
Abstract
This case report was presented in the Indian Board of Orthodontics examination under category II in September 2020. It demonstrates the one-phase treatment of a skeletal class II malocclusion in a 11 year-4-month old female using a combination of functional and fixed appliance therapy. The treatment summary along with various supporting records are reprinted here with minimal editing and reformatting so as to reproduce the actual documents submitted to the board.
Introduction
Class II malocclusion comprises a broad array of specific skeletal, dental, and soft tissue features. It ranks second in distribution and prevalence among Angle’s classes of malocclusion. 1 However, it is the most frequently encountered and treated malocclusion in orthodontic practice.
Mandibular deficiency, rather than maxillary excess, is reported to be the most common cause of skeletal class II malocclusion. 2 In such cases, growth modulation using functional jaw orthopedics has been the widely accepted treatment modality when sufficient favorable growth remains. 3 The choice of a particular appliance among the plethora of functional appliances depends on a case-based analysis and the clinician’s choice. The Twin-block appliance is found to be the most preferred removable functional appliance.
The case report presented below illustrates 1-phase treatment of a 11-year-old female with a skeletal class II malocclusion using the standard twin-block appliance followed by comprehensive fixed appliance.
Case Report
JJ, a 11 year-4-month old prepubertal female of South Indian origin in early permanent dentition stage presented with class II division 1 malocclusion on a moderate class II skeletal base attributed to mandibular deficiency with an average growth pattern. The mentolabial sulcus was deep with an everted lower lip and presence of lip trap. There was significant proclination of upper incisors and mild proclination of lower incisors, having an overjet of 8 mm and 60% overbite. The lower anterior were supraerupted with an accentuated curve of Spee. There was midline diastema of 1 mm in the upper arch with mesiopalatal rotation of 16 and crowding of 3 mm in the lower arch. She was in Cervical Vertebrae Maturation Index (CVMI) stage 3 with a positive clinical visualized treatment objective (VTO).
A growth modification treatment was planned using twin-block appliance for the correction of mandibular retrusion followed by nonextraction comprehensive orthodontic treatment for establishing occlusion. Appreciable improvement was achieved with facial esthetics and a stable buccal occlusion was established with bilateral class I molar and canine relation, normal overjet, and overbite with a class I incisor relation. Peer Assessment Rating (PAR) Index scores improved from 30 to 2 at the end of treatment with a change of 93.3%.
Section I: Pretreatment Assessment Details
Initials: JJ
Gender: Female
Date of birth: July 5, 2007
Age at start of treatment: 11 years 4 months and 22 days
Patient’s complaint: “Top front teeth are sticking out”
No relevant medical, dental, and family history were revealed.
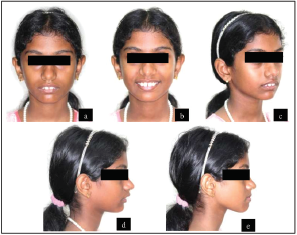
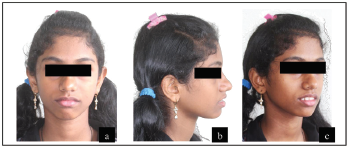
Clinical Examination: Extraoral Features
The pretreatment extraoral photographs are given in Figure 1.
Skeletal Assessment
Soft Tissue Assessment
Upper lip was normotonic whereas lower lip was hypertonic and everted. There was markedly negative lip step with the upper lip in line while the lower lip 3 mm short of Ricketts’ E line. Lips were potentially competent at rest with an inter-labial gap of 5 mm. Anterior oral seal was created by lip-to-lip contact with perioral hyperactivity. The mentolabial sulcus was deep with presence of lip trap. Nasolabial angle was average. Smile arc was nearly consonant.
TMJ Assessment
No signs or symptoms of TMD.
Clinical Examination: Intraoral Features
The pretreatment intraoral photographs are given in Figure 2.

Crowding/Spacing
Maxillary arch: U-shaped arch form. Symmetrical with proclination and spacing of 1 mm between the central incisors (midline diastema). Buccal segments are aligned with mesiopalatal rotation of 16.
Mandibular arch: U-shaped arch form. Symmetrical with mild crowding of the anterior segment. Buccal segments are aligned.
Occlusal Features
Incisor relationship: Class II division 1
Overjet (mm): 8 mm
Overbite: 4 mm (60%)
Centerlines: Upper and lower dental midlines were coincident with facial midline
Left and right buccal: Molars in half unit class II (End on by 3.5 mm)
egment relationship: Canine relation was end-on
Crossbites: None
Displacements: Lingual displacement of 42
Other occlusal features: Curve of Spee of 3.5 mm
Model analysis: Bolton’s analysis revealed overall mandibular tooth material excess of 0.7 mm and anterior maxillary excess of 1.3 mm. Carey’s analysis showed a space deficiency of 3 mm while the arch-perimeter analysis showed a space excess of 2 mm.
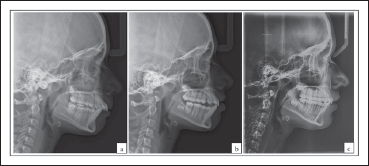
General Radiographic Examination
Pretreatment Radiographs Taken
Lateral cephalogram on November 21, 2018 (Figure 3)
Orthopantomogram on November 21, 2018 (Figure 4)
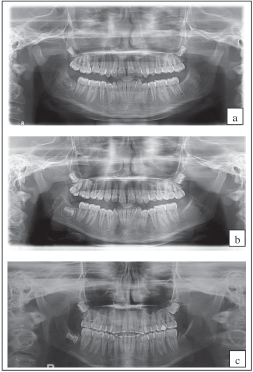
Relevant Radiographic Findings
The normal compliment of permanent teeth was present with no abnormalities in tooth forms as well as the surrounding structures. The lower left third molar was congenitally absent while those in the other quadrants were unerupted. The crestal bone level was normal.
Pretreatment Cephalometric Findings and Their Interpretation
The pretreatment cephalometric values are provided in Tables 1 and 2.
Cephalometric Findings at Different Stages of Treatment.
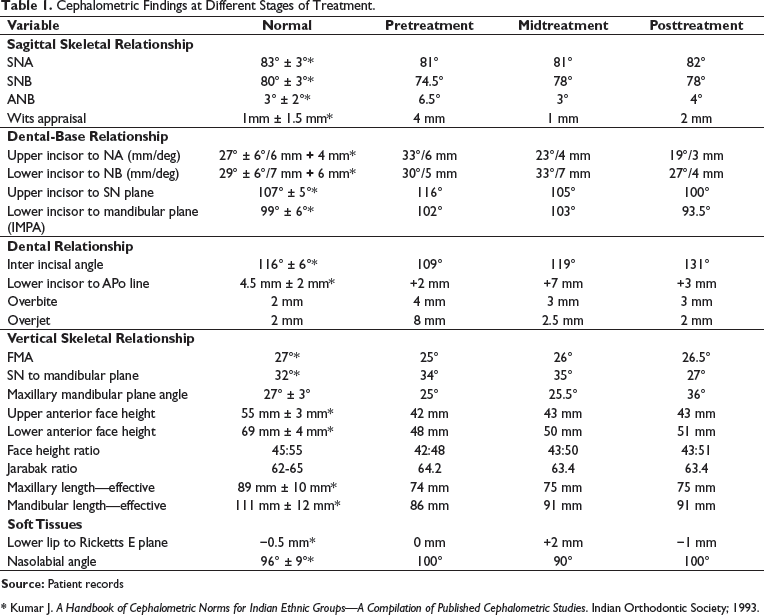
* Kumar J. A Handbook of Cephalometric Norms for Indian Ethnic Groups—A Compilation of Published Cephalometric Studies. Indian Orthodontic Society; 1993.
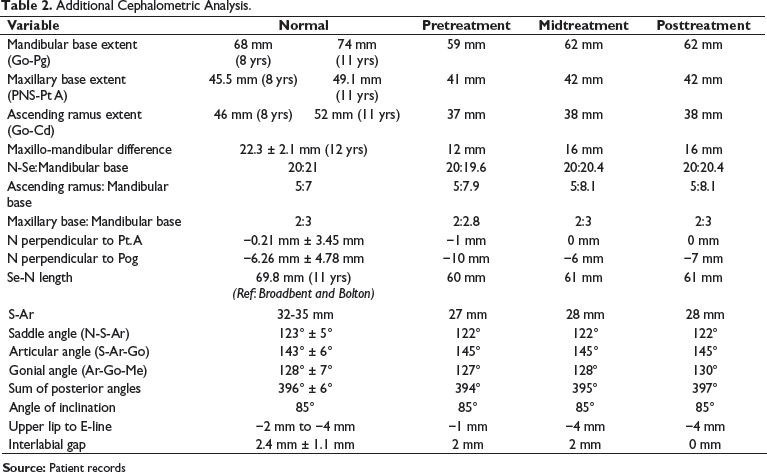
Additional Cephalometric Analysis.
Diagnostic Summary
The skeletal and dental relationships confirmed a class II skeletal base malocclusion due to retrognathic mandible with a favorable growth pattern and class II molar and end-on canine relation on either side. The mentolabial sulcus was deep with an everted lower lip and presence of lip trap, and an increased overjet of 8 mm. The maxillary arch was U shaped with a mesiopalatal rotation of 16. Overbite was deep with significant upper incisor proclination. There was midline diastema of 1 mm in the upper arch and crowding of 3 mm in the lower arch. She was in CVMI stage 3 with a positive clinical VTO.
Problem List
Class II skeletal pattern due to retrognathic mandible, deep mentolabial sulcus, and convex profile.
Class II division 1 incisor relation with 8-mm overjet and class II molar relationship.
60% deep bite.
Proclined and spaced upper incisors with mesiopalatal rotation of 16.
Mild crowding of the lower incisors.
Everted lower lip with deep mentolabial sulcus.
Aims and Objectives of Treatment
Maintain good oral hygiene throughout treatment.
Correction of the class II skeletal base relationship by mandibular growth modulation.
Correction of upper incisor proclination, limit the lower incisor proclination, and correct the overjet.
Correction of deep bite by differential eruption of the posteriors.
Level, align with derotation of the upper molar, and coordinate the dental arches.
Achieve class I molar and canine relation bilaterally.
Achieve class I incisor relation and a coinciding midline.
Achieve ideal soft tissue aesthetics and a consonant smile.
Retain the corrected result.
Treatment Plan
A one-phase comprehensive treatment was planned with myofunctional appliance therapy using Twin-block appliance, immediately followed by upper and lower preadjusted edgewise fixed appliance (0.022″ × 0.028″ MBT) to derotate, level, align, and detail the occlusion.
Construction bite for Twin-block was planned with a sagittal advancement of 7 mm, and vertical/interincisal opening of 2 mm, keeping in mind the freedom of movement and sufficient height for the posterior blocks of 6 mm in the premolar region and 2 to 3 mm toward the terminal molar.
Initial derotation of 16 was planned with NiTi aligning archwires using second molar as source of anchorage. In later stages (0.016″ SS and 0.018″ SS), asymmetric offset bends (toe-in) were used for final derotation and its maintenance thereafter.
Proposed retention strategy: Post Twin-Block therapy during the transition phase, an anterior inclined bite plane (AIBP) retained using ball end clasp was planned simultaneously with fixed appliance until rigid archwires with class II mechanics were to be initiated. Following debonding, bonded lingual retainers (3-3) in upper and (3-3) in lower along with upper (with AIBP) and lower wrap around retainers for night-time wear were planned.
Prognosis for stability: Considered to be good, if proper occlusal interdigitation and control of upper incisors by lower lip at rest is achieved at the end of treatment.
Section II: Treatment
Treatment Progress
Start of active treatment: Functional Jaw Orthopaedics: November 27, 2018
Comprehensive Orthodontics: October 30, 2019
Age at start of active treatment: 11 years 4 months and 22 days
End of active treatment: October 28, 2020
Active treatment time: 23 months
FJO (11 months) and Fixed Orthodontics (12 months)
End of retention: Ongoing
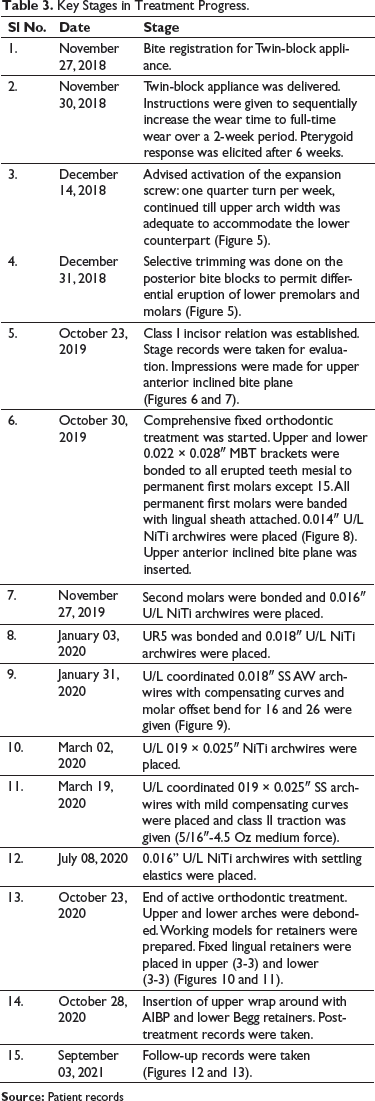
Key Stages in Treatment Progress
Key Stages in Treatment Progress.



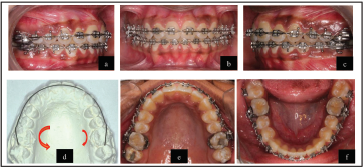




Mid-Treatment (Postfunctional) Records
The mid-treatment extraoral and intraoral photographs are given in Figures 6 and 7, respectively.
Lateral cephalogram on October 23, 2019 (Figure 3).
Orthopantomogram on October 23, 2019 (Figure 4).
Midtreatment Cephalometric Findings and Their Interpretation
Tables 1 and 2 provide the midtreatment cephalometric values.
The cephalometric analysis revealed a significant decrease in the class II skeletal anteroposterior relationship with an ANB of 3° (from 6.5°) and a Wits appraisal of +1 mm (from +4 mm). There was improvement in the linear measurements of the jaw bases: effective mandibular length improved from 86 mm to 91 mm, and mandibular base extent improved from 59 mm to 62 mm.
The notable changes observed were:
Improvement in the N perpendicular to Pog distance by 4 mm (from −10 mm to −6 mm). There was a marginal increase in the vertical skeletal parameters: Base plane angle (from 25° to 25.5°), mandibular plane angle (SN-Go-Gn, 34° to 35°), and a decrease in the Jarabak ratio (from 64.2% to 63.4%). There was a 1° increase in the gonial angle. Decrease in the upper incisor proclination as seen by reduction in upper 1 to NA angle by 10° (from 33 to 23°) and to SN plane by 11° (from 116 to 105°). There was a slight increase in the lower incisor inclination (lower incisor to NB increased from 30°/5.5 mm to 33°/7 mm and IMPA increased by 1°). Both overjet and overbite values have reduced to 2.5 mm and 3 mm, respectively. Improvement in the soft tissue profile.
Overall, the class II skeletal relationship has improved. The mandible showed favorable horizontal growth changes and was rotated marginally in downward and backward direction, with proportional increase in the vertical face heights. The upper incisors were tipped palatally, and lower incisors were marginally proclined by the Twin-block appliance. The soft tissue relationship has improved.
Section III: Posttreatment Assessment
The posttreatment extraoral and intraoral photographs are shown in Figures 10 and 11.
Occlusal Features
Incisor relationship: Class I
Overjet (mm): 2 mm
Overbite: 2 mm or 30%
Centerlines: Coincident midlines
Left and right buccal Class I molar relation and class I canine relation
Functional occlusal features: Mutually protected occlusion. Canine guidance on left and right lateral excursions with no working or nonworking side interferences. Anterior guidance on protrusion with posterior disclusion. No premature occlusal contacts during mandibular movements.
Complications Encountered During Treatment
During the fixed appliance therapy, the oral hygiene was not satisfactory despite repeated oral hygiene instructions and prophylaxis which resulted in increase in the white spot lesions which was present pretreatment.
Patient was not willing to go for near-end OPG due to the concern for radiation exposure due to which it was avoided. Hence, root parallelism could not be assessed at that stage. However, posttreatment radiographs revealed relatively parallel roots.
Occlusal Indices
The IOTN (DHC) and IOTN (AC) were 4a and 9 to begin with and 1 at the end for both components.
The PAR index score changed from the pretreatment 30 to posttreatment 2 with a change of 93.3%.
Radiographs Taken Toward/at the End of Treatment
Relevant Radiographic Findings
Unerupted third molar tooth buds were present in all quadrants except the third.
Normal condylar morphology.
Roots were relatively parallel.
No change in root length of upper incisors.
Posttreatment Cephalometric Findings and Their Interpretation
The posttreatment cephalometric values are provided in Tables 1 and 2.
Overall, the class II skeletal relationship has improved significantly by a combination of favorable skeletal and dentoalveolar corrections. The corrections achieved are within the stability of the soft tissue paradigm.
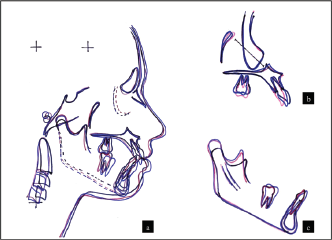
Cephalometric Superimposition
Superimpositions of pre-, mid-, and posttreatment cephalometric tracings are shown in Figure 14.
Section IV: Critical Appraisal
JJ was successfully treated with a combination of myofunctional therapy and comprehensive fixed orthodontics over 23 months. The original treatment aims were accomplished and the patient’s presenting complaint addressed. A good occlusal and aesthetic result was achieved and this was reflected in the PAR and IOTN scores.
The skeletal base relationship improved with significant improvement in facial profile. Although a slight relapse was observed after the functional phase, favorable intercuspation could be achieved at the end of the treatment.
Class I molar and canine relation was achieved. A mild rotational relapse was observed in 16, 10 months after debonding. A close monitoring is required for this and if needed, a vacuum-formed clear retainer to correct this may be planned.
The maxillary incisor inclination was slightly less than ideal at the end of fixed orthodontics. The lower incisors though slightly proclined to begin with and was further proclined by functional appliance therapy, was corrected to near ideal toward the end of comprehensive fixed orthodontics. Ideal overjet and overbite were achieved with a class I incisor relation.
In spite of meticulous oral hygiene instructions and repeated ultrasonic scaling, enamel opacities were observed on multiple teeth. Prophylactic use of fluoride mouth rinse has been prescribed and a close monitoring is scheduled.
The status of third molars is to be evaluated during follow-up and if impacted or unfavorable, she will be advised to undergo extractions of the same.
Discussion
The IBO category II requires a case of class II malocclusion with an ANB of more than 5° treated using growth modification and fixed appliance. 4 The above case had an ANB of 6.5° and Wits appraisal of +4 mm justifying the inclusion under category II. Patient was in CVMI stage 3 with mandibular retrognathism and positive VTO, hence growth modification using functional appliance was planned. Twin-block was selected due to patient comfort, affordability, and availability of remaining growth and time.5, 6 Traditionally, 2-phase treatment was suggested for class II malocclusion, where the first phase was done in the mixed dentition stage using functional appliances followed by a period of retention for 1 to 1.5 years and in the second phase in early adolescence another course of comprehensive fixed appliance treatment with or without functional appliance is undertaken. 7 However, the evidence is now clear that a 2-phase treatment is no more superior to 1-phase treatment and the former is recommended only in cases of anticipated traumatic dental injury or psychosocial issues.8-11
The most critical issue in integrated single-phase treatment when removable functional appliance is used includes maintenance of the bite correction during the transition stage from removable to fixed appliance. 12 Many appliances including EVAA, Steep and Deep, and AIBP were recommended until class II mechanics with rigid wire is initiated. An AIBP retained using ball end clasp was used in this case. The reciprocal lower incisor proclination was controlled using incorporation of labial root torque in the lower labial segment and use of short class II elastics.
Molar derotations can be addressed in many ways including the use of TPA with derotation moments, over-corrected molar tube positions, fourth order bends incorporated in archwires, couple forces generated from adjacent teeth, or from mini-implants. 0.018 SS Australian archwire with asymmetric toe-in bends was used to derotate UR6 and maintained thereafter.
Retention following growth modification and comprehensive treatment may be a problem at times considering the unfavorable pattern of growth that can still persist. Hence, a prolonged retention of the sagittal correction and deep bite is essential along with the dental corrections. Continued use of an ABP or AIBP is thus essential and followed in this case too during this phase.
Footnotes
Declaration of Conflicting Interests
Declaration of Patient Consent
The author certifies that he has obtained all appropriate patient consent forms. The patient has given her consent for her images and other related clinical information to be reported in the journal. The patient understands that her name and initials will not be published and due efforts will be made to conceal her identity, but anonymity cannot be guaranteed.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.