
Abstract
Aim and Objectives
The present study aims at evaluation and comparison of durability and hygiene between 2 different lingual retainer wires bonded between premolar to premolar, that is, maxillary or mandibular arch in the same patient.
Materials and Methods
Eighty retainer wires were placed in 40 patients. They were assigned to 2 groups and subjected to 2 different types of retainer wires (multistrand round and 8-braid flat).
Results
The mean durability of multistrand round retainer wire (235.7 ± 67.28 days) was more than 8-braid flat retainer wire (153.5 ± 43.85 days) irrespective of arches to which they were bonded, which was statistically significant. Scores for plaque index, calculus index, and gingival index were found more with 8-braid flat retainers and in lower arch than multistrand round retainer and in upper arch but these are statistically not significant.
Conclusion
The mean durability of multistrand round retainer wire was more than 8-braid flat retainer wire. The analysis did not find any statistical significant association for deposition of plaque, calculus, and gingival inflammation between different retainer wires and between arches.
Introduction
Stability of the posttreatment tooth position is very challenging for orthodontists because the changes occurring in the tooth position after getting the desired result may finally lead to a return of the teeth to an unwanted place that may not necessarily resemble the original malocclusion of the patients. 1 Many appliances have been used to retain the corrected tooth position. The first fixed appliance was banded, then a removable retainer was advocated, and in 1973 bonded fixed lingual retainer was introduced by Knierim 2 for the mandibular anterior teeth and was established as a part of orthodontic treatment to prevent secondary mandibular anterior crowding. Various studies have documented to compare the survival times and hygiene between 2 or more types of retainer wires bonded between canine to canine, and there is very few literature where premolar-to-premolar lingual-bonded retainer has been used. It was also found that a premolar-to-premolar-bonded lingual retainer prevents the recurrence of deep bites more effectively than a canine-to-canine retainer by preventing re-eruption of 6 mandibular anterior teeth after orthodontic leveling. 3
Materials and Methods
The study was done in the Department of Orthodontics and Dentofacial, Orthopaedics, Institute of Dental Sciences, SOA University, Bhubaneswar. The study period was 9 months, and the patients were taken after completion of active orthodontic treatment from the Department of Orthodontics and Dentofacial Orthopaedics, Institute of Dental Science, Bhubaneswar.
Sample Size
Forty subjects and eighty bonded lingual retainer wires.
Forty, multistrand round-dead soft stainless steel.
Forty, 8-braid flat dead soft stainless steel.
Sample Selection Process
Any fixed orthodontic case after debonding was examined for inclusion and exclusion criteria when indicated for a fixed bonded retainer. If the case satisfied the study’s inclusion criteria, the subject was explained the purpose of the study, and written consent was taken. If the patient agreed, they were assigned to one of the experimental groups on a lottery basis. It was ensured that the allocation of patients in each group was equal in numbers. In one group of patients (Group A), multistrand round-dead soft stainless steel was bonded to the upper arch, and 8-braid flat dead soft stainless steel wire was in the lower arch. In the other group (Group B), multistrand round-dead soft stainless steel was bonded to the lower arch, and 8-braided flat dead soft stainless steel wire was in the upper arch.
The inclusion criteria were as follows:
Finished orthodontic treatment with clinically acceptable occlusion.
Patients treated by premolars extraction, generalized space anterior to premolars, and premolars ectopically present or severely rotated initially.
Individuals between 15 and 30 years of age.
Subjects with healthy periodontium.
Subjects with no radiographic evidence of periodontal bone loss after radiographic examinations.
Methodology
After a thorough examination, patients were selected and oral prophylaxis was done about 48 h before bonding the lingual retainers. Given 2 different types of wires of required length for premolar-to-premolar-bonded lingual retainer were taken for the upper and lower arch for a patient. Before bonding of the fixed lingual retainer, wires were shaped on the working cast using a light wire bending plier to get proper adaption to the lingual/palatal surface of the tooth. The tooth enamel surfaces were cleaned and polished with the help of handpiece (low speed) using pumice powder and rubber cap for 20 to 25 s. After that, it was etched with 37% phosphoric acid (Meta Etchant; Meta Biomed Co Ltd) for 30 s. Subsequently, it was rinsed for 20 s and warm air dried to remove any moisture in the working area. The anterior segment was isolated by cotton rolls and a suction tube to prevent moisture contamination. The adhesive bis-GMA sealant (3M ESPE Adper TM Single Bond 2 Adhesive) was applied on all teeth to be bonded. Each tooth was light-cured with a light-emitting diode (Straight P; Mectron Dental Pvt Ltd) for 5 s. After bonding agent application and its curing, multistrand round-dead soft wire (Direct-Ortho) was placed on the lingual surface of the tooth to be bonded with the help of a retainer positioner 18 in the interproximal contacts to secure the wire in its ideal position. After securing the wire in an ideal position, resin composite (G-aenial Universal flo; GC Dental Products Corp) was applied to the wire to attach the wire with the tooth to be bonded. Each tooth was light-cured for 10 s for proper polymerization of the composite. After polymerization (curing), contouring and polishing were done to remove any irregularities on the surface of the cured composite. When bonding the upper lingual retainer, care was taken to ensure that the lingual retainer was free from the incisal surface of the teeth to reduce the likelihood of fracture. 9 The same procedure discussed above was followed for bonding 8-braid flat dead soft stainless steel (Direct-Ortho) wire.
Outcome Measurements
The patients were examined over 9-month follow-up period. During this period, the patients were checked for the following measures:
1.
Monthly follow-up was done for 9 months for each patient to evaluate and compare the durability of the 2 retainer wires. The data recorded was based on evaluation and comparison from the retainer bonding date to the retainer failure date. Only the first retainer failure was taken into consideration for 1 retainer wire. Retainer failure was either due to a fracture in the retainer wire or composite with/without a partial/total fracture of the retainer from the teeth. The time interval between bonding of retainer and retainer failure was measured in a number of days.
2.
A dental hygiene survey was done on each patient at the end of the study (9 months after bonding of retainers). Using different clinical variables, the patients were checked for oral hygiene status along the retainer wire and gingival margin. Data collected in this survey was for accumulation of plaque and calculus along the retainer wire, accumulation of plaque and calculus beyond the gingival margin (up to the cervical third of the tooth surface), and for gingival plaque and calculus which were not considered. 4
Seven hygiene indicators were used:
Deposition of plaque incisal/occlusal to the wire by wire.
Deposition of plaque gingival to the retainer wire by wire.
Deposition of calculus incisal/occlusal to retainer wire by wire.
Deposition of calculus gingival to retainer wire by wire.
Deposition of plaque beyond gingival margin (up to cervical third).
Deposition of calculus beyond the gingival margin (up to cervical third).
Gingival inflammation.
Hygiene between arches (upper and lower arch).
The scores were given according to the following indices: Plaque Index 5 (PI I), the Calculus component of the Periodontal Disease Index, 6 and Gingival Index 5 (GI).
Statistical Analysis
The data were collected for 80 bonded lingual retainers. As per the protocol, information on demographic profiles like age and gender, failure/survival of retainer, durability of failed retainer, and hygiene index (PI, CI, and GI) scores were recorded. The data were coded and entered into SPSS 16.0 software for statistical analysis.
Results
Durability of Wires
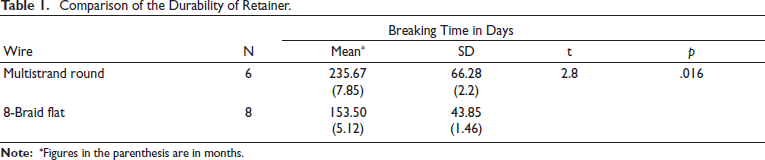
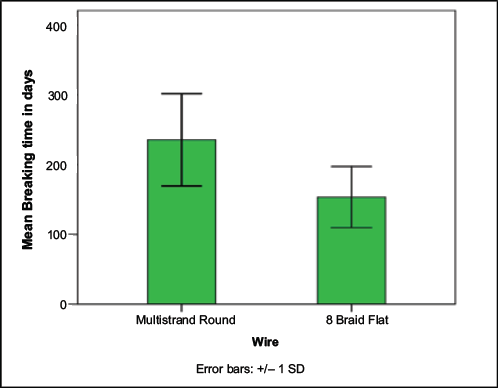
Table 1 and Graph 1 present the comparison of 2 types of retainers. There were 6 failures of the multistrand round wire with a mean duration of 235.7 ± 67.28 days. Similarly, 8 failures of 8-braid flat wire with a mean duration of 153.5 ± 43.85 days were there. This indicated that the mean durability of multistrand round wire was 82.2 days higher than the mean durability of 8-braid flat wire. The difference was statistically significant, with a p value of .016, as the independent sample t test revealed.
Comparison of the Durability of Retainer.
Comparison of Durability of Retainer.
Comparison of Hygiene
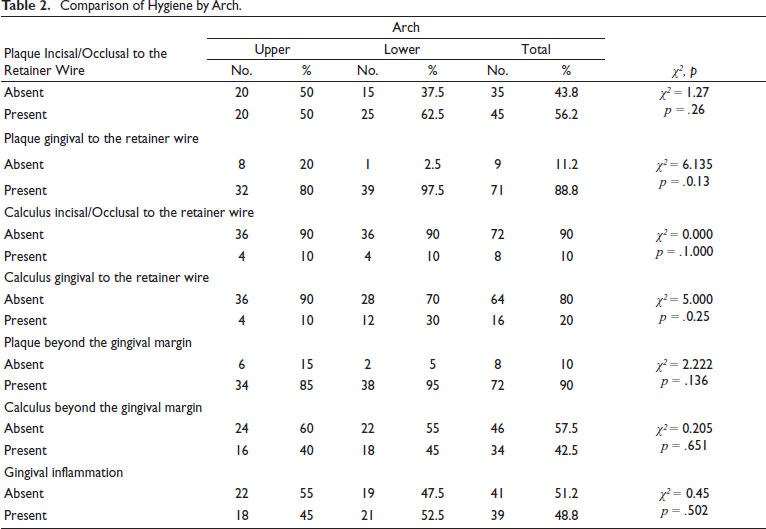
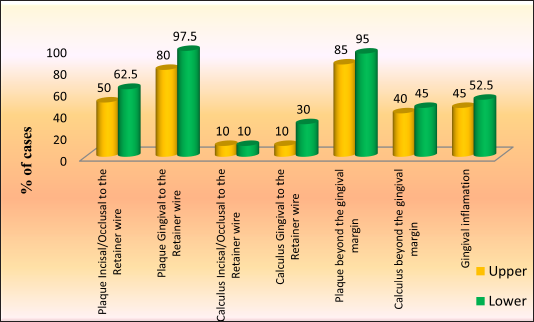
Analysis of different hygiene parameters relating to the wires by upper and lower arches is presented in Table 2 and Graph 2. Plaque deposition occlusal to retainer wire was found among 50% of cases in the upper arch and 62.5% in the lower arch (p = .260). Plaque deposition gingival to retainer wire was present among 80% of cases in the upper arch and 97.5% cases in the lower arch (p = .013). Calculus deposition occlusal to the wire was present in 10% of cases in both the upper and lower arch. Calculus deposition gingival to the wire was present in 10% of cases in the upper arch and 30% in the lower arch with p = .025. Plaque deposition along the gingival margin was found among 85% of cases in the upper arch and 95% in the lower arch (p = .136). Calculus deposition along the gingival margin was present in 40% of cases in the upper arch and 45% in the lower arch (p = .651). Gingival inflammation was found among 45% of cases in the upper arch and 52.57% in the lower arch (p = .502). All 7 hygiene indicators manifested more in the lower arch than in the upper arch.
Comparison of Hygiene by Arch.
Comparison of Hygiene by Arch.
Discussion
The result of the present study is in line with Ardeshna 7 who observed the overall mean survival time of 7.6 months for fiber-reinforced plastic-bonded orthodontic retainers bonded from canine to canine. Rose et al 8 in their 2 years of study of the retainer in the mandibular arch reported the durability of the retainer at 23.5 months for multistrand round wire and 11.5 months for ribbon-reinforced retainer wire. The difference in the result may be explained by the bonding of the retainer only in the mandibular arch and the small sample size of only 10 subjects for each group in the study. In the study conducted by Dahl and Zachrisson, 9 the spiral wire was employed as a fixed retainer in the maxillary arch and showed less survival than the mandibular arch. Salehi et al 10 also found high survival in mandibular arch for polyethylene-woven ribbon retainer. They found the mean durability of 15.34 ± 0.47 and 15.60 ± 0.42 months for flexible spiral wire retainer (0.0175 inch) in the upper and lower arch respectively while for ribbon retainer, it was 13.95 ± 0.55 and 14.26 ± 0.57 months. Both studies are reported with higher durability than the present study. The discrepancy in result may be explained by the shorter duration of the present study and bonding of retainer from premolar to premolars rather than canine to canine. Tuverson 11 suggested that rotational relapse may be due to small contact points at the axial part of bonded teeth, which seems unstable. Surbeck 12 commented that the presence of more crowded and irregular dentitions may not necessarily be the sole indicator of the risk of relapse after treatment.
Studies Comparing the Failure Rate of Retainer Wires
The present study’s finding is in accordance with the result of Bearn 13 who found an overall failure rate of bonded lingual retainer ranging from 10.3% to 47%. The data on the retainer failure rate in the present study is relatively higher than the 11.6% given by Zachrisson. 14 Bolla et al 15 found 21.42% and 22.22% retainer failure in maxillary arch for glass fiber-reinforced and multistranded retainers, respectively. The corresponding value for the mandibular arch is 11.76% and 15.62%, respectively. The high failure rate in the maxillary arch may be due to occlusal interference of maxillary retainer wire with incisal edges of lower anterior teeth. 9 Another possible cause may be the poor brushing habit of the patients. 13 As per the study of Salehi et al, 10 the failure rates, both in the upper and lower arch, were more with ribbon retainer than with multistranded retainer but not significant statistically. For multistrand retainer, it was 36.5% and 37.8% in maxillary and mandibular arch, respectively. The corresponding value for ribbon retainer was 50% and 42.6%. The higher failure rate of the ribbon retainer in the study may be due to less flexibility of the ribbon retainer than the multistranded retainer. Taner and Aksu 16 in a prospective study of 6 months found 37.9% of retainer failure from canine to canine in mandibular arch for 0.016×0.022 inch 8-braid flat wire. The overall failure rate found was 29%. Dahl and Zachrisson 9 reported an overall survival rate of 29% for 3 strand and 5-strand spiral wires. The lack of adaptation of retainer wire to the lingual surface of the teeth is also one of the reasons for the high failure rate because it helps in the close placement of wire and tooth surface with the help of composite. 9 It may be due to a lack of stabilization 17 of retainer wire during resin polymerization. Movement of the retainer wire during its initial setting causes bond failure and loosening of the retainer within a few days or months after retainer bonding.14, 17, 18 The number and experience of operators may also cause an increased retainer failure rate. Successful clinical outcomes are often reported by experienced operators.4, 9, 19 Sometimes it is also associated with dental fluorosis because it interferes with the etching of the enamel surface, causing poor adhesion of composite and enamel.
Studies Comparing Survival Rates and Types of Retainer Wire
Result of a study done by Farronato et al 20 also supports the present study in which they found a survival rate of 81.3% for posttreatment canine to canine lingual retainers with fiber-reinforced composite resin.
Survival rates are considerably higher than those reported in many other studies on lingual retainers. Taner and Aksu 16 clinically reported survival rate for mandibular lingual retainer. It was found to be 62% with 0.016 × 0.022 inch 8-braided stainless steel wire. A total of 63% survival rate was found for flexible, braided, bonded stainless steel lingual retainers by Lie Sam Foek 21 over 41.7 months. The survival rate decreased in this study, with the highest number of failures being observed within the first 6 months after placement. One explanation could be insufficient bond strength between composite and enamel. Factors such as moisture contamination or wire movement during the composite’s initial setting could impair ideal adhesion, resulting in a fracture in the first few weeks after bonding. The survival rate for 8-braid flat wire in the present study is relatively higher than in the previous study. It was found to be 80%, irrespective of the arches to which they were bonded.
Studies Comparing Hygiene Status
The results of the current research are in line with the study of Artun et al4, 22 in which they concluded that the accumulation of plaque and calculus is associated less with retainers made up of spiral wire than plane wire. Evaluation of plaque and calculus index related to retainer wire (incisal/gingival) demonstrates that deposition of plaque and calculus is more associated with 8-braid flat wire than multistrand wire, and this can be explained by the larger surface area of the 8-braid flat wire and to it being more significant contact with the dental surface. 9
Dahl and Zachrisson 9 observed that the maxillary retainers were generally free from plaque and calculus, while mandibular retainers often showing an accumulation of calculus in the interdental area. The observation of the present study also supports this observation, where deposition of plaque and calculus is more associated with lower retainers. The score difference between upper and lower may be explained by the tendency to develop plaque and calculus in the lower arch is more due to the presence of a submandibular gland. The gingival index was higher for the 8-braid flat wire than the multistrand spiral wire, this being in agreement with the result found for plaque index as the greater the quantity of plaque deposition, the more significant the gingival inflammation. 23
The observation of the present study also conforms the study of Marlice Azoia Lukiantchuki et al, 24 who compared periodontal parameters after bonding 2 types of retainers in the study. The retainers were multistand wire retainers and modified retainers. It was found that there is a more significant plaque accumulation on the lingual and total surface associated with a modified retainer. They also found greater calculus and gingival index scores with the modified retainer on the lingual surface. That implied that a more significant accumulation of calculus and a greater degree of gingival inflammation was found in association with a modified retainer than a multistrand round wire retainer, which is similar to the result in the present study.
Conclusion
The following conclusion can be drawn from the present study:
The mean durability of a multistrand round retainer is more than 8-braid flat retainer wire, irrespective of the arches to which they are bonded, which is statistically significant. We observed relatively less mean durability, which may be associated with short-term study and extension of retainer wire till premolars. The mean durability of retainer wires may be increased with an increase in the study period.
The failure rate of multistrand round retainer (15%) is less than 8-braid flat retainer (20%) over the period of the study but not statistically significant, and there is no difference in failure rate between upper and lower arch for both the retainers.
Deposition of plaque, calculus, and gingival inflammation is more associated with 8-braid flat retainer wire in the lower arch than multistrand round retainer wire in the upper arch, but it is statistically insignificant. Deposition of plaque and calculus are found more gingival to the retainer wire than occlusal to the retainer wire, and among wires, deposition of calculus incisal/occlusal to the retainer wire was more associated with multistrand round wire than 8-braid flat wire, but these are statistically not significant.
Ethical Approval
This study was approved by the Institutional Ethical Committee (approval no-IES/193).
Informed Consent
All participants provided written informed consent before enrolment in the study.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.