
Abstract
This case report submitted as a Category II case report in the Indian Board of Orthodontics Phase III exam describes the orthodontic treatment of an 11-year-old female patient with a skeletal Class II malocclusion due to mandibular retrognathia. She presented in the late mixed dentition and was treated with a two-phase treatment protocol. The first phase involved growth modulation with a Twin Block Appliance for mandibular advancement followed by the second phase of treatment with upper and lower fixed appliances and a non-extraction treatment plan. The fixed appliance used was 0.022’’ slot, metal pre-adjusted edgewise appliance with MBT prescription. The summary of the treatment, the case report, and the various records are reprinted here with minimal editing and reformatting so that the presentation resembles the actual documents submitted to the board.
Case Report
A.S, an 11-year-old female patient, reported to the clinic with a chief complaint of forwardly placed upper front teeth. On examination and analysis of relevant records, it was found that she presented with an end on molar relation bilaterally on an underlying Class II skeletal base on account of a retro positioned mandible. She had a normal mandibular plane angle in a growing patient. She had upper and lower second deciduous molars present in all four quadrants. It was also noted that the upper midline had shifted to the right and the upper canines partially erupted bilaterally. She had a convex profile with potentially incompetent lips and a positive clinical VTO. She was treated with a two-phase treatment protocol. The first phase involved growth modulation with a Twin Block Appliance which had the modification of having a jackscrew in the maxillary appliance and incisal capping in the mandibular appliance. The second phase of treatment involved non-extraction fixed appliance therapy with upper and lower fixed appliances. The fixed appliance used was 0.022’’ slot, metal pre-adjusted edgewise appliance with MBT prescription.
Section 1. Pre-treatment Assessment (Figures 1 and 2)
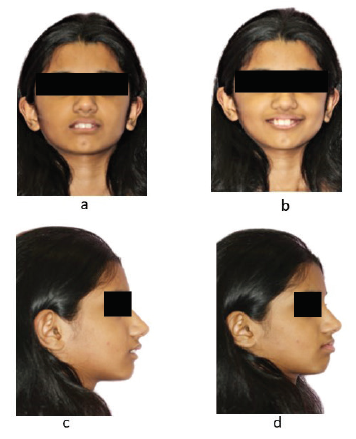
Pretreatment Extraoral Photographs: (a) Frontal View with Lips at Rest; (b) Frontal View with Smile; (c) Profile View (d) VTO.
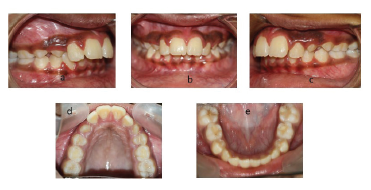
Pretreatment Intraoral Photographs (a) Right Buccal View; (b) Anterior View; (c) Left Buccal View; (d) Maxillary Occlusal View; (e) Mandibular Occlusal View.
Pre-treatment Assessment Details
Initials: A.S
Sex: Female
Date of birth: March 10, 2006
Age at start of treatment: 11 years
Patient complaint: “The patient complains of forwardly placed upper front teeth.”
Clinical Examination: Extraoral Features
Skeletal Assessment
Frontal examination: She was Mesiofacial with apparently symmetrical face, with relatively normal proportions horizontally and vertically. The upper midline was shifted to right side.
Profile examination: A.S had convex profile, potentially incompetent lips, an acute nasolabial angle, slightly long and pointed everted upwards nose, normal nasal bridge with normal mandibular plane angle.
TMJ: Normal on functional examination
Soft Tissue Assessment
Clinical Examination: Intraoral Features
Soft tissues: Mild Gingival Inflammation
Oral hygiene: Average with moderate amount plaque accumulation
Erupted teeth present: 11,12,13,14,5E,16,21,22,23,24,5E,26,31,32,33,34,7E,36,41,42,43,44,8E,46
General dental conditions: Deciduous second molars present in all four quadrants
Restorations on: Composite restorations with respect to 7E & 8E
Crowding/Spacing
Maxillary arch: She had deciduous second molars present bilaterally; it was also noted that the upper midline had shifted to right. The upper canines were partially erupted bilaterally.
Mandibular arch: She had deciduous second molars bilaterally with mild crowding
Occlusal Features
Molar relationship: Half cusp Class II (End on) bilaterally
Incisor relationship: Class II div 1
Overjet (mm): 9 mm
Overbite (mm): 7 mm
Centerlines: Maxillary midline shifted towards the Right side.
Left buccal segment relationship: End on relation.
Right buccal segment relationship: End on relation.
Crossbites: None
Displacements: Contacts between 11&12,21&22,42&43 were displaced
Rotations: Distobuccally rotated 42, Mesiobuccally rotated 24
Other occlusal features: Normal Curve of Spee in the Mandibular arch. Tapered upper and ovoid shaped lower arch form.
Pre-treatment Occlusal Indices
IOTN Dental Health Component:
Increased overjet greater than 6 mm but less than or equal to 9 mm: Great need for treatment
IOTN aesthetic component:
Severe Need for treatment
General Radiographic Examination
Relevant Orthopantomogram (OPG) Findings: Figure 3
Orthopantomograms: (a) Pretreatment; (b) Post Twin Block; and (c) Post-treatment.
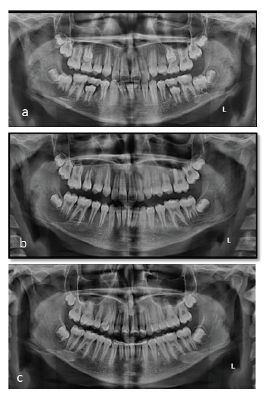
Pre-treatment: All permanent teeth are present except 15,25,35,45,17,27,37,47,18,12,28,38 and 48. Deciduous 5E,6E,7E,8E present. Root formation of canines is incomplete. No pathology seen. Lamina dura is intact and height of the interdental crest is normal.
Post twin block: In the post twin block panoramic radiograph, alveolar bone levels did not decrease compared to pre-treatment status, good root parallelism was achieved, interdental alveolar crest bone levels were horizontal and no significant root resorption was evident. The 17 and 27 was still erupting at this stage. All the third molars in all four quadrants had not erupted
Post-treatment: In the post-treatment panoramic radiograph, alveolar bone levels did not significantly decrease compared to pre-treatment status, good root parallelism was achieved, interdental alveolar crest bone levels were horizontal and no significant root resorption was evident. Lower third molars have not yet erupted.
Lateral Cephalogram
Pre-treatment Cephalometric Findings and Their Interpretation: Figure 4
Little Cephalograms (a) Pretreatment; (b) Post Twin Blog; and (c) Post-treatment.
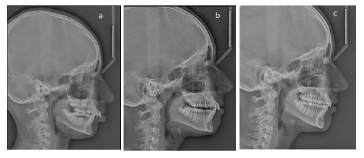
Various cephalometric findings are described in Table 1.
Cephalometric Findings at Various Stages of Orthodontic Treatment: Composite.
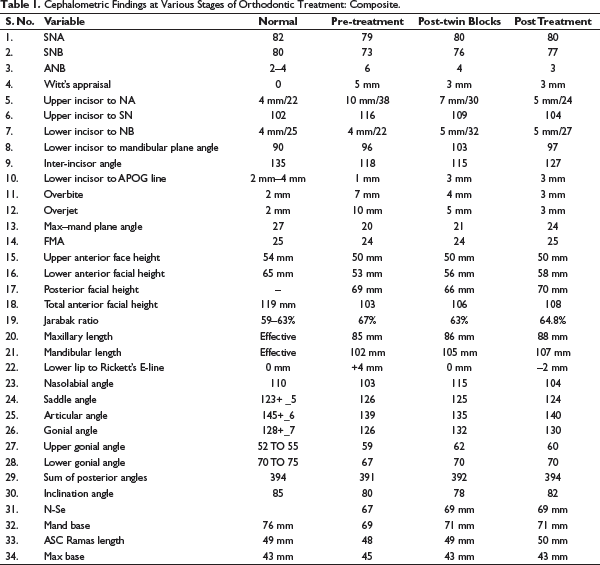
The sagittal relationship was towards Class II malocclusion on account of retro positioned mandible. The upper incisors were placed forwardly and the inclinations were also severely increased. The overjet and overbite were increased. The lower lip was procumbent leading to a convex profile with potentially incompetent lips.
Diagnostic Summary
A.S, an 11-year-old female, the patient presented with an end on molar relation bilaterally on an underlying Class II skeletal base on account of a retro positioned mandible as confirmed with SNB of 73°. She had a normal mandibular plane angle, saddle angle, articular, lower gonial angle in a growing patient, she was in her CS3 stage of the CVMI index. She had upper and lower deciduous second molars present in all four quadrants. It was also noted that the upper midline had shifted to the right and the upper canines were partially erupted bilaterally. She had a convex profile with potentially incompetent lips.
Problem List
Skeletal Class II relation with a normal maxilla and retro positioned mandible
Tapered-shaped upper and ovoid lower arches
Increased overjet
Increased overbite
Non-coinciding midline; maxillary shift to right side
End on molar relation bilaterally
Mild crowding in the lower arch
Proclined upper and lower anterior
Potentially Incompetent lips
Aims and Objectives of Treatment
To refer for appropriate management of mild gingivitis.
To correct the skeletal Class II jaw base relation by growth modulation by restricting growth of the maxilla while stimulating mandibular growth to allow the mandible to achieve and express its full growth potential.
To correct upper and lower incisor inclinations.
To establish a Class I buccal segment relationship bilaterally and a normal overjet
To level the curve of Spee in the lower arch by relative intrusion of the lower incisors, thereby establishing a normal overbite
To establish well-aligned upper and lower arches with normal arch form.
To achieve soft tissue balance and harmony through the above treatment.
Treatment Plan
On examination of relevant records, it was found that AS had Class II end on molar bilaterally on a Class II skeletal base on account of retro positioned mandible and normal maxilla as revealed by her reduced SNB of 73°. She had a normal mandibular plane angle, saddle angle, articular, lower gonial angle in a growing patient with CS3 stage in the CVMI index all parameters contusive for growth modulation with functional appliance. Since she had a retro positioned mandible it was planned to treat with two-phase treatment, first being the myofunctional phase for correction of skeletal dysplasia and second being the fixed mechanotherapy phase to achieve a stable and harmonious occlusion with proper interdigitation of the buccal segment. The myofunctional of choice in her case was the Twin Block Appliance since twin block from day 1 will bring the mandible forward which will aid in fully expressing the remaining growth left in the patient. Twin Block Appliances will also be easy to trim in order to facilitate the exfoliation of deciduous and guide the permanent teeth into occlusion. In the fixed mechanotherapy phase, the appliance planned was .022 slot metal braces with MBT prescription in order to correct the increased upper inclination prescription will provide adequate torque and tip which will help in achieving stable results.
Extractions
None
Appliance: Figure 5
Twin Blocks Photographs.
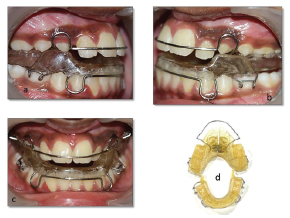
Phase 1: Twin Block Appliance
Phase 2: Maxillary and mandibular fixed appliances. The appliance used was 0.022’’slot, MBT prescription metal Pre-adjusted Edgewise Appliance.
Proposed Retention Strategy
Fixed lingual bonded retainers for the mandibular anterior and removable wrap around retainers extending till the second permanent molars in both the arches.
Prognosis for Stability
Good
Section 2. Treatment
Treatment Progress
Start of active treatment with Twin Block Appliance: December 8, 2017
Age at start of active treatment: [11 years]
End of active treatment with Twin Block Appliance: [March 9, 2019]
Active treatment time with Twin Block Appliance: 1 year 3 months
Start of Fixed Mechanotherapy: March 11, 2019
End of Fixed Mechanotherapy: July 1, 2021
Active treatment time with Braces: 2 years 4 Months
Total treatment time with twin blocks and Fixed appliance 3 years 7 Months
End of retention: Retention is ongoing in both the upper and lower arches.
Key Stages in Treatment Progress
December 8, 2017: Bite registration for the fabrication of Twin Block Appliance
December 15, 2017: Twin Block Appliance with modification of having a jackscrew and incisal capping was given for full-time wear
March 9, 2019: Twin Block Appliance discontinued
March 11, 2019: Maxillary and Mandibular appliance was bonded with UL 0.014 NiTi arch wires ligated in both the arches for alignment
December 15, 2019: U/L 019x025 Niti continuous archwire were ligated once the maxillary lateral incisor had got aligned
March 11, 2020: Upper 019x025 SS with mild curve of Spee and lower 019x025SS with mild reverse Curve of Spee with active tie backs were ligated for residual space closure.
September 13, 2020: Parallel elastics given for correction of midline
July 1, 2021: Maxillary and Mandibular Appliance was debonded and lower bonded lingual retainer bonded
July 3, 2021: Maxillary and Mandibular Wraparound Retainers were given
Post-twin Block Cephalometric Findings and Their Interpretation
Post Twin Block there was a good amount of improvement seen in the position of mandible (SNB 77) and also there was improvement in the inclination of upper anterior teeth. The lower incisor had proclined a little but was well within the normal range. The soft tissue profile became straight with a remarkable change seen in the nasolabial angle and E-line.
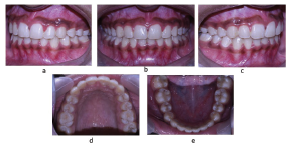
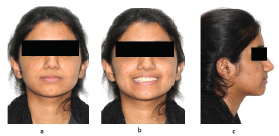
Section 3. Post-treatment Assessment (Figures 6 and 7)
Post Intraoral Photographs: (a) Right Buccal View; (b) Anterior View; (c) Left Buccal View; (d) Maxillary Occlusal View; and (e) Mandibular Occlusal View.
Post Treatment Extraoral Photographs: (a) Fronting View with Lips and Rest; (b) Frontal View with Smile; (c) Profile View; (d) VTO.
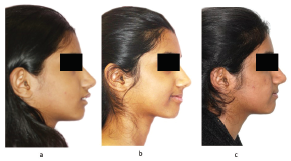
Comparison Profile Extraoral Photographs.
Occlusal Features
Molar Relationship: Class I
Incisor relationship: Class I
Overjet: 2 mm
Overbite: 2 mm
Centerlines: Coinciding with each other
Left buccal segment relationship: Class I canines, premolars, and Molars
Right buccal segment relationship: Class I canines, premolars, and Molars
Crossbites: None
Displacements: Contact between 26&27,46&47 is slightly displaced
Functional occlusal features: Mutually protected occlusion and canine guided in excursive movements.
Other occlusal features: Curve of Spee and Curve of Wilson in the lower arch within optimal limits.
Post Treatment Cephalometric Interpretation
The sagittal position of mandible and effective Mandibular length increased over the treatment period. Upper incisors inclination improved remarkably and lower incisors moved slightly forward leading to optimal overjet and overbite. Anterior crossbite was corrected. Nasolabial angle was average. The position of lower lip significantly improved during the treatment which helped in an improvement in facial profile, good maxillary incisor exposure, enhanced smile arch, smile esthetics, and improved facial balance Comparison of pre-treatment, post expansion, and posttreatment results showed a clinical improvement in soft tissue profile, normal overbite and overjet.
Results Achieved Include
The case was selected as per Category II of the IBO case requirements which is skeletal and dental Class II malocclusion with ANB angle greater than 5 degrees, case should exhibit efforts taken to correct the sagittal discrepancy non-surgically (with orthopedic and orthodontic treatment). The Twin Block Appliance facilitated the forward posturing of the mandible allowing it to express its full growth potential, thereby significantly improving the skeletal Class II jaw relationship and Class II molar relationships with significant orthopedic changes. The molar and incisor relationships were corrected partly by skeletal changes and partly by dentoalveolar changes. The functional aspects of the occlusion achieved were acceptable. The fixed appliance therapy helped in achieving good incisor inclinations and a well-balanced occlusion. We were able to achieve all the treatment objectives we had planned at the time of the start of treatment. The facial soft tissue features showed a substantial improvement, with appreciable improvement in profile convexity and lip competency.
Retention
The lower anterior was bonded with lingual retainer and removable wrap-around retainers for the upper and lower arches. She was advised full-time removable retainer wear for the first 10 to 12 months followed by part-time wear at night for the next 12 months and then it could be gradually weaned off.
Section 4: Critical Appraisal
The patient and her parents were very happy with the treatment results. Although initially there were compliance issues with the patient not wearing the Twin Block Appliance but later these were completely resolved. The patient turned out to become fully dental health conscious was compliant with her appliance wear and reporting for routine follow up appointments. The settling could have been better on the right buccal segment but it will improve with time. The buccolingual of the lower left second molar could have been better. The patient was referred to a periodontist for the necessary management of the gingivitis following the removal of the fixed appliance.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Patient Consent
The author certifies that he has obtained all appropriate patient consent forms. In the form, the patient has given her consent for her images and other clinical information to be reported in the journal. The patient understands that her name and initials will not be published, and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.