
Abstract
Objective
This study aimed to assess the connection between tongue pressure, Modified Mallampati Score (MMS), BMI, and their role in evaluating obstructive sleep apnea (OSA).
Materials and Methods
A total of 180 participants were categorized into four groups (n = 45) based on the MMS. After securing informed consent, demographic data, including age, gender, body height, and weight (used to calculate BMI) were collected. A tongue pressure measurement system, patented as Innovative Australian Patent no. 2021106623 on 24 November 2021, was utilized.
Results
The one-way analysis of variance test was employed to compare variations in average BMI and tongue pressure across the groups. The post hoc Tukey test revealed significant differences at p ≤ .05. Tongue pressure significantly varied among the distinct MMS categories (p = .001), notably with group 4 displaying significantly lower tongue pressure compared to the other three groups.
Conclusion
The findings suggest that both tongue pressure and MMS are interconnected factors contributing to OSA, while BMI and tongue pressure operate independently in determining OSA.
Introduction
Sleep occupies a significant portion of our lives, and the quality of our sleep profoundly impacts our productivity. Sleep-disordered breathing (SDB) is an umbrella term encompassing a spectrum of chronic conditions, from mild primary snoring to severe obstructive sleep apnea (OSA). 1 OSA is a prevalent sleep disorder with considerable health consequences, including potential risks for hypertension, diabetes, heart disease, and neurological comorbidities. 2 It affects both physical and mental function, and assessing health-related quality of life (HRQOL) among individuals with OSA is a matter of increasing research interest.
Diagnosing OSA remains challenging. To make informed clinical decisions, a systematic approach is essential. Patients reporting loud snoring witnessed apnea episodes, or excessive daytime sleepiness should be considered for OSA evaluation. However, solely relying on typical patient features may miss OSA in older, mildly obese, or healthy-weight individuals who should undergo polysomnography for further assessment. 3
Anatomical and functional abnormalities of the upper airway play a pivotal role in increased airway resistance and the development of OSA.4, 5 The modified Mallampati score (MMS) offers a simple, non-invasive, and cost-effective diagnostic tool for assessing oropharyngeal visualization without requiring specialized equipment. Moreover, the presence of increased fatty tissues, particularly in the tongue and pharyngeal areas, negatively affects upper airway patency due to reduced muscular tone during respiration. 6 Upper airway collapse often occurs at the tongue base, especially in more severely affected patients.7, 8 Kushida and colleagues 9 even developed a predictive model combining oral cavity measurements with body mass index (BMI) and neck circumference to predict the likelihood of sleep apnea.
Despite the critical role of craniofacial soft tissue structures in the pathogenesis of OSA, little attention has been given to their examination and quantification in assessing OSA risk. Furthermore, there is limited literature on human tongue pressure, and only a few publications have explored tongue strength. 10 Thus, this study aims to establish the clinical utility of tongue pressure, the MMS, and BMI in predicting OSA.
Materials and Methods
Participants
The research was conducted at Vidarbha Youth Welfare Society Dental College and Hospital in Amravati, Maharashtra, India. In adults, the anatomy of collapsible lateral pharyngeal walls is well understood, and the risk of developing sleep apnea increases with age, becoming more likely around the age of 30. The estimated prevalence of OSA is 2–5% in the adult population, emphasizing the importance of early identification of individuals at a high risk for OSA.11–13
A total of 180 adult participants, with complete permanent dentitions and an average age of 28 ± 8.2 years, were included in the study. The sample size was determined using GPower 3.1 software, with each group consisting of 45 participants, including 23 males and 22 females.
Exclusion criteria encompassed patients with palate and tongue abnormalities, musculoskeletal disorders, and syndromic conditions. The study protocol was meticulously designed to align with the principles of the Declaration of Helsinki and received approval from the local ethics board at Vidarbha Youth Welfare Society Dental College and Hospital in Amravati, Maharashtra, India.
Study Design
The 180 participants who gave consent were included. Participants were divided into four groups using a MMS. MMS has been proven to be an independent risk factor in predicting the presence and severity of OSA14, 15 (Figure 1).
A System Used to Measure Tongue Pressure Granted by Australian Patent No. 2021106623.
Group I: Tonsils, uvula, and soft palate are fully visible(n = 45).
Group II: Hard and soft palate, upper portion of tonsils, and uvula are visible (n = 45).
Group III: Soft and hard palate and base of the uvula are visible (n = 45).
Group IV: Only the hard palate is visible (n = 45).
Data Collection for Tongue Pressure.

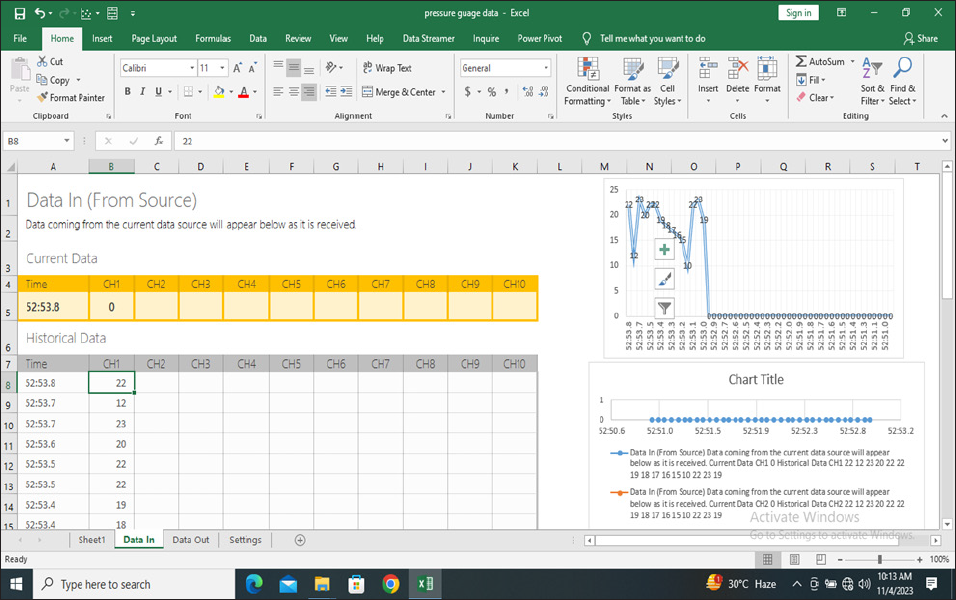
Data Streaming Software.
Criteria used to measure are as follows:
Reliability – The degree to which an instrument measures the same way each time it is used under the same condition with the same subject.
Validity – Validity is the extent to which a test measures what it claims to measure.
Usability – Ease in administration, scoring, interpretation, application, low cost, and proper mechanical make-up.
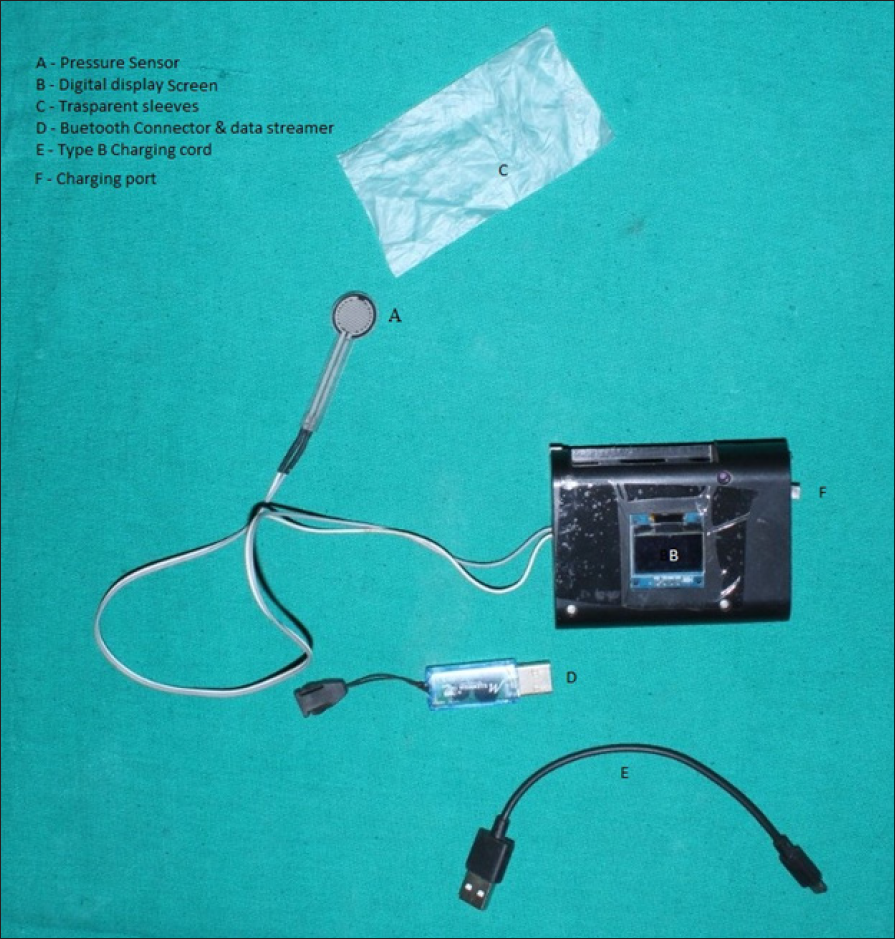
A patented innovative system (Australian Patent no. 2021106623, granted on 24 November 2021) was utilized to measure tongue pressure in kilopascals (kPa). This system comprises a pressure sensor, a digital display screen, an inbuilt Bluetooth connector for cordless and portable functionality, and a data streaming program for data collection and storage (refer to Figure 3). The device is compatible and can be connected via Bluetooth to Windows or Android systems, ensuring practicality.
To gauge the maximum tongue pressure, the patient is instructed to apply pressure on the sensor while it rests on the palate (see Figure 2). This measured value reflects the strength of the genioglossus muscle. Three measurements are taken, with a 1-minute break between each, ensuring reliability and validity. The highest obtained value is considered the reference measurement.
The Protocol
We received informed consent from participants and collected data on age, gender, body height, and body weight (used to calculate the BMI in kg/m). Participants were then introduced to the tongue pressure measurement system, as depicted in Figure 3. A transparent plastic sleeve was used to cover the sensor, with a new sleeve for each participant. Each participant underwent three practice attempts, which were not recorded.
Analysis
Tongue pressure, BMI, and the MMS were compared using a one-way analysis of variance (ANOVA) test. Subsequently, the significance of differences between pairs of group means was assessed through the post hoc Tukey test, with results tabulated in Table 2. A significance level of p < .05 was considered statistically significant in determining differences.
To ensure objectivity and maintain participant anonymity, examiners evaluated the results prospectively without prior knowledge of the participants’ identities. This approach aimed to uphold the integrity of the analysis and maintain confidentiality.
Result
Our study involved 180 individuals categorized into four groups based on their MMS.
Table 1 indicates a significant difference (p ≤ .05) in tongue pressure among various MMS categories. Different superscript letters within a column signify significant differences in tongue pressure based on the MMS. Notably, tongue pressure significantly varied across different MMS categories (p = .001), with Group IV exhibiting significantly lower tongue pressure compared to the other three groups.
Table 2 demonstrates the use of a one-way ANOVA test to compare BMI across different MMS categories, revealing a nonsignificant difference in BMI scores among the MMS categories.
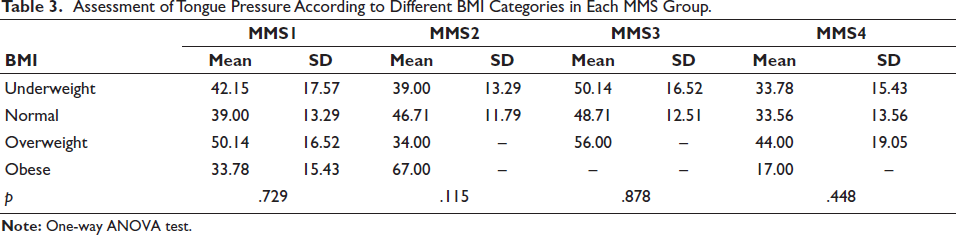
In Table 3, a one-way ANOVA test was used to assess tongue pressure across various BMI categories within each MMS group. The findings indicated no difference in tongue pressure among the four different BMI categories in Group I, Group 2, Group 3, and Group 4, respectively.
Comparison of Tongue Pressure According to MMS.
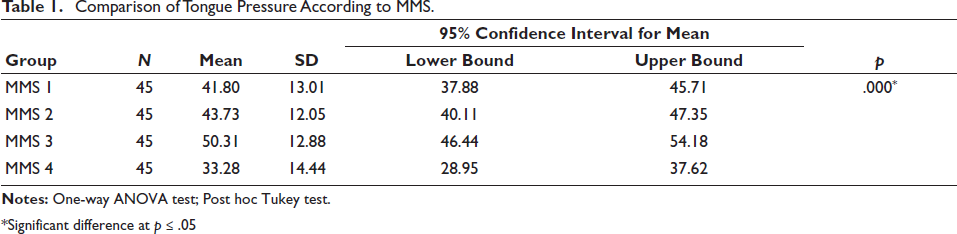
*Significant difference at p ≤ .05
Comparison of BMI According to MMS.
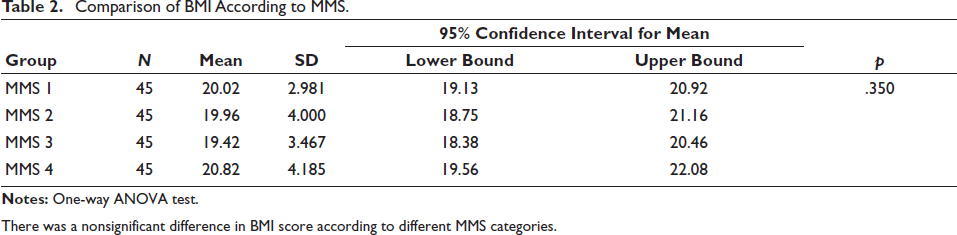
There was a nonsignificant difference in BMI score according to different MMS categories.
Assessment of Tongue Pressure According to Different BMI Categories in Each MMS Group.
Discussion
The role of upper airway anatomy is widely acknowledged in the pathogenesis of airway closure in OSA.18–20 Each patient with sleep apnea may experience airway occlusion at different points along the upper airway.21–23 However, limited attention has been given to the anatomical variations that can influence the onset and management of OSA. While the assessment of OSA typically involves parameters such as the MMS and BMI, there has been a consensus that increased BMI and a high Mallampati score are associated with a higher risk of OSA. Surprisingly, tongue pressure, despite its potential significance, has remained largely overlooked in this context.
To our knowledge, this study represents the first attempt to establish a correlation between tongue pressure, BMI, and the MMS in the screening process for OSA. The importance of tongue strength in the development of OSA cannot be understated, as it is often linked to the malfunction of the dilator muscles of the upper airway. Notably, tongue and lip resting pressures are major factors in dental equilibrium. This study introduces a novel insight into the relationship between tongue pressure, the MMS, BMI, and OSA. The primary objective of this study is to facilitate the early diagnosis of OSA, considering that an estimated 80% of individuals with sleep apnea are currently untreated.
Relationship of Modified Mallampati Score to OSA
The assessment of OSA risk often involves a physical examination of the oral cavity and oropharyngeal crowding. 23 Airway narrowing in various anatomical regions depends on surrounding craniofacial and soft tissue structures. 13 A critical element of this evaluation involves visually estimating the distance from the tongue base to the roof of the mouth, a method that has shown a high sensitivity score (89.7%) in predicting OSA.
The Mallampati grade, first introduced by Seshagiri Mallamapati in 198521, was further modified by Samsoon and Young, 24 and subsequently, Hiremath et al. 25 unveiled a MMS for OSA assessment. Nuckton et al. 26 evaluated 137 patients with suspected OSA and identified it as an independent risk factor for OSA. Dahlqvist et al. 27 highlighted that a MMS of 3 or above was an independent risk factor for an AHI (Apnea-Hypopnea Index) exceeding 15 events per hour.
In our study, we utilized this grading system to categorize the sample into four groups. Through the one-way ANOVA test and post hoc Tukey test, we observed a significant difference (p ≤ .05) denoted by in Table 1. Different superscript letters in a column signify significant distinctions. Our findings indicated a significant variation in tongue pressure among different MMS categories (p = .001), notably showing significantly lower tongue pressure in MMS 4 groups compared to the other three groups.
Relationship of Body Mass Index to OSA
Increased BMI is recognized as a risk factor for developing OSA, a bidirectional relationship often emphasized in mainstream sleep research. Adipose tissues, particularly in the tongue and neck regions, are thought to reduce the normal tone of respiratory muscles during respiration and can alter functional residual capacity, potentially leading to a mechanical restriction of airflow.7, 8 Individuals fitting the “Pickwickian” stereotype, characterized by traits such as being male, obese, sleepy, and snoring in middle age, should not overlook signs of OSA.
Studies, such as Vaara et al., 28 have shown that total body mass and fat are negatively correlated with muscular endurance, while fat-free mass and maximal isometric strength have a positive correlation. Interestingly, a higher prevalence of OSA was found in a population sample of nonobese Asian patients compared to white patients.29, 30 While some studies linking anatomic risk factors with OSA have primarily focused on obesity as defined by BMI or neck circumference, our study revealed non-significant differences when comparing BMI with the MMS in Table 2. Moreover, in Table 3, we found no significant difference in tongue pressure across various BMI categories within each MMS group (underweight, normal, overweight, obese).
Our data suggest that tongue pressure and oropharyngeal soft tissue structures are crucial in assessing individuals exhibiting signs or symptoms of obstructive sleep, independent of obesity. It is imperative to continue investigating how local obesity impacts different soft tissue structures of the oropharynx. Additionally, our study confirmed that the enlargement of lateral pharyngeal walls is an independent risk factor for OSA, even when controlling for BMI and neck circumference. 31 Furthermore, research conducted by Sommer et al. showed a correlation between sex, BMI, and tongue forces.32, 33
Role of Tongue in the Pathogenesis of OSA
The tongue plays a crucial role in upholding the size and shape of the upper airway. Increased fat accumulation at the base of the tongue can alter its shape in the retroglossal region, diminishing the size of the airway behind the tongue and heightening the risk of sleep apnea. Airway shape holds substantial importance in obstructing airway closure during apnea. Moreover, the reduction in tongue muscle tone that occurs during sleep may contribute significantly to OSA.34–37
Tongue Pressure and OSA
Tongue strength plays a crucial role in the development of OSA, as it is often associated with dysfunction of the upper airway dilator muscles and contributes to oral appliance stabilization.
When planning treatment and conducting screenings for OSA, several approaches can be considered, including weight loss, positional therapy, mandibular advancement devices, positive airway pressure therapy (PAP), and surgery. Among these, oral appliances have been found to be more effective and comfortable for treating mild to moderate OSA compared to CPAP. Additionally, noninvasive nerve stimulation is a novel treatment for moderate to severe cases.38, 39 Hence, when managing OSA, the evaluation of tongue pressure should be a primary consideration.
Unfortunately, clinical examinations of patients with OSA often neglect to evaluate the tone of the tongue muscle. In our study, we demonstrated tongue pressure using an innovative appliance that obtained an Australian patent (no. 2021106623).
However, information about tongue mechanics, kinematics, and tongue force remains limited. Some studies suggest a gender-based difference in maximum tongue strength favoring men. Carlos O’Connor-Reina et al. utilized the “Iowa Oral Performance Instrument” (IOPI) to assess maximum elevation strength using a plastic bulb and pneumatic pressure sensor placed just behind the alveolar ridge. Their study found that both tongue and lip peak pressures were lower in OSA patients compared to healthy controls, with tongue peak pressure correlating with the severity of tongue collapse during drug-induced sleep endoscopy. 40
Moreover, a recent meta-analysis by Franciotti et al. 41 demonstrated improvement in patients after engaging in experimental tongue training exercises. However, there was no significant difference in muscle activity of the genioglossus muscle between wakeful healthy individuals and those with OSA. 42 Additionally, in September 2019, Eastwood et al. introduced a new device for Hypoglossal Nerve Stimulation (HGNS) known as the Genio system. 43 In our study, we revealed the association between tongue pressure, BMI, and MMS.
Clinical Applicability and Future Directions
The correlation between tongue pressure and the MMS significantly impacts the prediction of OSA.
Clinical assessment of the oropharyngeal soft tissues in patients with suspected SDB can significantly enhance risk stratification for these individuals and offer valuable insights for determining the most effective treatment options.
In current practice, the utilization of oral appliances like Mandibular Advancement Devices, Tongue Stabilizing Devices, and hypoglossal nerve stimulation stands as more widely accepted treatments for adults with OSA. In such scenarios, measuring tongue pressure can offer valuable diagnostic and treatment information.
Limitations in this Study
More parameters can be added.
Conclusion
Reduced upper airway patency due to anatomical narrowing is a leading cause of respiratory disorders during sleep and correlates with the severity of OSA.
Using the mentioned device for additional screening during routine clinical interviews can help identify patients requiring further diagnostics.
Notably, tongue pressure significantly varies across different MMS categories, with MMS 4 showing notably lower tongue pressure compared to the other three groups.
A strong correlation exists between tongue pressure and the MMS, indicating their interdependence in screening for OSA, while BMI stands as an independent factor in this context.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study protocol was meticulously designed to align with the principles of the Declaration of Helsinki and received approval from the local ethics board at Vidarbha Youth Welfare Society Dental College and Hospital in Amravati, Maharashtra, India.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.