
Abstract
KL, a 12-year-old boy, presented with a class II Div I malocclusion on a class II skeletal base (retrognathic mandible) with a 7-mm overjet and a horizontal growth pattern. He had a convex profile, incompetent lips, lip trap, deep mentolabial sulcus, everted lower lip, and positive visual treatment objective (VTO). KL had a CS2 cervical maturation stage, which indicates 65% to 85% adolescent growth remaining. Treatment involved growth modification using a removable Twin Block with midpalatal expansion screw. This was followed by upper and lower fixed appliance using 0.022” × 0.028” slot Mclaughlin Bennet and Trevisi (MBT) prescription. The retention protocol involved upper wrap around and lower lingual bonded retainer.
Diagnosis and Etiology
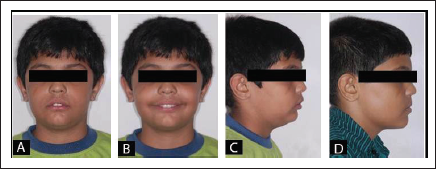
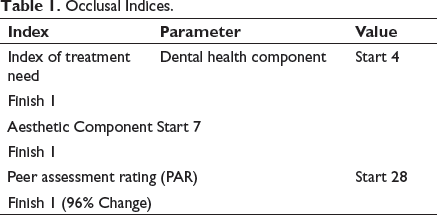
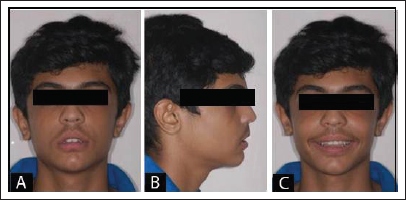
KL, a 12-year-old boy, presented with a chief complaint of forwardly placed upper front teeth resting on lower lip, presented with a class II Div 1 malocclusion on a class 2 skeletal base. He had a convex profile, posterior divergence, retrognathic mandible, incompetent lips, lip trap, deep mentolabial sulcus, everted lower lip, and average lower anterior facial height proportion and low mandibular plane angle. Intraoral examination showed no soft tissue abnormality, the oral hygiene was sub optimal, 26 and 46 were restored with glass ionomer cement. Both the arches were U shaped and there was mild labial crowding and buccal segment irregularities in the lower arch. Marginal ridge discrepancies were found between 26 and 27, 35 and 36, and 45 and 46. The incisor and molar relation were class II on both sides and the midlines was coinciding. The overjet was 7 mm and overbite was 6 mm (Figures 1 and 2; Table 1).
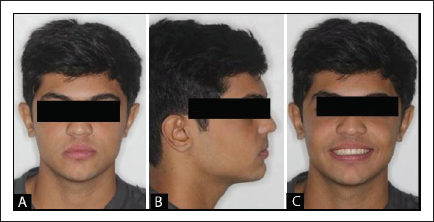
Pretreatment Extraoral Photographs: (A) Frontal With Lips at Rest. (B) Frontal Smile. (C) Profile. (D) Visual Treatment Objective.
Pretreatment Intraoral Photographs.

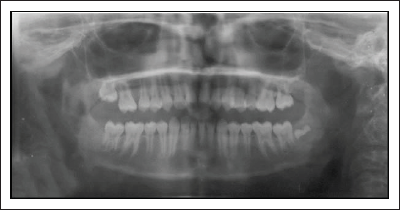
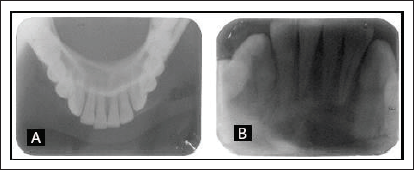
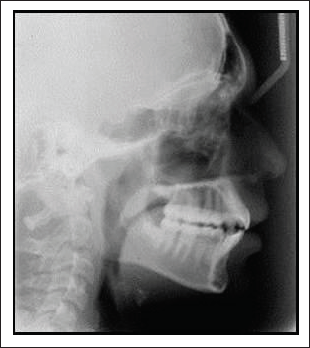
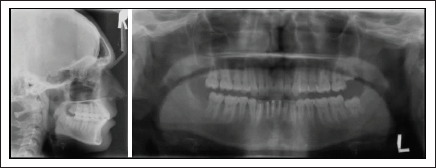
The pretreatment radiographs taken were lateral cephalogram, orthopantomogram (OPG), intraoral periapical (IOPA), and lower occlusal (Figures 3-5). The OPG revealed a radiolucency in the periapical region of 31 to 43. All permanent teeth were present including developing third molars on the left side; 18 and 48 were congenitally missing and 17, 47, 28, and 38 were unerupted and there were no signs of root resorption in other permanent teeth. All permanent teeth had good alveolar bone height and no signs of caries. The lower occlusal radiograph and IOPA revealed radiolucency in the periapical region of 31 to 43 region.
Pretreatment Lateral Cephalogram.

Pretreatment Orthopantomogram.
(A) Lower Occlusal Radiograph, (B) Intraoral Periapical.
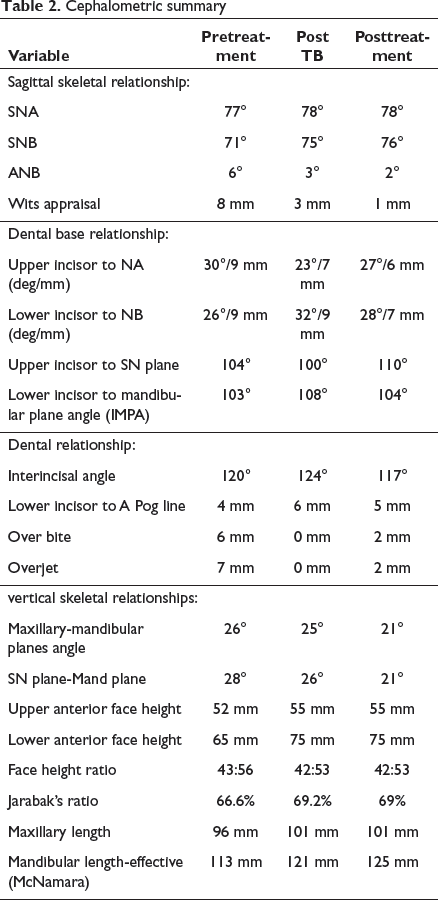
The lateral cephalogram revealed a class II skeletal malocclusion with an ANB angle of 6°. The maxillary-mandibular plane angle was average and concordant with the clinical findings. The lower facial height proportion was average. Both the upper and lower incisors were proclined compared to the normal values in relation to their dental bases. The nasolabial angle was average with a short upper lip and a protrusive lower lip relative to the Rickett's E-plane.
Diagnostic Summary
Angle’s class II malocclusion was due to mandibular deficiency with an ANB of 6°. He had a convex profile, incompetent lips, short upper lip, lower lip trap, retrusive mandible, horizontal growth pattern, and VTO positive. Skeletal maturity index showed CS2 stage indicating 65% of adolescent growth expected. The maxillary mandibular plane angle was average with an average lower anterior facial height. He had mild crowding in upper and lower arches with an overjet of 7-mm and 6-mm overbite.
Aims and Objectives of Treatment
The treatment objectives were (a) management of periapical lesion in 31 to 43 region, (b) attempt growth modification to correct class II anteroposterior relationship, (c) achieve class I molar and canine, (d) level and align and coordinate the dental arches, (e) achieve ideal overjet and overbite, and (f) finishing and detailing the occlusion.
Treatment Plan
The radiolucency in the periapical region of 31 to 43 was managed by a multidisciplinary approach. There was a history of trauma (fall during playing) 3 years back. The patient underwent root canal treatment in 31, 41, 42, and 43. The postendodontic radiograph showed radiolucency which persisted in spite of root canal treatment. Hence, curettage was done to remove the lesion with granulation tissue (Figure 6) and diagnosed as periapical granuloma. The radiolucency subsequently reduced.
The treatment was carried out in 2 phases. Phase 1 involved use of functional appliance (Twin Block) to reduce overjet and overbite and achieve class I molar relationship. Phase 2 involved use of fixed appliance treatment with 0.022” × 0.028” slot MBT prescription to align and level the arches. The prognosis for stability would be predicted to be good as upper wrap around retainer and the lower bonded retainers will aid maintenance of the corrected incisor position. A class I incisor relationship with a well-interdigitated occlusion would enhance stability. Patient was advised extraction of 18 and 48.
Treatment Progress
KL was advised full time wear of upper and lower Twin Block functional appliance (Figure 7). After correction of buccal segments to class I molar and edge to edge incisor relationship, the patient was advised night time wear of twin block. Postfunctional appliance records were taken (photographs, study models, and lateral cephalogram) (Figures 8-11). The upper and lower arches were bonded 7-7 with fixed appliance using 0.022” × 0.028” MBT prescription (Figure 10). The upper and lower arch were levelled and aligned using .016” NiTi, 0.016” × 0.022” NiTi, 0.018” × 0.025” NiTi, and 0.019” × 0.025” SS archwire. Interproximal slicing was done in the lower arch to address the proclination. During the end of treatment, brackets were repositioned in 11, 31, 34, 43, and 45 for finishing and detailing (Figure 12). Fixed appliance was debonded followed by upper wrap around and lower lingual bonded retainer.
IOPA After RCT and Shows Radiolucency Resolved After Removal of Granulation Tissue.

Intraoral Photographs With Twin Block.

End of Phase 1 Treatment Intraoral Photographs.

End of Phase 1 Post Twin Block Treatment Extraoral Photographs. (A) Frontal With Lips at Rest. (B) Profile. (C) Frontal Smile.
End of Phase 1 Treatment Lateral Cephalogram.
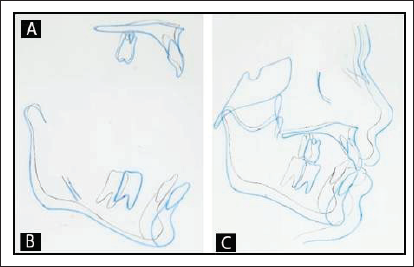
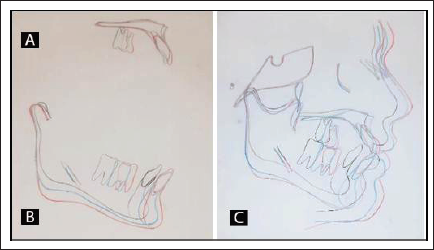
Pre and End of Functional Phase Superimpositions. (A) Maxillary Superimpositions: Registered on Anterior Surface of Palatal Vault. (B) Mandibular Superimpositions: Registered on Mandibular Canal. (C) Overall Superimpositions: Registered on Anterior Cranial Base.
Near End of Treatment Intraoral Photographs.

Treatment Results
Changes Observed at the End of Phase 1 Treatment
Cephalometric analysis of KL showed significant skeletal changes using functional appliance was downward and forward growth of the mandible with an increase in SNB and this resulted in an overall reduction in ANB by 3°. The Wits appraisal also supports an improvement in the skeletal anteroposterior relationship with a change in B point moving forward by 2 mm. Vertically, a small increase in the maxillary mandibular plane angle occurred. The superimposition of the maxilla and mandible showed vertical growth of the ramus and a downward and forward growth of the mandible. This may in part explain the increase in lower facial height. At the end of functional phase treatment, the lower incisors were proclined and the upper incisors retroclined. The lips were contained within the aesthetic norms of the Rickett’s E-plane. Some minor remodeling of soft tissues of the nose and chin was evident. These are expected maturational changes.
Changes Observed at the End of Phase 2 Treatment
At the end of phase 2, the ANB was 2° which indicates that a class I skeletal pattern was achieved. Vertically, a small decrease in the maxillary mandibular plane angle occurred and a small increase of the lower facial height due to vertical growth of ramus. The lower incisors to mandibular plane also increased as a result of proclination of the lower labial segment during treatment. At the end of phase 2 treatment, a class I incisor relationship with bilateral class I molar and class I canine with midlines coinciding was achieved (Figures 13-16). The overjet and overbite was 2 mm. The lips were contained within the aesthetic norms of the Rickett’s E-plane. Some remodeling of soft tissues of the nose and chin is evident.
Post Treatment Lateral Cephalogram and Orthopantomogram.
Post Treatment Cephalometric Tracing. Pre Treatment: Black; Post Functional Treatment: Blue; Post Treatment: Red. (A) Maxillary and (B) Mandibular Superimpositions. (C) Overall Superimposition, Registered on Sella-Nasion Line at Nasion.
Post Treatment Intraoral Photographs. (A) Frontal With Lips at Rest. (B) Profile. (C) Frontal Smile.
Post Treatment Intraoral Photographs.

Radiographs Taken Toward/at End of Treatment
Analysis of OPG revealed acceptable root paralleling at the end of treatment. Lateral cephalogram showed average inclination of upper and slight proclination of lower incisors. Third molars present on the left side were to be extracted later.
Summary of Treatment Changes
KL was successfully treated with an interdisciplinary approach for periapical lesion in 31, 41, 42, and 43 region.
A class I skeletal pattern was achieved at the end of treatment with an ANB of 2°. There was a reduction in ANB owing to an increase in SNB which improved the overall skeletal pattern. Growth of maxilla and mandible was in a downward and forward direction. Correction of the anteroposterior discrepancy improved the lip competence, lip support, and reduced the labiomental fold. Vertically, a decrease in the maxillary mandibular plane angle occurred due to vertical growth of ramus which was favorable .The class 2 incisor relationship was corrected with a combination of skeletal and dentoalveolar changes. An MBT prescription which usually favors postfunctional phase was used to increase palatal root torque for the upper and labial root torque in the lower arch. The lower incisors clinically appear proclined and an extraction approach would have prevented this but the soft tissue profile, the nasolabial angle, together with space requirement did not favor removal of all 4 first premolars. Interproximal slicing was done in the lower arch to address the proclination. The overbite and overjet was reduced to ideal. An aesthetic occlusion and good buccal segment interdigitation was achieved. Final PAR score of 1 was achieved, with a reduction of 96%. The near end of treatment lateral cephalogram and OPG identified no change in root length of the maxillary and mandibular incisors. No new enamel decalcifications were evident during and on removal of the fixed appliances. The results achieved were well maintained 4 years after treatment except for slight increase in gingival recession in the lower canines.
Critical Appraisal
11 and 21 required more mesial root tip and 46 needed more mesial offset and toe-in. Patient was informed about third molar extraction.
Footnotes
Statement of Informed Consent
Written informed consent was obtained from the patient for use of clinical photographs for publication.
Declaration of Conflicting Interests
Funding
The author received no financial support for the research, authorship, and/or publication of this article.