
Abstract
In orthodontic therapy alone, perhaps in skeletal class III cases with facial asymmetry, achieving an excellent occlusal result and maintaining a stable posttreatment occlusion is difficult. Growth modification should begin before the pubertal growth spurt; there are only 2 options after that. Adults with skeletal class III malocclusions require orthognathic surgery in addition to traditional orthodontic treatment to boost self-esteem, restore normal occlusion, and improve facial harmony. Unquestionably, a multidisciplinary approach is required to achieve exceptional treatment outcomes in adult patients with diverse skeletal and dental issues. In order to provide a comprehensive therapeutic outcome for the patient, an orthodontist must collaborate with a surgeon.
Introduction
In growing patients, skeletal class III may be associated with a functional shift of the mandible because of a narrower maxillary arch and occlusal interferences. According to research, posterior unilateral crossbite develops quickly and spontaneous correction is uncommon. It may cause mandibular and facial asymmetry in growing patients if left untreated, because of mandibular growth and displacement. 1
To increase self-esteem, achieve normal occlusion, and improve facial aesthetics, adults with skeletal class III malocclusion require orthognathic surgery along with traditional orthodontic treatment.2–4 It was determined that psychological features, not morphologic ones, were most likely the driving force behind an individual’s desire to have surgery. Cheng et al 5 also indicated that the patient’s perspective primarily impacted the decision to have surgery. The majority of class III malocclusions are surgically corrected with mandibular retrusion, maxillary protrusion, or a combination of the two, and it is critical to predict the soft tissue changes that can occur with maxillary advancement and mandibular setback surgery.
Case Description
AJ, a 21-year-old male patient, presented to the department of orthodontics and dentofacial orthopedics with the major complaint of a jaw that deviated to the left. The patient was mesocephalic and mesoprosopic on extraoral examination, with a concave profile and incompetent lips. On clinical examination, the patient had angles class III subdivision, a –2 mm reverse overjet, and a –4 mm open bite. On radiographic examination, the patient’s maxilla and mandible were normal, and he had Angle’s class III subdivision on skeletal class III jaw bases and a horizontal growth pattern. The patient’s treatment strategy included fixed orthodontic treatment with pre-adjusted edgewise appliance (PEA) mechanotherapy and MBT prescription, followed by a mandibular setback with a bilateral sagittal split osteotomy (BSSO). Facial aesthetics improved significantly, as did bilateral class I molar and canine relation, normal overjet, and overbite with a class I incisor relation.
Diagnosis and Etiology
AJ complained of his jaw deviating to the left and his inability to bite food with his front teeth. There was no relevant medical history for the patient. Asymmetrical face with enlarged lower anterior facial height, visible inferior sclera, expanded alar base, and lengthy upper lip on clinical frontal examination. At repose, there was no incisal show, with just half of the maxillary incisor crown visible while smiling and an expanded buccal corridor visible (Figure 1A to 1D).
Pretreatment Extraoral Photographs: (A) Frontal with Lips at Rest, (B) Frontal Smile, (C) and (D) Profile.
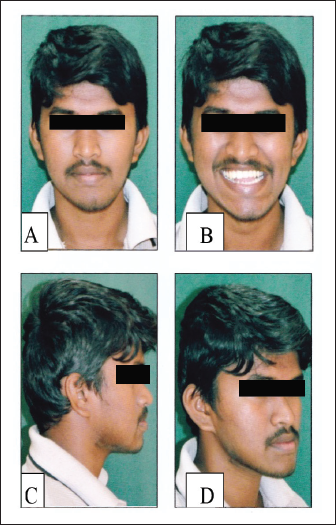
Facial aesthetics improved significantly, as did bilateral class I molar and canine relation, normal overjet, and overbite with a class I incisor relation (see Figure 1A to 1D).
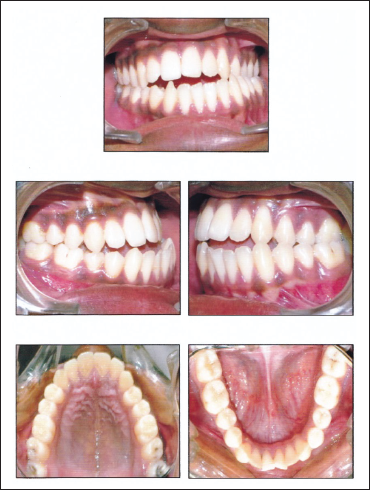
The oral examination revealed that the patient had good dental health and no periodontal issues. Upper arch symmetrical and well-aligned. Both arches had anterior crowding with lower slight rotation. The interarch connection has a 2.5 mm reverse overjet and a 4 mm open bite. In maximum intercuspation with a bilateral posterior crossbite, a class III subdivision with a class III canine connection existed. Compared to the facial midline, the mandibular midline was 2 mm to the left (Figure 2 and Table 2). A straightforward tongue thrust swallow was observed. A temporomandibular joint examination revealed no relation-centric occlusion disparity in the absence of any history of pain or discomfort in the temporomandibular joint or associated muscles. According to Bolton’s analysis, the space study revealed a –2.5 mm shortage in both the maxillary and mandibular arches, a 1.8 mm total mandibular surplus, and a 0.5 mm anterior excess.
Pretreatment Intraoral Photographs.
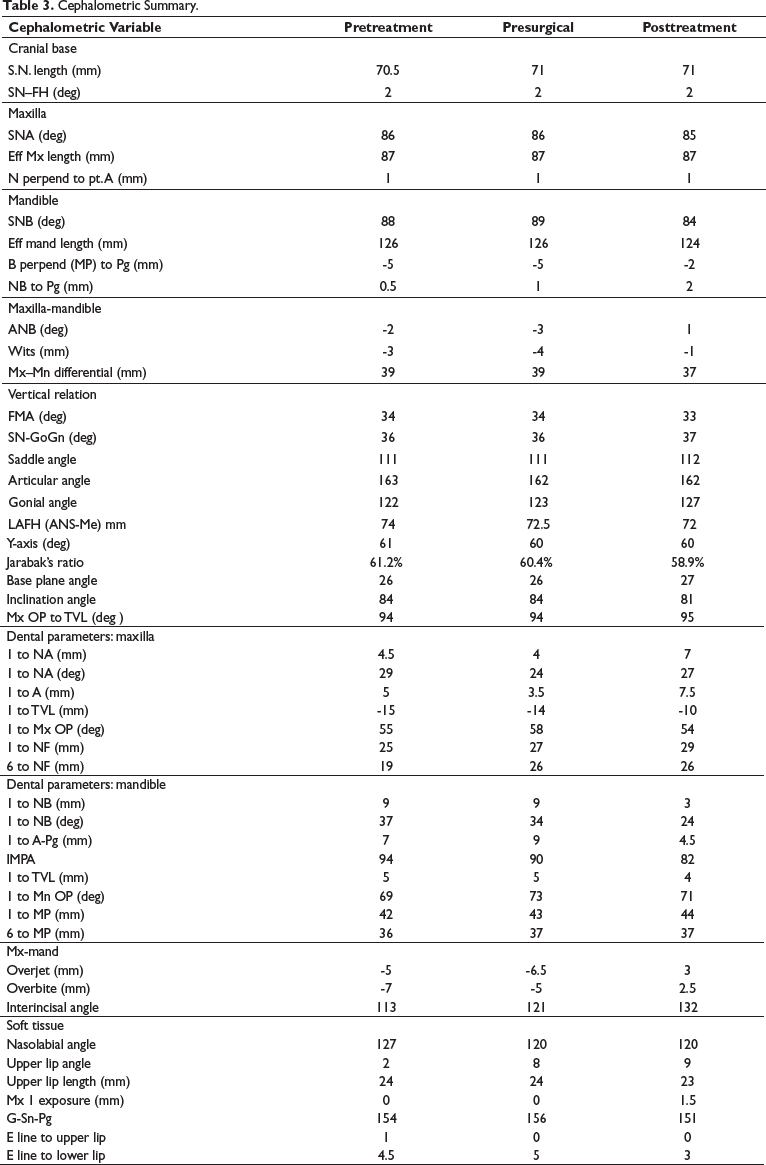
A hyperdivergent class III malocclusion characterized by a short retrognathic maxilla and a large prognathic mandible. It was discovered during a cephalometric examination. There was a minor vertical maxillary deficit. The maxillary incisors were somewhat proclined, but the mandibular incisors were quite upright. The soft-tissue profile revealed a concave profile with increased nasal projection, a sharp nasolabial angle, a protruding lower lip, and an increased throat length. Lower incisor exposure increased upper lip length (Figure 3 and Table 3), but there was no temporomandibular pathology identified by the orthopantomogram (OPG) (Figure 3).
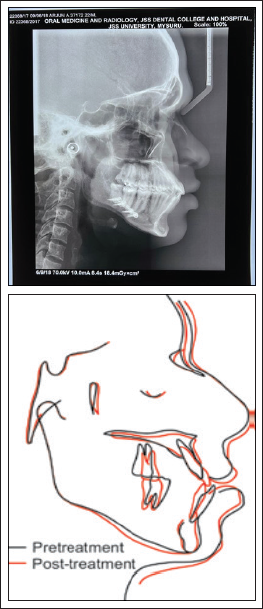
Pretreatment Lateral Cephalogram., Orthopantomogram and A-P Orthopantomogram.
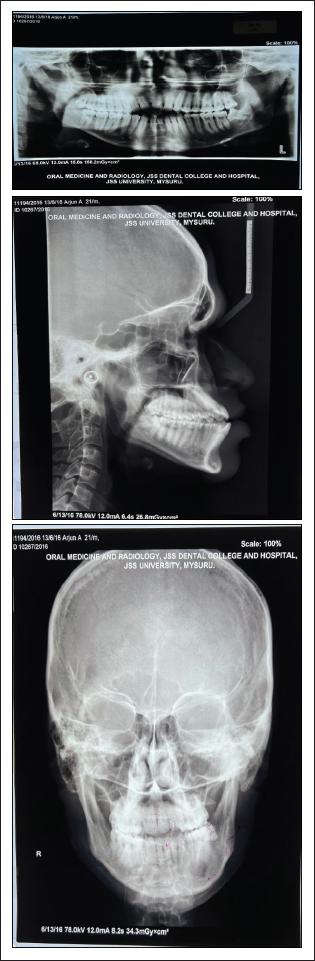
Pretreatment radiographs included a lateral cephalogram, an OPG, and a posterior-anterior cephalogram (Figure 3). The OPG revealed that all permanent teeth were present, with 38 mesioangular impaction and no other permanent teeth showing symptoms of root resorption. All permanent teeth demonstrated adequate alveolar bone height and were free of cavities. A significant amount of facial asymmetry was noticed (Figure 3) in posterior-anterior cephalometric. 6
This adult male was diagnosed with class III skeletal malocclusion, which was a mix of maxillary normognathism and mandibular prognathism with a hyperdivergent growth pattern with an intraoral Angles class III malocclusion with an anterior crossbite, an open bite, and some minor misalignments of individual teeth. Analysis of the soft tissues showed a concave profile, facial asymmetry, and a long upper lip with reduced incisor display.
Problem List
The mandible was shifted to the left side. Left unilateral posterior skeletal crossbite. Lower anterior crowding. Reverse overjet. Open bite.
Treatment Objectives
The objectives were to
achieve a beautiful profile by reducing the lower jaw’s prominence, which will balance the face and enhance the profile; correct the open bite and crossbite in the anterior skeletal region; adjust the arches to rectify the teeth’s inclinations and angulation; achieve an acceptable functional and static occlusion; fix an inadequate incisor display.
Treatment Plan
In the presurgical stage of orthodontic treatment, nonextraction therapy was used to realign the arches and eliminate any obvious compensation. Because of the relatively upright position of the mandibular teeth, decompensation was not necessary in the mandibular arch. To repair the slightly proclined incisors, slenderization of the maxillary arch was intended. There is no need for vertical decompensation. To achieve the intended tooth interdigitation, a BSSO of 6 mm mandibular asymmetrical setback was planned, and this was followed by a brief postsurgical orthodontics period.
Treatment Progress
Orthodontic Preoperative Phase
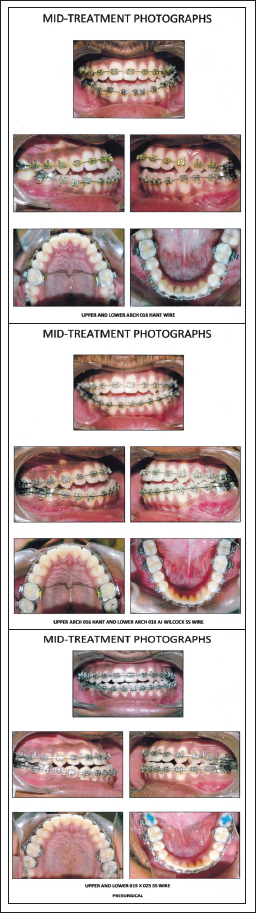
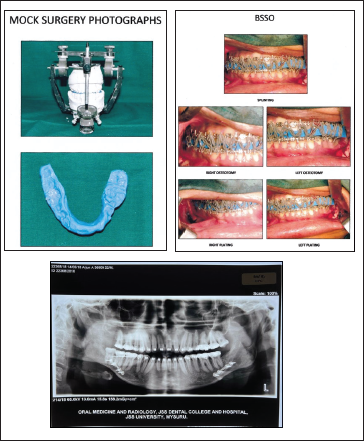
We began with a 0.022" MBT preadjusted edgewise appliance during the presurgical period (Table 1). Using 0.016" NiTi arch wires first, then 0.018" stainless steel, and finally 0.017" to 0.025" stainless steel, the maxillary and mandibular arches were aligned. Finally, stainless steel between 0.019" and 0.025". Before surgery, presurgical records were obtained after the placement of upper and lower coordinated 0.019" and 0.025" stainless steel wires for 4 weeks (Figure 4). At 6 months before surgery, the mesioangular impacted 38 was removed, and a final surgical occlusal wafer splint was made (Figure 5).
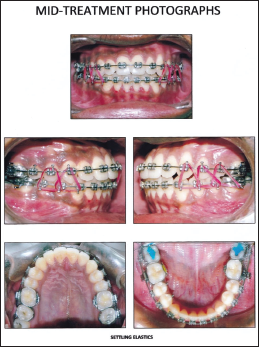
Presurgical Mid Treatment Intraoral View Stages Photograph.
Surgical Phase–Treatment Intraoral View Stages Photograph and OPG.
Operative Phase
Using a BSSO, the mandible was then asymmetrically set back during surgery by 6 mm on the right side and 5 mm on the left side (BSSO). With the aid of surgical plates, the splint was then used to position and stabilize the mandible (Figure 5).
Postoperative Phase
The stabilizing elastics and the splint were taken off 4 weeks after surgery. With the help of settling elastics and 0.014" stainless steel arch wires, postsurgical leveling and final detailing were accomplished. Total 18 months were spent on treatment (Figure 6, Table 1). The upper fitted lingual bonded retainers were placed in position after the lower and upper arch brackets were debonded.
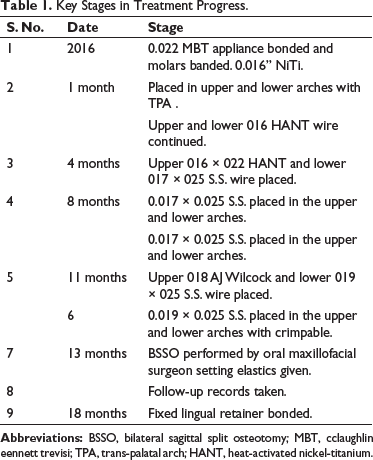
Key Stages in Treatment Progress.
Postsurgical Phase–Treatment Intraoral View Stages Photograph.
Treatment Outcomes
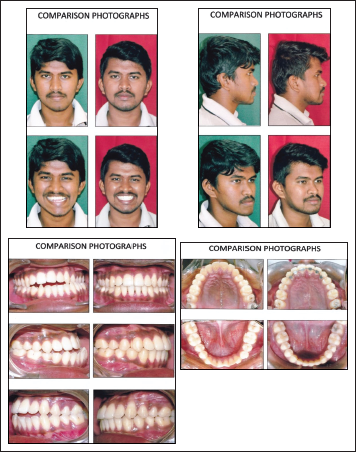
The treatment’s goals were accomplished. There was no unattractive throat sagging, and facial aesthetics improved significantly. When at rest, the incisor is visible and smiling has greatly improved. Class I buccal occlusion and proper alignment of the maxillary and mandibular arches were both accomplished with corrected anterior open bite and crossbite (Figures 7 and 9). With facial harmony in the projections of the nose, lips, and chin as well as an outstanding aesthetic balance between the hard and soft tissue, cephalometric superimposition revealed a significant improvement in the facial profile (Figure 8).
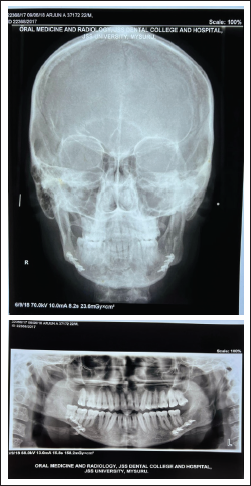
Posttreatment Radiograph A-P View Cephalogram and OPG.
Posttreatment Changes Cephalometric Superimposition.
Comparison Photograph Treatment Intraoral View Stages.
Critical Appraisal
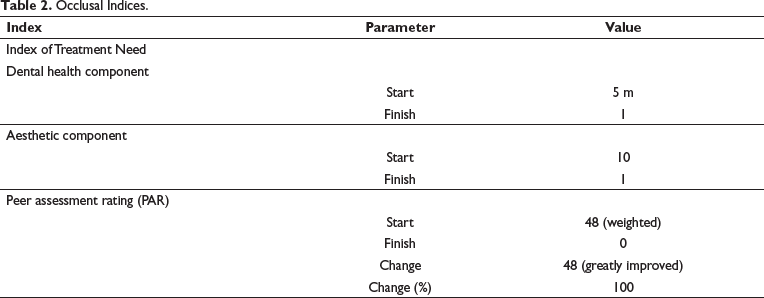
Over 18 months, AJ underwent successful treatment using a combination of orthodontic and orthognathic surgical treatments. The therapy goals and the patient’s complaints were both addressed. The peer assessment rating (PAR) and index of orthodontic treatment need (IOTN) ratings showed that we had outstanding occlusal and cosmetic results.
Dental and skeletal alterations led to an improvement in the facial profile.
Angle’s class I molar and canine relation was attained, and fixed lingual bonded retainer and removable Begg’s retainer were delivered in the upper and lower arches, respectively.
After comprehensive fixed orthodontics, the maxillary incisor inclination was slightly over ideal, and root uprighting concerns 44, 45 were successful.
A multidisciplinary strategy was used to control skeletal open bite, jaw deviation, and facial asymmetry. The patient received signed consent after being told of the surgical complications. The case’s overall outcomes were satisfactory.
During follow-up, the condition of the third molars was assessed, and for the ones that were supraerupted or in an undesirable position, extractions were indicated. 7
Discussion
IBO category III demands either a vertical discrepancy with an frankfort-mandibular plane angle (FMA) angle greater than 35° or less than 20°, or a transverse discrepancy—complete unilateral or bilateral posterior crossbite. With an relationship of maxilla to mandible (ANB) of –2° and an FMA of 33°, the aforementioned example qualified as class III and was therefore included. It is impossible to treat severe cases of class III asymmetrical malocclusion with orthodontics alone. For enhancing occlusion, masticatory function, and, more crucially, aesthetics and facial balance, an orthosurgical approach becomes unavoidable. 8
In this patient, nonextraction reverse orthodontics is required before surgery to address incisor torque, leveling, and arch alignment, as well as to allow a surgeon to perform surgery to achieve perfect facial outcomes. Presurgical orthodontics must so be planned. Clinical success after orthognathic therapy can be defined as a combination of the following factors: patient satisfaction, accurate static and functional occlusion, patient comfort, chewing, no temporomandibular joint pain, and result stability (Tables 2 and 3).
Occlusal Indices.
Cephalometric Summary.
Conclusion
Orthodontics combined with orthognathic surgery is an ideal combination for correcting skeletal abnormalities. Both professions necessitate skill, and they collaborate at all stages of treatment, both presurgical and postsurgical. A multidisciplinary approach assists us in achieving ideal goals and satisfying outcomes on the oral, facial, skeletal, and psychological levels.
Footnotes
Acknowledgment
We are grateful to the Oral Maxillofacial Surgery faculty of JSS Dental College and Hospital in Mysuru for their support and direction throughout the surgery. I would like to express my heartfelt appreciation to my lecturers and colleagues at the Department of Orthodontics and Dentofacial Orthopedics, JSS Dental College and Hospital, Mysuru
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
The author certifies that he has obtained all appropriate patient consent forms. The patient has the consent to use the clinical photographs for publication in the journal.