
Abstract
Background:
Skeletal nongrowing class II patients with retrognathic mandible are often at risk of developing obstructive sleep apnea (OSA). This skeletal discrepancy, when severe enough, is often addressed by surgical mandibular advancement which not only achieves aesthetics, structural balance, and functional efficiency but also improves the airway function.
Objective:
The aim of the study was to evaluate the effectiveness of surgical mandibular advancement on airway dimensions, in nongrowing skeletal class II patients with mandibular retrognathism associated with OSA.
Materials and Methods:
The sample consisted of 8 patients with skeletal class II due to retrognathic mandible associated with OSA. Screening was done with functional outcomes of sleep questionnaire (FOSQ) score and confirmed with polysomnography. Pretreatment and posttreatment airway dimensions/volume were assessed and calculated on cone beam computed tomography (CBCT). Three months post surgery, oxygen saturation was recorded.
Results:
A statistically significant improvement in mean oxygen saturation level was observed from 87.62 ± 7.70 to 97.75 ± 0.46 and mean increase in airway volume was from 48.60 ± 7.17 to 69.48 ± 26.22. The smallest cross section increased from 137 ± 74.37 to 253.75 ± 76.67. Anteroposterior dimensions increased significantly from 6.17 ± 1.78 to 9.33 ± 2.07 and transversed from 24.56 ± 6.41 to 30.14 ± 3.35. FOSQ score improved from 9.37 ± 2.61 to 15.25 ± 0.88.
Conclusion:
Surgical mandibular advancement is an effective treatment option in improving airway dimensions in nongrowing skeletal class II patients with mandibular retrognathism associated with OSA.
Introduction
Obstructive sleep apnea (OSA) is a highly prevalent condition with a prevalence of 6.2% in Indian population. 1 It is characterized by increased nocturnal airflow resistance resulting in repetitive episodes of pharyngeal collapse during sleep. The impact on quality of life is almost similar to that experienced by those with other chronic disorders of moderate severity. 2
Various risk factors associated with OSA are obesity, gender, genetics, craniofacial disorders, and skeletal patterns. 1 Skeletal class II with mandibular deficiency often compresses the airway predisposing to OSA. In growing patients, growth modification works best; however, in adults, surgical advancement of mandible is the most suitable treatment option. This treatment option not only improves the aesthetics, structural balance, and functional efficiency but also improves the airway function. 3 There are various studies on the effect of maxillomandibular advancement (MMA) on pharyngeal airway (PA) dimensions 4 ; however, there is paucity of literature regarding the effect of surgical mandibular advancement alone on OSA.
Thus, the aim of this study was to evaluate the effectiveness of surgical mandibular advancement in nongrowing skeletal class II patients with mandibular retrognathism associated with OSA on airway dimensions using CBCT. The improvement in quality of life of these patients was also assessed using the functional outcomes of sleep questionnaire (FOSQ). 5
Material and Methods
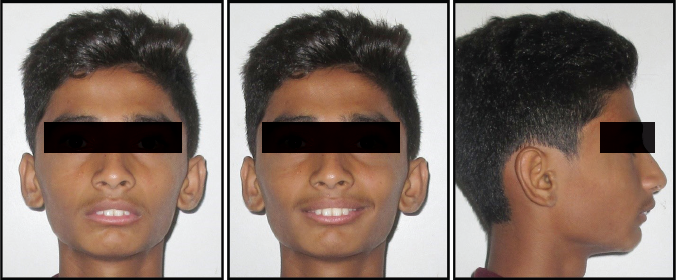
The sample consisted of 8 patients (5 males and 3 females) in the age group of 18 to 30 years. All patients had an average body mass index in the range of 17 kg to 22 kg per square meter. Adult patients reporting to the department with chief complaint of difficulty in breathing during night, daytime sleepiness, and snoring were considered. Among them, those patients with a class II mandibular deficiency and no underlying systemic disease/syndrome or any history of adenoidectomy were selected for the study. The cohort consisted of 40 patients. Diagnosis and treatment planning were done for each patient after detailed case history, clinical examination, and analysis of records (study models, cephalogram, OPG, photographs) (Figures 1, 2 and 11). Cervical Vertebrae Maturation Index staging was performed to confirm absence of any remaining growth. To assess the quality of life in each patient, FOSQ was explained and filled by each patient. This questionnaire originally comprises 5 domains; however, since most of the patients were unmarried, the fifth domain was excluded from the study. The questionnaire of each individual patient was given a score. The cohort consisted of 40 patients, out of which 28 patients had a score of less than 10 suggesting a poor quality of life. These patients were referred to a sleep physician for nocturnal polysomnography test (PSG), a confirmatory test for OSA (Table 1). Of the 28 patients, 20 patients were diagnosed with mild to severe OSA with a minimum frequency of obstructive respiratory events 15/h. These patients were treated conservatively by mandibular advancement device 6 and were followed up every month for assessment of compliance and reduction in symptoms. After a follow-up of 6 months, 10 patients showed no improvement in symptoms. Surgical treatment option of mandibular advancement to mitigate the symptoms was explained to these patients, out of which only 8 patients gave consent for surgery.
Pretreatment Extraoral Photograph.
Pretreatment Intraoral Photograph.

Distribution of Patients According to AHI After Polysomnography.

A written informed consent was obtained from all the patients. The study was approved by the Institutional Ethics Committee (No. MUHS/PG/E-2/2386/16) and is in accordance with the Helsinki Declaration of 1975.
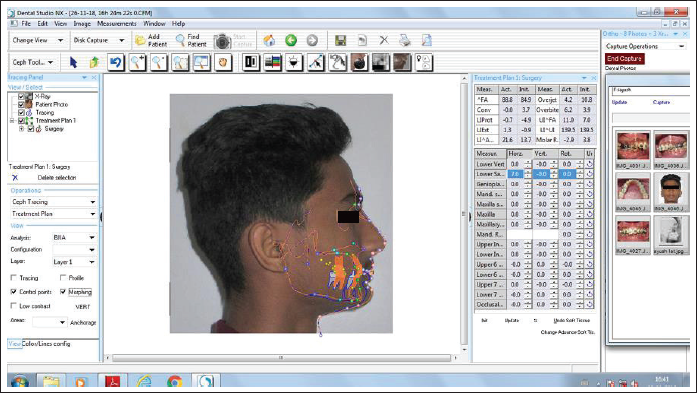
In all 8 patients, presurgical orthodontics was carried out by fixed mechanotherapy with MBT 0.022 slot (ORTHO Organizers). After the initial alignment was completed, a final working wire 19″×25″ SS (G&H, Orthoforce) was placed (Figure 3). Leveling was done postsurgically, which is desirable in patients with mandibular advancement. Presurgical records (T1) (models, cephalogram, OPG, photographs, and CBCT) were taken. Prediction tracing was done using Nemotec Medical Studio Software (Figure 4). Mock surgery was carried out and intraoral splint was fabricated for the mandibular advancement surgery.
Post Alignment.

Computerized Presurgical Superimposition.
CBCT was taken to assess the airway dimensions and volume. Before recording the CBCT, bite registration was done with the patient in the supine position and the same bite record was used during CBCT acquisition. Images were taken on a CBCT machine (Promax 3D Mid; Planmeca) and Romexis software (version 3.2.0.r; Planmeca). The scanning protocol was 120 kV, 5 mA, 13 × 3 × 17 cm field of view, 0.25-mm voxels, and a scanning time of 40 s. Patients were instructed to avoid tongue movement and swallowing during the consecutive CBCT scans. The CBCT volumetric data sets were imported in DICOM files into the Romexis software, a software package that reconstructs 3-dimensional (3D) images and facilitates accurate measurements. Once imported, the 3D reconstructions were oriented in a precise manner so that the Frankfort horizontal plane was parallel to the axial plane. The midsagittal plane was oriented to the subject’s midline. The coronal plane was oriented so that it passed through both the left and the right porion points. The airway analysis tool was used to define the portion of the upper airway of interest. This portion was the velopharynx and the oropharynx, defined with the superior border as the horizontal line through the posterior nasal spine on the midsagittal image, and the inferior border as the horizontal line through the superior point of the epiglottis on the midsagittal image. The airway analysis tool calculated the volume and cross-sectional areas of different slices of the defined portion of the airway. It also generated JPEG files of cross-sectional areas. A pretreatment CBCT was taken before surgery and posttreatment after 3 months of mandibular advancement surgery.
For volume determination, all 3 axial views (transverse, sagittal, and axial) were checked to ensure that the airway was included in the selected area. The threshold value was set to 73 for all patients to obtain a solid airway volume. 3 Threshold is a tool in the Romexis software that controls the filling degree of the empty airway space. Generally, the increase or decrease of the threshold results in a greater or smaller airway volume, respectively. Adjustments of brightness and opacity values and removal of unwanted voxels were done before calculating the final airway volume. Once segmentation was performed, the software automatically computed the volume of the oropharyngeal region in cubic millimeters.
Other measurements recorded included the smallest cross-section (SmCa), the point where the airflow is theoretically the most constricted, which is the limiting factor in airflow during respiration: the anteroposterior linear dimension of the smallest cross-sectional area and the transverse dimension of the smallest cross-sectional area.
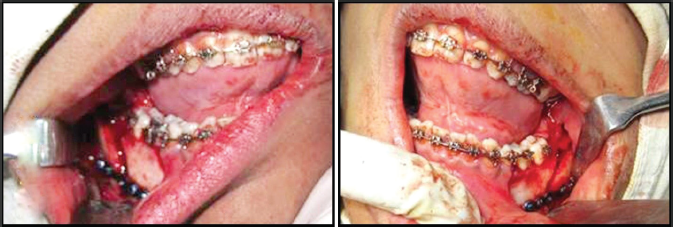
A bilateral sagittal split osteotomy for mandibular advancement was done under general anesthesia by an oral surgeon (Figure 5). Postsurgical records (T2) were taken 3 months after surgery followed by postsurgical orthodontics (Figures 6 and 7). Since level I polysomnography is expensive post surgery, level IV test with pulse oximeter was performed. A second FOSQ was given after a period of 3 months.
Mandibular Advancement Surgery.
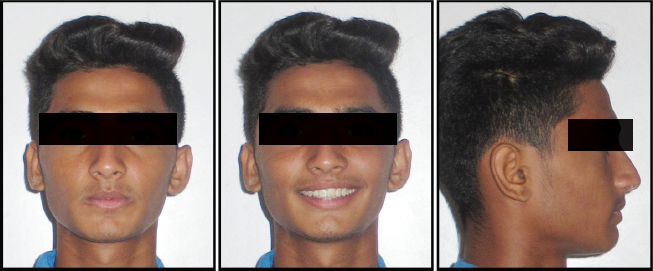
Posttreatment Extraoral Photograph.
Posttreatment Intraoral Photograph.

SPSS Version 20.0 software was used. All parameters were summarized in terms of means and standard deviations. The comparison of means of each parameter was performed before and after treatment using paired t tests. The data was checked for normality of distribution before using the t test to evaluate intergroup differences.
Results
FOSQ score improved significantly from 9.37 ± 2.61 at T1 to 15.25 ± 0.88 at T2. The difference in the means was highly significant with P < .001 using paired t test. Mean oxygen saturation (SaO2) level improved from 87.62 ± 7.70% to 97.75 ± 0.46%. This improvement was statistically significant.
CBCT Parameters
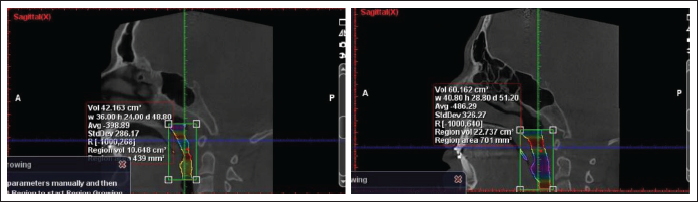
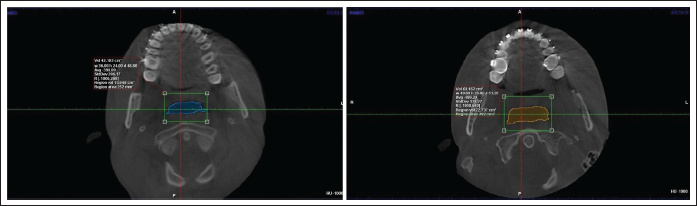
The pretreatment mean airway volume of 49.60 ± 7.17 cm3 increased to 69.48 ± 26.22 cm3 posttreatment. The mean SmCa area was 137 ± 74.37 mm2 pretreatment, improved to 253.75 ± 76.67 mm2 posttreatment (Figures 8 and 9). Mean pretreatment anteroposterior width of airway observed was 6.17 ± 1.78 mm. Posttreatment anteroposterior width increased to 9.33 ± 2.07 mm, which was statistically significant (P < .001). Mean pretreatment transverse airway width of 24.56 ± 6.41 mm increased to 30.14 ± 3.35 mm posttreatment (Table 2; Figure 10).
Change in Smallest Cross-Section of Airway With Mandibular Advancement Surgery in Sagittal Plane.
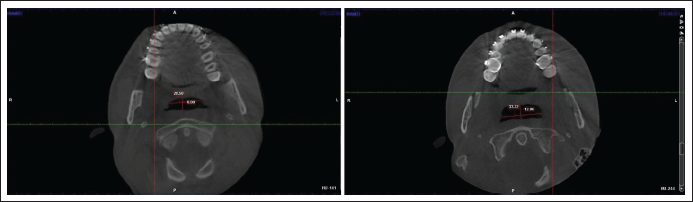
Change in Smallest Cross-Section of Airway With Mandibular Advancement Surgery in Transverse Plane.
Change in Anteroposterior and Transverse Dimension of Smallest Cross-Section With Mandibular Advancement Surgery.
Pretreatment Radiographs.

Statistics for CBCT Parameters: Pretreatment and Posttreatment (Three Months After Mandibular Advancement Surgery).
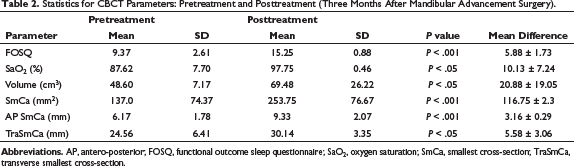
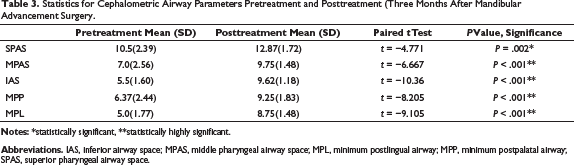
Statistically significant increase in airway volume and highly significant increase in SmCa area was observed. SmCa area in anteroposterior dimension showed a highly significant increase and in transverse dimension showed a significant increase with mandibular advancement surgery.
Cephalometric Parameters
Statistics for Cephalometric Airway Parameters Pretreatment and Posttreatment (Three Months After Mandibular Advancement Surgery.
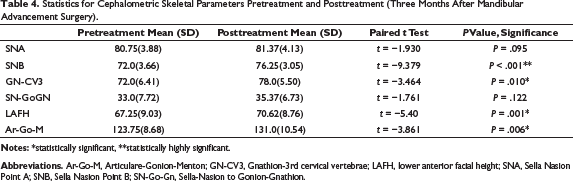
Statistics for Cephalometric Skeletal Parameters Pretreatment and Posttreatment (Three Months After Mandibular Advancement Surgery).
Discussion
Skeletal class II malocclusion comprises a significant proportion of orthodontic patients. In adults with skeletal class II, the only option is camouflage or surgery. Although these patients come primarily for aesthetics, often the underlying craniofacial abnormality of a deficient mandible may serve as a significant predisposing factor for sleep disordered breathing or sleep apnea. The treatment approach should be planned taking into consideration the risk of future development of airway problems as well as the effect of treatment on the airway.
Sleep questionnaire (FOSQ) serves as a diagnostic screening test in individuals with sleep disordered breathing. Weaver et al 5 was the first to describe this self-report measure to assess the impact of disorders of excessive sleepiness on multiple routine activities of everyday life as overall activity level, vigilance, general productivity, social behavior, and physical intimacy.
Decreased FOSQ scores indicate increased daytime sleepiness and vice versa. Dattilo and Drooger 8 used an Epworth Sleepiness Scale to compare with overnight sleep study. However, in the present study, ESS scale was not used as it cannot distinguish sleepiness as a result of disturbed sleep or resulting from other causes such as medication effect. Significant improvement in FOSQ score after mandibular advancement surgery showed a reduction in daytime sleepiness and improved quality of life of these patients.
Sleep questionnaire is a screening test for OSA but the gold standard is level I polysomnography. It gives the apnea-hypopnea index (AHI), an index that grades the severity of OSA into mild (5-15), moderate (15-30), and severe (>30). In the present study, 4 patients had mild OSA, 2 patients had moderate OSA, and 2 patients had severe OSA. The mean AHI index was 17.68 ± 10.54 with minimum AHI of 9 events/h and maximum of 35.4 events/h. In all the patients, level I polysomnography was carried out prior to treatment. A level IV test was done posttreatment (use of pulse oximeter to record oxygen saturation and pulse rate at home). Although PSG is treated as the gold standard for diagnosing OSA, it is labor-intensive, time-consuming, and expensive. The overnight pulse oximetry is a highly effective diagnostic tool for moderate to severe OSA patients. 9 It is an inexpensive method to check and monitor oxygen saturation at home. Normal SaO2 in healthy individual is 95% to 100%. In our study, mean SaO2 level improved from 87.62 ± 7.70% to 97.75 ± 0.46%. Similar improvements in SaO2 level were reported by Riley et al 10 and Li et al. 11 Noller et al 12 reviewed mandibular advancement in adult OSA patients. In their study, the oxygen saturation (55 patients) increased from 71.9 ± 14.6% to 89 ± 11.0%. They stated that current literature supports isolated mandibular advancement as an efficacious treatment modality for adult OSA with mandibular deficiency.
Most of the earlier studies have used lateral cephalograms to assess skeletal position and airway space. Lateral cephalograms only provide a 2D means to assess 3D spatial relationships of the airway and skeletal position. However, a 2D image only determines the area of airway space; in reality, it is the volume that represents the complex dynamic of the 3D structure. Cone beam computed tomography (CBCT) serves as the best assessment tool to measure 3D volume.
The mean increase in airway volume post surgery in the present study was from 48.70 ± 7.17 cm3 to 69.48 ± 26.22 cm3. The findings are in accordance to those reported by El et al. 13 They found an improvement in volume from 7,957.8 mm3 to 14,433.5 mm3 (7.9578 cm3 to 14.4335 cm3). This increase in airway volume shows increased airway flow, which improves the patient’s quality of life (FOSQ scale) and oxygen saturation level. The pretreatment and posttreatment airway images showed increase in size of the upper airway in the lateral, anterior, and posterior views.
The smallest cross-section area of the upper airway is a limiting factor for airflow. This SmCa of the upper airway causes maximum resistance to airflow, and it is a site of obstruction of the airway during sleep in patients with OSA. The prognosis of the different treatment modalities in the management of these patients depends on an increase or a decrease in the SmCa of the airway. Hence, an increase in the SmCa of the upper airway is a definite indicator of improvement of airflow and airway volume. Anteroposterior and transverse measurements of the upper airway present the exact nature of collapse at the site of obstruction.
There was an increase in SmCa area from 137.0 ± 74.37 mm to 253.75 ± 76.67 mm. The findings of our study are in accordance to those reported by Hernández-Alfaro et al. 14 They found an improvement in SmCa area from 46.3 mm2 to 170.7 mm2. The anteroposterior dimension at the SmCa of the airway shows the severity of the obstruction of the upper airway in the sagittal plane. With a mandibular advancement surgery, the smallest cross-section of the airway in sagittal plane increased by a mean of 3.16 mm and in transverse plane by 5.58 mm. Several studies15-17 have shown influence of mandibular advancement surgery on the PA space. Mandibular advancement surgery is a well-established procedure in the treatment of patients with retrognathic mandible with concomitant beneficial effect on PA.
Majority of the systematic reviews18, 19 have focused on the effect of MMA on PA which undoubtedly increases the airway size, but there has to be a definite indication to carry out such procedure. Eggensperger et al 20 reported that mandibular advancement surgery alone does not achieve a stable increase of PA size over a long-term period of 12 years. Another recent systematic review was carried out on the effect of surgical MMA on PA dimensions and the AHI in the treatment of OSA, with the aim of determining whether increased PA in the context of MMA is the main factor conditioning the subsequent decrease in AHI. 4 They concluded that there is sufficient evidence to conclude that MMA significantly increases PA dimensions and ensures a final AHI score below the threshold of 20 events/h, obtaining a mean SR of 87.5%. However, further studies are needed to individualize the required magnitude and direction of surgery-induced movements for each patient.
The limitation of the present study was that the CBCT assessment was diurnal with the patient in the upright position. This limitation was partly overcome by bite registration in the supine position. However, the effect of soft palate, tongue, and other adjacent soft tissue structures were not taken into account. Therefore, it does not accurately simulate the pharyngeal dimensions during sleep. The sample size was comparatively smaller. Additionally, the amount of surgical relapse and long-term prognosis has not yet been evaluated as the patients are still under follow-up.
Conclusion
Skeletal class II patients with mandibular retrognathism should be routinely screened for OSA.
Mandibular advancement surgery is an effective surgical treatment option not only in improving the aesthetics and function but also in improving the airway dimensions and volume overcoming the future risk associated with OSA.
It is vital to holistically correct the dentofacial malocclusion to improve the quality of life.
Future Perspectives
The patients included in the present study are being followed up for a long-term objective evaluation of improvement in OSA symptoms.
Footnotes
Authors’ Contributions
All the above authors have contributed to the work, and agree with the presented findings and that the work has not been published before nor is being considered for publication in another journal. Procedures involving experiments on human subjects are done in accordance with the ethical standards of the Committee on Human Experimentation of the institution in which the experiments were done in accord with the Helsinki Declaration of 1975.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committee (No. MUHS/PG/E-2/2386/16) and is in accordance with the Helsinki Declaration of 1975.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.