
Abstract
Objectives
The aim of this study was to evaluate and compare the long-term skeletal stability of mandibular advancement and mandibular setback achieved with bilateral sagittal split ramus osteotomy (BSSRO) procedure in adult patients with a minimum follow-up of at least 1 year.
Methods
A literature search was systematically performed according to PRISMA guidelines from four databases without limitation till 15 June 2021. Available literature was assessed for long-term skeletal stability as horizontal/vertical changes at cephalometric point B following conventional mandibular surgery (BSSRO) with rigid internal fixation. The quality of selected articles was assessed using Newcastle–Ottawa scale and the meta-analysis was carried out with Q statistic method, I-squared statistics, and fixed-effect model to estimate the pooled mean and Begg–Mazumdar bias indicator.
Results
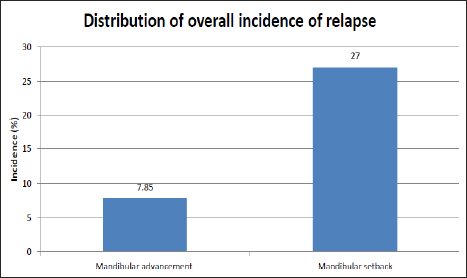
A total of five studies (three pertaining to mandibular advancement and two setback groups) were included for comparative evaluation of relapse. The mean horizontal relapse was 7.85% pertaining to mandibular advancement (4.2–7.06 mm) as compared to 27% pertaining to mandibular setback (7.18–10.26 mm). The meta-analysis of four included studies (two in each group) revealed significant differences in long-term skeletal stability of mandibular advancement and setback (pooled proportion = 20.10; 95% confidence interval = 2.48–39.57).
Conclusion
Mandibular setback can be expected to relapse by 21.7–32.3% (mean 27%) as compared to mandibular advancement accounting for a relapse of 2.1–15.4% (mean 7.85%) in adult patients. Hence, mandibular advancement is a relatively stable procedure in the long term.
Introduction
The vast advancement in orthognathic surgical techniques has created various opportunities for the management of dentofacial deformities, thereby providing an orthodontist with multiple options rather than a compromised treatment. 1 Bilateral sagittal split ramus osteotomy (BSSRO), as described by Trauner and Obwegeser, 2 is a widely used standard procedure to address mandibular deformities. However, stability following such procedures has been a major concern since the treatment outcome is directly related to post-surgical stability 3 that can be further categorized into short and long-term stability.4, 5 Function adapts to form up to one-year post-surgery; hence, short-term stability is directly attributable to surgery-related factors (errors in surgical planning/model surgery, intraoperative surgical errors, or wound healing problems). However, form is affected by function beyond one-year post-surgery (long-term stability); thus, treatment changes during this period reflect adaptive bone remodeling and/or resumption of growth and adaptive changes in the dentition. 4 Factors responsible for skeletal relapse primarily include the magnitude of surgical movement (advancement or setback), osteotomy slippage due to muscle pull, condylar displacement from glenoid fossa, lack of control of proximal segment during surgery, and inappropriate fixation method. Unfavorable postsurgical growth, pre-existing temporomandibular joint (TMJ) derangement, age at the time of surgery, and condylar osteolysis also contribute to relapse.6–8
Mandibular advancement has been regarded as a highly stable technique as compared to mandibular setback, which has been considered problematic. 4 During the last few decades, various studies have evaluated short-term changes; however, in recent years, the long-term skeletal and dental stability of these surgical techniques has been questioned. As a result, recent research has evaluated the long-term dental stability of various orthognathic surgical techniques. 9 A recent overview of systematic reviews 10 reported both mandibular advancement and setback as “stable” procedures but did not provide comparative data for the stability of both procedures. Therefore, this systematic review attempted to assess and compare the long-term skeletal stability of mandibular advancement and mandibular setback with BSSRO procedure in adult patients with follow-up of at least one year.
Materials and Methods
Protocol and Registration
A thorough protocol was designed as per Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2021 guidelines 11 (Supplementary Table 1). The specification and registration of the search protocol was done with the International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42021261466. The following focused question was formulated according to the Patient, Intervention, Comparison, and Outcome (PICO) format: “What is the long-term skeletal stability of Bilateral sagittal split ramus osteotomy procedure for mandibular advancement and setback? Is there any difference in long-term skeletal stability of mandibular advancement and mandibular setback using bilateral sagittal split ramus osteotomy procedure?”
Search Strategy
In addition to a manual search from institutional library’s database, a comprehensive and systematic electronic search was carried out by two investigators from database inception till 15 June 2021 from the following search engines—Science Direct, Google Scholar, MEDLINE-PubMed, and Cochrane Central Register of Controlled Trials (CENTRAL). Numerous combinations of terms from Medical Subject Headings (MeSH) and free text were used as follows:
“Bilateral sagittal split ramus osteotomy” OR “BSSRO” “Mandible” OR “Mandibular” “Advancement” “Setback” “Skeletal stability” OR “Stability” OR “Relapse” OR “Relapse rate” “Fixation” OR “Rigid fixation” OR “Semi-rigid fixation” (1) AND (2) AND (3) AND (5) AND (6) (1) AND (2) AND (4) AND (5) AND (6) (1) AND (2) AND (3) AND (4) AND (5) AND (6)
Eligibility Criteria
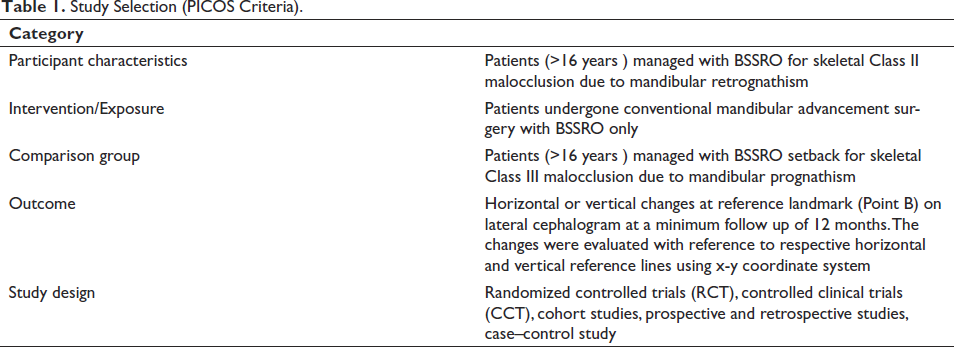
Table 1 illustrates the PICOS format used for forming inclusion and exclusion criteria.
Inclusion criteria:
Full-text articles published/available in English language till 15 June 2021; Adults (≥16 years) treated with conventional isolated BSSRO advancement or setback procedure; Mandibular surgery ≥ 4 mm; Rigid or semi-rigid fixation; Follow up of ≥ 12 months after surgery; Studies reporting skeletal changes at point B; Controlled clinical trials (CCTs), randomized controlled trials (RCTs), cohort studies, prospective and retrospective studies, case–control study.
Exclusion criteria:
Syndromic patients; Bimaxillary surgical procedure or BSSRO along with any adjunctive surgical procedure; Surgery first approach for management of mandibular deformity; Abstracts, expert opinion, case reports, reviews, case series, letter to editor, animal or in vitro studies.
Study Selection (PICOS Criteria).
Selection of Studies
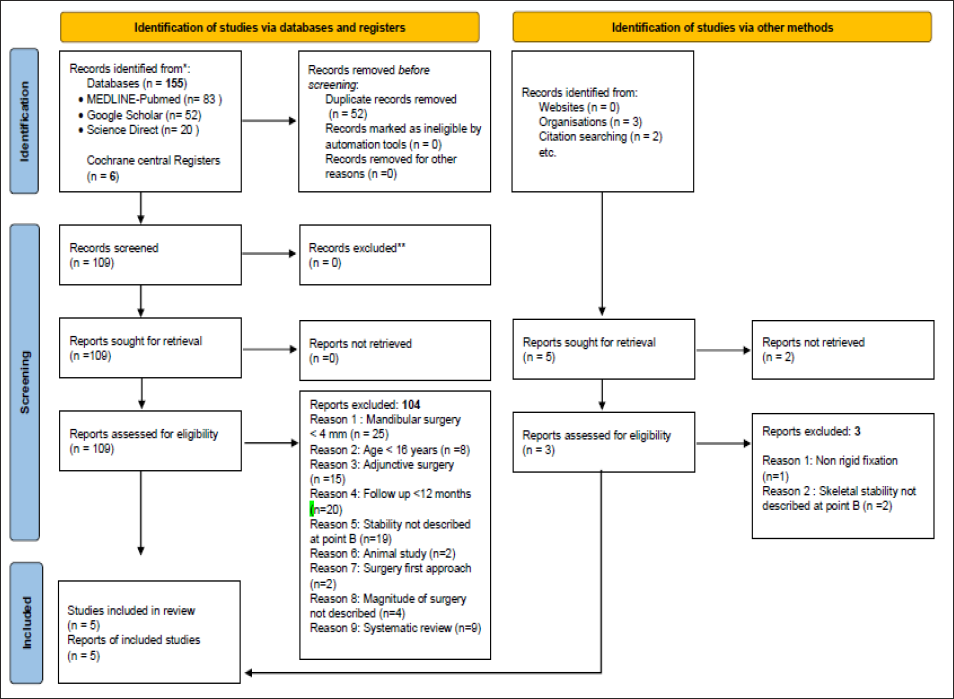
The stage-wise procedure for the selection of articles as per PRISMA guidelines 11 is elaborated in Figure 1 and Supplementary Table 2. Publications not meeting the inclusion criteria were eliminated using a positive exclusion method, while a full report was obtained and further screened for the titles qualifying the inclusion criteria. The studies excluded after full-text evaluation have been listed as Supplementary Tables 3 and 4 with references attached as Supplementary Tables 5 and 6. Two authors individually compiled a list of retrieved evidences in a stepwise manner, which was further verified by senior orthodontists to ensure strict adherence with the study protocol as per guidelines. A total of five articles12–16 met the selection criteria and were therefore included in the present study.
Data Extraction and Quality Assessment
The studies that were included were split into two groups, that is, BSSRO advancement and BSSRO setback. The data extraction from the selected studies was carried out using the following parameters: study and patients characteristics, number of patients, minimum age, fixation method, the minimum amount of BSSRO (advancement or setback), follow-up period, and relapse rate at follow up. The assessment of relapse at point B was measured using an x–y coordinate system in a lateral cephalogram in which the horizontal reference x-axis and vertical reference y-axis served as the basis for evaluation of vertical and horizontal relapse, respectively. Newcastle–Ottawa scale 17 was utilized for the assessment of risk of bias in the selected studies stating their methodological quality (Supplementary Table 7).
Heterogeneity Assessment
Cochran Q (chi-squared) test and I-squared statistics were used to assess and quantify statistical heterogeneity which was graded as low (I2 < 25%), moderate (I2 = 25–50%), or high (I2 > 75%). In case of nonsignificant heterogeneity (p > .10 and I2 < 50%), a fixed effect model was used to estimate the pooled means with corresponding 95% confidence intervals (95% CIs); otherwise, a random effect model was employed. Using the Begg–Mazumdar’s rank correlation test, publication bias was statistically evaluated, which was further verified by the presence of statistically significant Kendall tau value (p < .05).
Results
Search Results
The search strategy identified a total of 164 articles, that is, 155 articles through the electronic database, five articles through the Cochrane central register, and three articles manually from the database available in the institutional library, thereby comprising 91 studies in BSSRO advancement group and 73 studies in BSSRO setback group. After elimination of duplicates, a total of 112 articles including institutional searched articles were assessed for eligibility. These comprised 63 articles in the BSSRO advancement group and 49 in the BSSRO setback group (Supplementary Table 2).
Included Studies
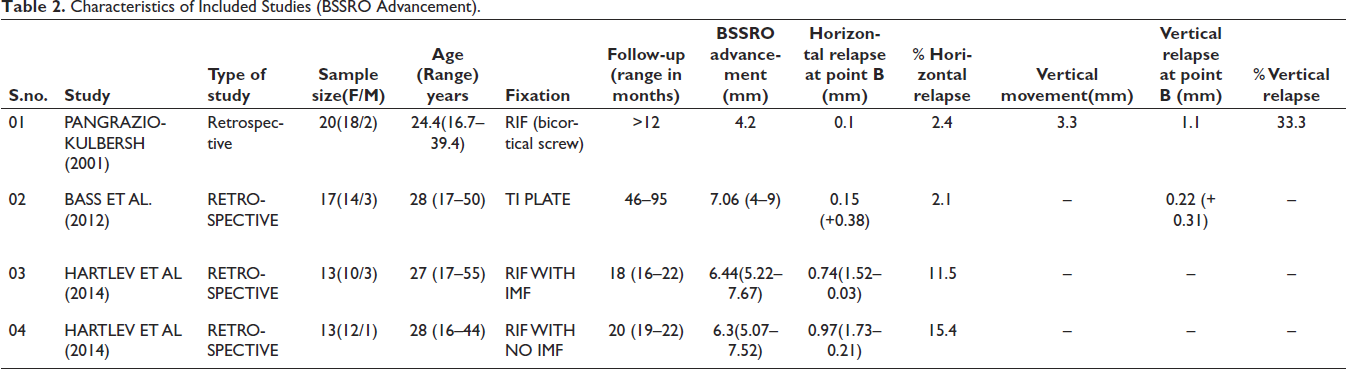
Five articles were eligible for the final assessment among which three studies were included in the mandibular advancement group12–14 and two studies in the setback group.15, 16 A total of 107 patients were involved in the studies, 63 in the mandibular advancement group and 44 in the mandibular setback group. Detailed characteristics of included studies are outlined in Tables 2 and 3, respectively. Since none of the included study contributed data to both the groups, hence only the pertinent data from each of them were extracted. A study by Hartlev et al. 14 yielded two data pertaining to horizontal relapse rate owing to two different groups (RIF with intermaxillary fixation and RIF without intermaxillary fixation) included in the study.
Characteristics of Included Studies (BSSRO Advancement).
Characteristics of Included Studies (BSSRO Setback).

Excluded Studies
The studies excluded after full-text evaluation have been listed as supplementary Tables 3 and 4 with detailed references attached as supplementary Tables 5 and 6, respectively. Twenty-five studies were excluded from the review because the magnitude of surgery was <4 mm [A1–A15, B31–B40]; 15 studies were excluded due to adjunctive surgical procedure other than BSSRO [A26–A31, B10–B18], skeletal stability was not mentioned in 21 studies [A43–A54, B19–B27], 20 studies failed to follow up for at least 12 months [A32–A42, B19–B27], the minimum age was <16 years in eight studies [A16–A23], four studies did not define minimum or total magnitude of surgery [A55, B28–B30], two studies used surgery first approach [B41–B42], one study did not incorporate RIF [B43], and two were animal studies [A24–A25]. The full text of two articles [B48–B49] could not be retrieved and hence excluded. Out of the nine systematic reviews, seven were excluded, as all the reviewed studies were already excluded during the initial search strategy [A56, A57, A59, A60, B44–B46]; one reviewed 24 studies out of which one was already included and rest excluded [A58]; one reviewed 14 studies out of which one was already included and rest excluded [B47]. Four studies [A5, A15, A52, A55] compared the stability of BSSRO mandibular advancement with the setback; however, they did not meet the inclusion/exclusion criteria and were hence excluded.
Assessment of Methodological Quality
All the included studies were retrospective in nature and Newcastle–Ottawa scale was used for their methodological quality grading comprising of three perspectives, that is, selection of study group, groups comparability, and determination of the desired outcome. The star (*) system assigned a score of 6 to each included study signifying moderate methodological quality (Supplementary Table 8).
Results of Studies Subjected to Meta-analysis
The incidence of relapse was used in the meta-analysis as an outcome variable via StatsDirect, a statistical Software version 2.8.0 (
Distribution of Overall Incidence of Relapse.

Distribution of Overall Incidence of Relapse.
Meta-analysis of Incidence of Relapse (Mandibular Advancement vs. Mandibular Setback).
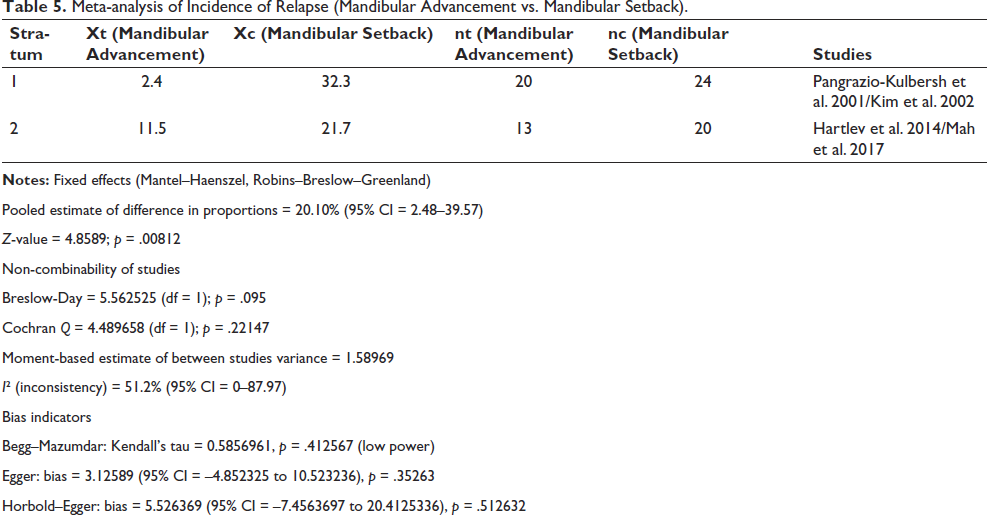
Pooled estimate of difference in proportions = 20.10% (95% CI = 2.48–39.57)
Z-value = 4.8589; p = .00812
Non-combinability of studies
Breslow-Day = 5.562525 (df = 1); p = .095
Cochran Q = 4.489658 (df = 1); p = .22147
Moment-based estimate of between studies variance = 1.58969
I² (inconsistency) = 51.2% (95% CI = 0–87.97)
Bias indicators
Begg–Mazumdar: Kendall’s tau = 0.5856961, p = .412567 (low power)
Egger: bias = 3.12589 (95% CI = –4.852325 to 10.523236), p = .35263
Horbold–Egger: bias = 5.526369 (95% CI = –7.4563697 to 20.4125336), p = .512632
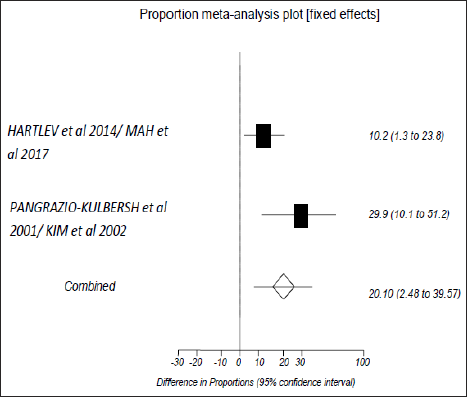
Study-specific Difference in the Incidence of Relapse (Mandibular Advancement vs. Mandibular Setback).

Forest Plot Showing the Difference in Proportions Along With 95% Confidence Interval (CI) Found in the Studies for Incidence of Relapse Included in the Meta-analysis.
Results of Studies not Subjected to Meta-analysis
One study was not suitable for meta-analysis; hence, the results of postoperative stability are discussed in a narrative form. Baas et al. 13 compared the long-term stability of BSSRO mandibular advancement with distraction osteogenesis (DO) procedure; hence, the data pertaining to only BSSRO were extracted. The authors reported a horizontal relapse of 2.1% following a mandibular advancement of 7.06 mm (4–9 mm) in 17 patients with follow-up periods ranging from 46 to 95 months. The vertical relapse reported was 0.22 (+0.31) mm. Among 17 patients, steep mandibular plane angle was present in four cases, while others had average to low mandibular plane angle, though no difference in relapse was reported between these two groups.
Discussion
BSSRO along with rigid fixation is a widely used standard procedure for the correction of mandibular deformity. 18 However, the success is determined by its long-term stable results. 4 Numerous factors contribute to skeletal relapse, which include the expertise of the ortho-surgical team, the age of the patient, preoperative mandibular plane angle, craniofacial growth pattern, the magnitude of surgical movement, muscle tension, the seating of condyles in the glenoid fossa, condylar resorption, pre-existing TMJ pathology, and fixation method.19, 20 Most of the studies have evaluated the relapse of either BSSRO mandibular advancement or setback, but only limited studies have compared the relapse potential of both procedures. Therefore, this systematic review was carried out to evaluate and compare the long-term stability of BSSRO mandibular advancement with BSSRO mandibular setback procedure in adult patients with a follow-up of at least one year.
The conventional surgical approach is usually carried out once the skeletal maturation of an individual has been attained so as to minimize the long-term relapse potential contributed by the resumption of growth, especially in patients with mandibular prognathism.
20
Approximately 98% of mandibular growth is ceased by 15 years in females and usually at the age of 17–18 years in males.
21
The earliest recommended age for orthognathic surgery has been 16.5 years in males.
22
However, late mandibular growth is least likely to be expected following adolescent growth spurt in patients with mandibular hypoplasia, so mandibular advancement is often carried out once the adolescent growth spurt is over.
23
The highest growth rate of the mandible occurs at 13
The assessment of relapse at point B was measured using an x–y coordinate system in a lateral cephalogram in which the horizontal reference x-axis and vertical reference y-axis served as the basis for evaluation of vertical and horizontal relapse, respectively. These x and y axes varied in included studies. Mah et al. 16 used Frankfurt horizontal (FH) plane as x-axis and a plane perpendicular to FH plane at Sella was taken as y-axis. Baas et al. 13 used Sella-Nasion plane as x-axis and plane constructed perpendicular to x-axis at Sella as y-axis, while Pangrazio-kulbersh et al. 12 and Hartlev et al. 14 used constructed x-axis (horizontal line through Sella rotated down anteriorly by 6° and 7°, respectively) and constructed y-axis (perpendicular to x-axis at Sella).
As compared to problematic mandibular setback, mandibular advancement has been considered as a highly stable procedure. 4 However, a recent study reported both mandibular advancement and setback as “highly stable” procedures with relapse up to 24% in the context of BSSRO with RIF, whether with screws and/or plates. 10 In the present review, the mean horizontal relapse was 7.85% pertaining to mandibular advancement (2.1% with Ti plate, 13 2.4% with bicortical screw, 12 11.5% with RIF along with IMF, 14 15.4% with RIF without IMF 14 ) and 27% pertaining to mandibular setback (21.7% with semi RIF, 16 32.3% with bicortical screw 15 ). Among the five included studies, only two studies12, 16 reported vertical relapse at point B. Pangrazio-kulbersh et al. 12 reported a vertical relapse of 33.3% following mandibular advancement, while Mah et al. 16 reported nonsignificant vertical relapse following a mandibular setback.
Three among the five selected articles were categorized under the mandibular advancement group, while the remaining two articles fell into the category of mandibular setback. All the studies were retrospective in nature. With a minimum follow-up of one year, the period ranged from 12 to 95 months in the selected studies. In the present study, the higher incidence of relapse in mandibular setback may be contributed to a larger magnitude of surgical procedure (7.18
Strength and Limitations
The present systematic review attempts to provide comparative data pertaining to the long-term stability of BSSRO procedure, that is, advancement versus setback, which has not been reported in the literature from database inception till 15 June 2021, thereby making this review a maiden attempt. The minimum age of the patient considered for review was 16 years so as to minimize the bias pertaining to the resumption of growth as a cause of relapse. The minimum surgical magnitude chosen was 4 mm, which is usually carried out in clinical practice.
The review has limitations, including the availability of limited data and the inclusion of articles published in English language only which adds to the bias. The present review has taken into consideration the skeletal stability measured at point B only so as to obtain homogenous data. However, articles evaluating stability at point Pogonion are also available. Among the retrieved literature, only four studies compared the stability of BSSRO—advancement with setback; however, these were excluded, as they did not qualify the selection criteria. Consequently, neither group received the data from any single study. Although the data are homogeneous, yet they are obtained from different studies for the two groups.
Conclusion
The following conclusions can be drawn from the present study:
Mandibular setback can be expected to relapse by 21.7–32.3% (mean 27%) in comparison to mandibular advancement accounting for relapse of 2.1–15.4% (mean 7.85%) in adult patients. The long-term skeletal stability of mandibular advancement and setback accomplished with BSSRO differs significantly. Hence, mandibular advancement is a relatively stable procedure.
Footnotes
Author Contributions
All authors meet the authorship criteria. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not required.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.