
Abstract
Introduction:
Molar distalization is one of the treatment protocols in cases with mild to moderate arch discrepancy and class II molar relationship associated with a normal mandible. It is achieved by using pendulum appliance and temporary anchorage devices such as miniscrew anchorage system.
Aims and Objectives:
To evaluate and compare the dentoalveolar and skeletal changes between pendulum appliance and miniscrew anchorage system.
Materials and Methods:
The patients were divided into 2 groups of 10 each: group I (using the pendulum appliance) and group II (using miniscrew anchorage system). Lateral cephalogram was taken for each subject and various skeletal such as SNA, SNB, ANB, and PTV-A dentoalveolar (U1-PTV, U6-PTV, U5-FH, and U6-FH) measurements were taken. The data obtained were statistically analyzed using Statistical Package for Social Sciences (SPSS) software. Intragroup analysis between pendulum and implant group was done using Wilcoxon Matched pairs test and the intergroup analysis between pendulum and implant group was done using Mann–Whitney test.
Results:
The results showed that there was nonsignificant difference in both the groups (p > .05) with the less tipping in group II (1.2°) than group I (2.7°) .The molar extrusion was more with the pendulum group (2.1 mm) than the miniscrew anchorage distalization group (1.3 mm).
Conclusion:
The molar distalization using the miniscrew anchorage system showed more bodily movement than the pendulum appliance which showed more tipping movement. Moreover, the pendulum appliance showed significant amount of anchor loss than the miniscrew anchorage system.
Keywords
Introduction
Molar distalization is the most common nonextraction treatment protocol for class II malocclusion. Various treatment modalities are used such as headgear, pendulum appliance, miniscrew anchorage system, and so on. The most conventional is the use of extra oral appliance such as headgear but it requires patient compliance and has poor esthetics. To overcome this disadvantage, molar distalizing appliances requiring minimal patient cooperation are required. 1
Among several intraoral distalizing devices, the pendulum appliance is one of the most commonly used noncompliance appliances. 2 However, the premolar mesial movement and anterior anchorage loss continued to be a problem and requires an additional treatment time for correction during fixed appliance therapy. 3
To overcome the problem, miniscrew anchorage system comes to role in orthodontic mechanics. 4 To overcome this problem, miniscrew anchorage system comes to role in orthodontic mechanics. 7 The distal movement of anterior teeth or posterior teeth or both without anchorage loss is possible with its use in orthodontic mechanics. They have the advantage of having easy placement and removal with minimal anatomic limitations due to their small size. 5 Since there are limited studies in the literature that have been done to evaluate the comparison of dentoalveolar and skeletal changes between pendulum appliance and miniscrew appliance. Hence, the aims and objectives of the study were to evaluate and compare the dentoalveolar and skeletal changes between pendulum appliance and miniscrew anchorage system.
Materials and Methods
The present study was conducted in the Department of Orthodontics and Dentofacial Orthopedics. The subjects were selected from the patients visiting the department for seeking orthodontic treatment. The ethical approval was taken from the institutional research ethical committee (vide no. HDC/ethical/ortho/2017–20/13). Informed consent was taken from each subject before commencing the study. The sample size was calculated with a type 1 error frequency and power of statistical test was set at 80% for a clinical significant difference or the effect size of 0.6. A total of 22 patients were selected; anticipating the dropout rate of 10%, the resulted sample size was 20 subjects.
The subjects were selected on the basis inclusion criteria which was as follows: skeletal class I or mild class II malocclusion (ANB < 7 degrees) with end-to-end or class II molar relationship, absence of protrusive profile or mandibular retrusion, horizontal or average growth pattern with Frankfort mandibular plane angle (FMA) < 25 degrees and radiographs with adequate landmark visualization, and minimal or no rotation of the head. The exclusion criteria includes severe skeletal class II cases (ANB ≤ 7 degrees), severe vertical growth pattern, and severe tooth size/arch length discrepancy.
The patients were divided into 2 groups of 10 each based on the type of appliance used for molar distalization:
Group I—molar distalization was done using the pendulum appliance.
Group II—molar distalization was done using the miniscrew anchorage system.
Methodology
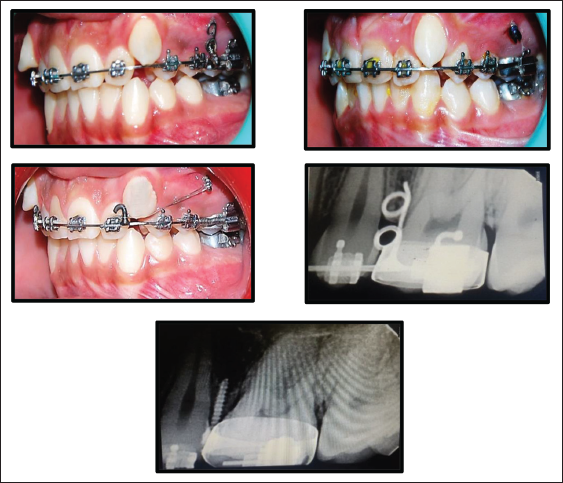
Group I—The Molar Distalization was Done Using the Pendulum Appliance (Figure 1)
After the fabrication of the pendulum appliance, 3 cementation was done at first and second premolars, and first molar. The springs were preactivated extraorally before appliance cementation. After delivery of the appliance, the patients were recalled every month till the desired amount of molar distalization was achieved.
Molar Distalization Done Using Pendulum Appliance.

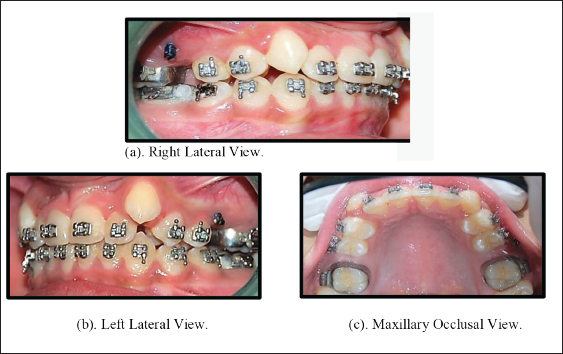
Group II—Molar Distalization was Done Using Miniscrew Anchorage System (Figures 2 and 3)
For all the patients in this group, bonding was done and the wire sequence was followed according to the MBT straight wire mechanics. The miniscrew placement was deferred till the 0.019 inch × 0.025 inch stainless steel rectangular cross-section wire was placed in 0.022 inch × 0.028 inch slot of the bracket.
Miniscrew Anchorage System Placement Methodology.
Molar Distalization Done Using Miniscrew Anchorage System. (a). Right Lateral View. (b). Left Lateral View. (c). Maxillary Occlusal View.
A surgical guide template was made and miniscrew location was selected using an intraoral x-ray. After giving local anesthesia, thickness of soft tissue was measured using periodontal probe at the desired insertion angle of the miniscrew. Absoanchor miniscrew, a titanium screw (Titanium-6Aluminum-4Vanadium ELI Alloy){1.2 mm diameter and 8 mm length}, was inserted between maxillary second premolar and first molar at 45° angulation to the long axis of the proximal tooth. Then open coil spring (Nitinol 0.010 inch diameter) was placed between maxillary second premolar and first molar on 0.019 inch × 0.025 inch stainless steel wire which had J hook soldered distal to canine. Then a ligature wire (0.009 inch) was used for ligation between the J hook and the head of the mini-implant which would reinforce the anchorage. The patients were recalled after every month for the evaluation of the amount of distalization achieved. The open coil spring was reactivated till the desired amount of molar distalization and class I molar relation was achieved.
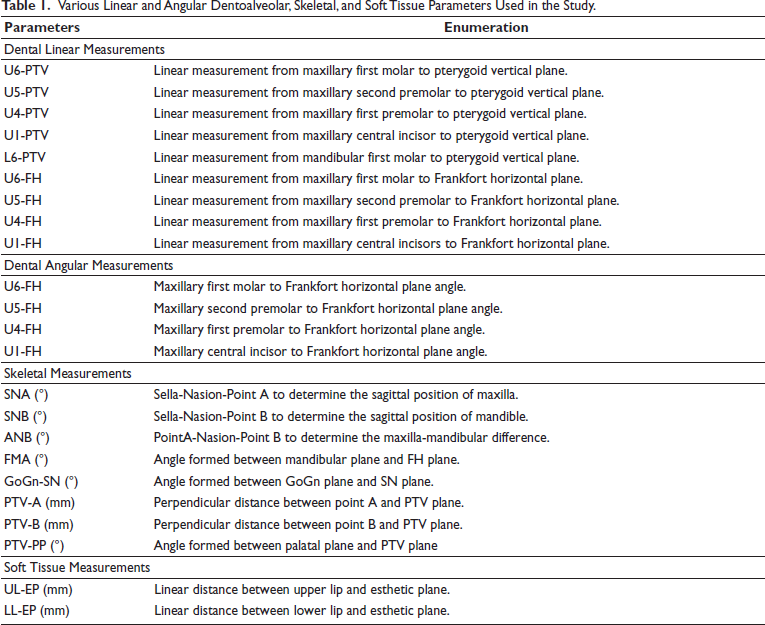
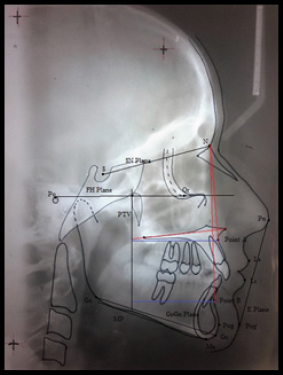
Then manual tracing was done using cellulose acetate paper of thickness 0.003 inch. The lateral cephalogram was taken before the start of orthodontic treatment (T1) and at the completion of the molar distalization (T2) in both the groups. Various linear and angular measurements were assessed as shown in Table 1 and Figures 4 and 5. All the measurements on the lateral cephalogram were made twice by the same examiner to minimize the error of measurements. The intraexaminer reliability was found to be p < .001.
Various Linear and Angular Dentoalveolar, Skeletal, and Soft Tissue Parameters Used in the Study.
Lateral Cephalogram (Showing Skeletal and Soft Tissue Measurements).
Lateral Cephalogram Showing Dental Linear and Angular Measurements.

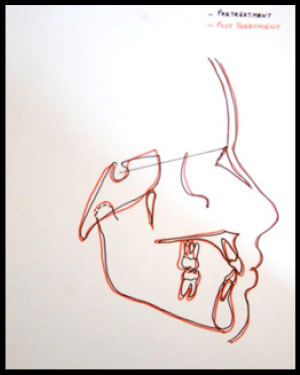
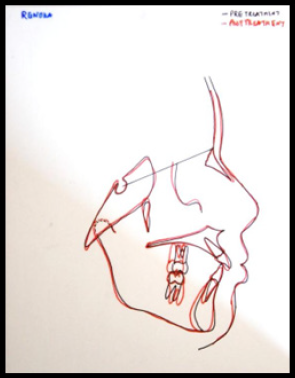
The data obtained was statistically analyzed using SPSS software (version 1.3). The variables were calculated as mean and standard deviation and compared using Wilcoxon Matched pairs test and Mann–Whitney test. The superimpositions of pretreatment and posttreatments lateral cephalogram were done as shown in Figures 6 and 7.
Superimposition of Pendulum Patient.
Superimposition of Implant Patient.
Results
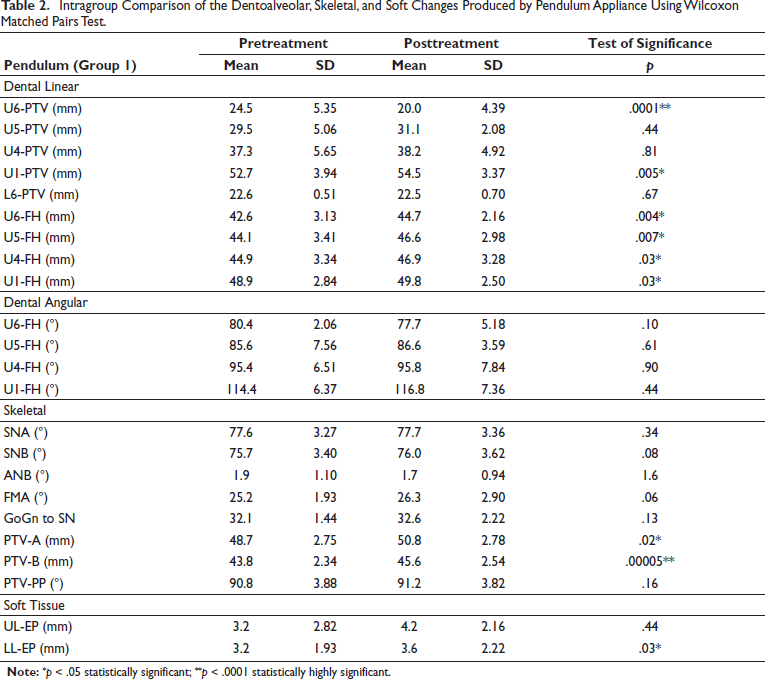
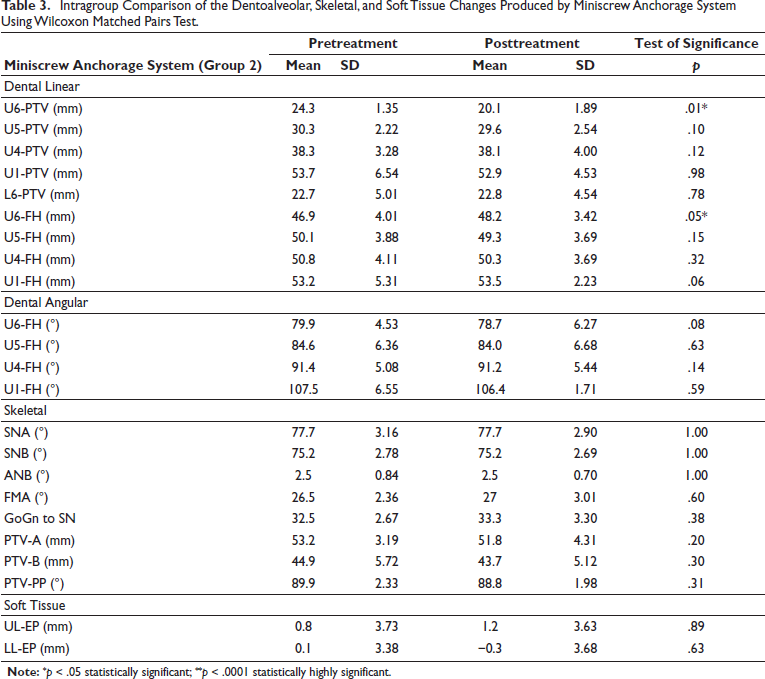
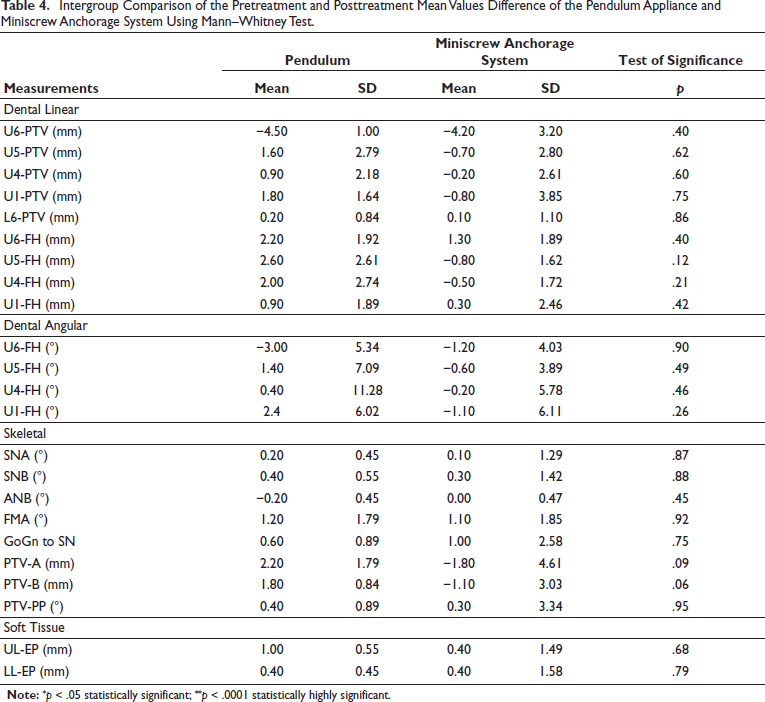
The results showed that on comparison of the pretreatment and posttreatment, difference values of the pendulum appliance, and miniscrew anchorage system using Wilcoxon Matched pairs test, statistically nonsignificant difference (p > .05) was found as shown in Tables 1 and 2, respectively. Further on comparison of mean differences between pendulum appliance and miniscrew anchorage system using Mann–Whitney test, statistically significant difference (p < .05) was found in some parameters of the study as shown in Table 3. The data obtained after analysis showed statistically nonsignificant difference with the less tipping in group II (1.2°) than group I (2.7°) and the molar extrusion was more with the pendulum group (2.1 mm) than the miniscrew anchorage distalization group (1.3 mm).
Intragroup Comparison of the Dentoalveolar, Skeletal, and Soft Changes Produced by Pendulum Appliance Using Wilcoxon Matched Pairs Test.
Intragroup Comparison of the Dentoalveolar, Skeletal, and Soft Tissue Changes Produced by Miniscrew Anchorage System Using Wilcoxon Matched Pairs Test.
Discussion
The results showed that when pretreatment and posttreatment mean values of U6-PTV were compared in group I (pendulum), statistically significant (p < .05) difference of 4.5 mm was found as shown in Tables 1 and 3. This amount of distalization was greater than that achieved in the study conducted on molar distalization (3.4 mm) by Byloff et al. 6 and Ghosh and Nanda. 7 The reason for greater amount of distalization was that the pendulum appliances of conventional types were used in the previous studies in which no additional wire of 19 gauge was soldered on the bands of first and second premolars to reinforce the anchorage.
When pretreatment and postreatment values of the upper first molar to pterygoid vertical (U6-PTV) in group II (mini screw/implant anchorage system) were compared, statistically significant (p < .05) difference of 4.2 mm was found as shown in Tables 2 and 3. The lesser molar tipping might be due to the vector of distalizing force and reactive force which were located near to the center of resistance of molars in the implant group as compared to the pendulum group.
When intergroup comparison of U6-PTV between pendulum appliance and miniscrew anchorage system was done, statistically nonsignificant difference (p > .05) was found as shown in Table 3. This may be due to the fact that both the appliances showed molar distalization, irrespective of their effect produced on the dentoalveolar and skeletal components.
The results of the present study showed that the difference in the pretreatment and posttreatment mean values of second premolar (U5-PTV) and first premolar (U4-PTV) in group I was found to be 1.6 mm and 0.90 mm respectively and on comparison the difference was statistically nonsignificant (p > .05) (Tables 1 and 3). The reason for the minimal movement of first and second premolars in mesial direction in our study was the use of a modified form of pendulum appliance which was fabricated by using 19-gauge wire which was soldered on to bands of first and second premolar which reinforced the anchorage. This was supported by the study done by Koul et al. 3
On comparing the measurements of groups I and II, there was more mesial movement of premolars in group I subjects and distal movement of premolars in group II subjects as shown in Tables 2 and 3. This could be explained on the fact that the implant was ligated to a J hook soldered on 0.019 inch × 0.025 inch stainless steel wire which nullifies the anterior component of force applied by the open coil spring and thus reduces the anchor loss.
The mean value difference of 1.8 mm between pretreatment and posttreatment linear measurements (U1-PTV) was found to be statistically significant (p < .05) as shown in Tables 1 and 3. This suggests that there was protrusion of the central incisor in group I which was in accordance to the study done by Keles et al. 8 This might be due to the use of modified pendulum in which additional wire has been soldered on the first and second premolar bands which reinforced the anchorage in the buccal dentoalveolar segment and resulted in lesser counter effect of distalization on the central incisors.
Moreover, the difference in mean values of linear measurement (U1-PTV) in group II subjects was statistically nonsignificant (p > .05) as shown in Tables 2 and 3. This suggests the retrusion of the upper incisor by 0.8 mm which could be explained on the basis that in group II subjects bone anchored device was used which provided excellent source of anchorage for molar distalization.
Further on comparison of the pretreatment and posttreatment linear measurements (U1-PTV) of groups I and II, the miniscrew anchorage system showed no movement of the central incisor in the maxillary arch. As in miniscrew anchorage has been reinforced, hence the counter effect on the anterior teeth has been reduced compared to the pendulum appliance. This was in accordance to Goyal et al. 9
Moreover, the difference in the pretreatment and posttreatment mean values of U6-FH (angular measurements) in group I was 2.7° and was found to be statistically nonsignificant (p > .05) (Tables 1 and 3). The distal tipping of first molar was lesser might be due to the special anchorage considerations used in this study which was in accordance to the study done by Bussick and McNamara. 10 Further in group II, the angular measurements (U6-FH) was 1.2° and was statistically nonsignificant (p > .05) (Tables 2 and 3). It was due to the proximity of force to the center of resistance of first molar which causes slight tipping of molar distally. It was supported by the study of Yamada et al. 5
Further on intergroup comparison of angular measurements (U6-FH) in group I of pendulum appliance and group II of miniscrew anchorage system, it was found that the distal tipping was less in group II. This might be due to the fact that the buccal force vector applied for distalization is below the center of resistance of molar. When the force vector is below the center of resistance, it will result in distal tipping of crown and the generated moments on the teeth tend to tip the molar distally. This was supported by the study of Bussick and McNamara. 10
Moreover, the difference in the pretreatment and posttreatment mean values of vertical linear measurements (U6-FH) in group I was found out to be statistically significant (p < .05); there was a mean extrusion of 2.1 mm of the mesiobuccal cusp as shown in Tables 1 and 3, this was due to the fact that molar distalization is often accompanied by extrusion of molars. This was as per the study done by Karlsson and Bondemark. 11
Further pretreatment and posttreatment values of vertical linear measurements, U6-FH in group II was found out to be statistically significant (p < .05); there was a mean extrusion of 1.3 mm of the mesiobuccal cusp as shown in Tables 2 and 3. This might be due to the buccal force vector applied for the distalization. This was supported by the study done by Bhide et al. 12
In group I, the vertical linear measurements of first premolar (U4-FH) showed extrusion of 2.0 mm, whereas second premolar (U5-FH) showed extrusion of 2.5 mm and was statistically significant (p < .05) as shown in Tables 1 and 3. This could be due to the activation of the appliance which produces a vertical force component that causes the extrusion of the premolars. This was supported by the study done by Ghosh and Nanda. 7
In group II, the vertical linear measurements U4-FH showed intrusion of 0.50 mm and was statistically nonsignificant (p > .05) as shown in Tables 2 and 3. The U5-FH linear vertical measurements showed intrusion of 0.8 mm and was statistically nonsignificant (p > .05). The vertical component of the force exerted from the implant resulted in intrusion of posterior teeth during distal movement. This fact was supported by Park et al. 13
U4-FH and U5-FH (angular measurements) were statistically nonsignificant (p > .05) in group I with mean mesial tipping of 0.40° and 1.10°, respectively (Tables 1 and 3). The possible reason for this might be due to the fact that every action has equal and opposite reaction. As the molar tipped distally, the reactive forces which are created in the buccal segment would tip the premolars mesially. This was in accordance to the study done by Kircelli et al. 4
The pretreatment and posttreatment mean value of angular measurements in U4-FH and U5-FH was statistically nonsignificant (p > .05), with mean distal tipping of 0.20° and 0.60° respectively in group II (Tables 2 and 3). This mesial tipping of premolars was supported by a study conducted by Bhide et al. 12
On intergroup comparison of posttreatment angular measurements (U1-FH) between group I and group II was statistically significant (p < .05) as shown in Tables 1 and 2. The reason may be attributed to the fact that the proclination of maxillary incisors was more in pendulum group. This was supported by the study done by Bhide et al. 12
Maxillary central incisor (U1-FH) showed statistically significant value (p < .05) with an extrusion of 0.9 mm in group I as shown in Tables 1 and 3. This is due to the proclination of incisors which produces the relative effect on the vertical dimensions of the incisors. This was supported by Fuziy et al. 14 In group II, maxillary central incisor (U1-FH) showed statistically significant value (p < .05) with an extrusion of 0.3 mm as shown in Tables 2 and 4. This may be due to the fact that the tipping of the premolars and incisors is less in miniscrew anchorage system, hence the counter effect on the central incisors is less in group II.
Intergroup Comparison of the Pretreatment and Posttreatment Mean Values Difference of the Pendulum Appliance and Miniscrew Anchorage System Using Mann–Whitney Test.
The analysis of the changes in lower lip to esthetic plane (LL to EP) was found to be statistically significant in group I and was found to be statistically nonsignificant in group II as shown in Table 2. This may be due to the fact that soft tissue changes follow incisor inclination changes, as was reported by Ucem et al. 15
Though the study showed significance of miniscrew anchorage anchorage system over the pendulum appliance but the sample size used is small ;site of anchorage is different in both the groups, pendulum being palatal and miniscrew placed buccally may be considered as a limitation for the present study. Further studies to evaluate the effect of distalization before eruption of second molars with its retention and relapse on the longitudinal basis with large sample size should be done.
The result of the present study showed that the dentoalveolar and skeletal effects were more pronounced in the pendulum appliance group as compared to miniscrew anchorage system.
Conclusion
The molar distalization by the miniscrew anchorage system has more bodily movement than the pendulum group which showed more tipping movement.
The pendulum group showed significant amount of anchor loss than the miniscrew anchorage system used for distalization.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Taken from the Institutional Research Ethical Committee prior to commencing the study (vide no. HDC/ethical/ortho/2017–20/13).
Informed Consent
Informed consent was taken from each subject before commencing the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.