was observed in the tooth-resin interface for both the total-etch and self-etch systems, with very little adhesive residue remaining on the zirconia surface. These findings suggest that both bonding systems offer clinical advantages in terms of easy clean-up and minimal damage to the tooth or prosthetic surfaces.20, 21
When ceramic brackets were bonded to zirconia surfaces, total-etch and self-etch bonding techniques both showed satisfactory shear bond strengths. However, the self-etch system exhibited slightly higher bond strengths and performed marginally better in terms of ARI scores. These findings highlight the efficacy of self-etch adhesives in orthodontic practice, offering convenience, reliability, and favorable bond characteristics for bonding ceramic brackets to zirconia surfaces. Further research incorporating different surface preparation techniques and adhesive formulations may provide additional insights into optimizing bond strength and clinical outcomes in orthodontic bonding procedures.
Limitation
Data collected in vitro should not be naively translated to the clinical scenario due to the complexity of the oral ecosystem. Studies conducted in vitro can be utilized as a screening technique to forecast clinical outcomes. Variations in relative humidity, temperature, pH, and the frictional and masticatory loads placed on a bracketed tooth in the mouth cannot be replicated in vitro. Conversely, in vitro studies could inspire in vivo investigations.
Conclusion
According to the study’s findings, ceramic brackets and zirconia crowns can be bonded together with sufficient shear bond strength using both the self-etch and total-etch bonding techniques. The self-etch system’s superiority was further corroborated by the ARI scores, which showed a larger percentage of surfaces with little adhesive residue.
The self-etch system is the recommended option for bonding ceramic brackets to zirconia crowns because of its higher shear bond strength and favorable ARI scores, as well as its stated benefits of reducing the number of bonding processes, cutting down on time, and allowing bonding on wet surfaces. The self-etch method provides effective bonding properties, dependability, and convenience—all of which are critical for the successful completion of orthodontic treatment.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board evaluated the study and approved (approval number: 0420/DE/2017).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.