
Abstract
Here is a case report of a 20-year-old female patient with skeletal Class I malocclusion, with Angle’s Class I molar relation on the right and super Class I molar relation on the left side. The patient was diagnosed with hyperdivergent face pattern, proclined upper and lower anteriors, convex profile, potentially competent lips, short upper lip, average nasolabial angle, and anterior facial divergence. Treatment was organized by Damon System and En-masse distalization using the Infrazygomatic Crest and buccal shelf bone screws. The facial changes produced as a result of treatment were directly related to skeletal and dentoalveolar modifications that were designed as goals for patient treatment. It provided a minimal friction environment for the full-arch distalization. In this borderline bimaxillary protrusion case with a good profile, en-masse distalization turned out to be a better option than extracting the premolars and retracting incisors. It also stands out to be an example for the management of the same.
Introduction
For a long time, the extraction of teeth in orthodontic intervention has always been debated. Whether to extract or retract the premolars remain unclear in borderline cases. Initially, a decision regarding premolar extraction was taken by considering the hard tissue profile only, but due to the recent soft tissue paradigm shift, soft tissue profile is also taken into consideration. In a straight pleasant profile, the orthodontic treatment with premolar extraction can lead to flattening of the profile, which can make the patient look 5 to 10 years older than the current age.1, 2
The extra radicular placement of mini-implants or mini-plates became possible with the advent of the skeletal anchorage system, which appears to be the ideal place where the en-masse retraction of whole dentition is required. Miniscrews have overcome many of these problems regardless of whether one or all of the posterior molars will be moved. Sagittal movements of dentition in cases of extraction are often difficult and time-consuming. Therefore, when performed with skeletal anchorage, it reduces the side effects. Although no special coherence is required, incisor positions and facial profiles can be well controlled. 2
Mini-implants, or miniscrews, are included as a complete suspension system for good use in orthodontic practice. Although it is common to place them in areas of the alveolar process located between the roots of the affected teeth, new sites have been proposed, called extra alveolars. 3 Numerous authors recommend the infrazygomatic crest and the mandibular buccal shelf area as suitable places for a great number of orthodontic therapies that require an effective and safe adherence system, thereby increasing treatment limits. The bone quality of the infrazygomatic crest and buccal shelf area are ideal for good stability of screw installation. 3 This can withstand the force required for distalization without interfering with the roots of teeth. A passive self-ligation system provides the least friction as compared to other bracket systems. This advantageous characteristic when combined with the infrazygomatic and buccal shelf bone screws becomes much beneficial while undergoing en-masse distalization.1, 4
Conversion of extraction to non-extraction treatment, using miniscrews for complete distalization of both maxillary and mandibular dentition, is discussed in the present case report. Our case report presents a bimaxillary protrusion case with a delicate profile of soft tissue treated with en-masse distalization of both dental arches using the Damon system using infrazygomatic bone screws (IZC) and buccal shelf screws (BSS) without the removal of premolars.
Case Report
A 20-year-old female reported with the chief complaint of irregularly arranged, forwardly placed teeth that she wanted to get fixed. Detailed clinical history revealed that the patient had a cesarean delivery and was born with a hearing defect in the right ear. The extraoral examination of the patient showed mesoprosopic facial form, mesocephalic head, potentially competent lips, and complex smile with 70% of incisal exposure. The patient was diagnosed with a convex profile, anterior divergence, convexity/bulging on the dorsum of the nose, the flattened tip of the nose, average nasolabial angle, short upper lip, average malar prominence, and mandibular prominence (Figure 1).
Pre-treatment Extraoral Photographs.

Intraoral examination revealed proclined upper and lower anteriors, Angle’s Class I molar relationship on the right side and super Class I molar relationship on the left side, having 3.5 mm overjet, 1 mm overbite, rotated upper left central incisor, and second premolar with square-shaped upper and ovoid-shaped lower arches (Figure 2).
Pre-treatment Intraoral Photographs.

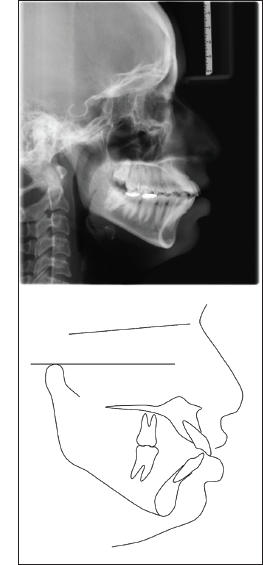
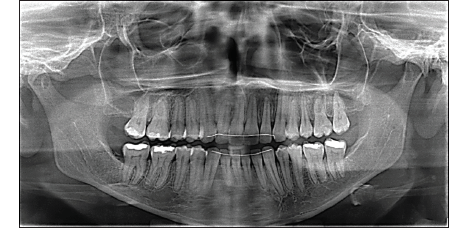
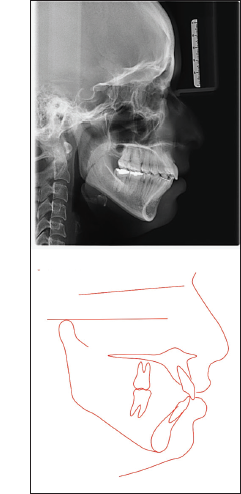
The patient was subjected to radiographic examination. Panoramic radiograph revealed that temporomandibular joint (TMJ) of the patient was normal with bilaterally symmetrical condyles, and third molars were erupting in all the quadrants with mesioangular impaction with respect to mandibular right third molar (Figure 3). Lateral cephalometric analysis showed skeletal Class I pattern (A point, Nasion, B point (ANB angle) = 3 degrees) with a plane angle of mandibular angle (SN − MP = 37 degrees). The maxillary and mandibular incisors are proclined (U1 − SN = 119 degrees; incisor mandibular plane angle—IMPA = 107.5 degrees), and the interincisal angle (98 degrees) is elevated, showing bimaxillary protrusion, high mandibular plane angle, and short upper lip (Figure 4). In Bolton’s analysis, there was anterior maxillary excess of 1 mm and total maxillary excess of 1.14 mm. Carey’s analysis showed the need for a space of 4.5 mm in the upper arch and 5 mm in the lower arch.
Pre-treatment Panoramic Radiograph.

Pre-treatment Lateral Cephalogram.
Treatment Objectives
Patient treatment objectives: (a) improve the appearance of the aesthetic profile; (b) reduce lip protrusion and soft tissue aesthetics; (c) reduce the proclination of the upper and lower anteriors; (d) achieve ideal overjet and overbite; (e) correction of midline shift; (f) derotation of rotated 21 and 25; and (g) to correct the smile aesthetics.
Considering the soft tissue profile of the patient, the treatment plan decided was (a) extraction of all third molars (b) retract the entire maxillary and mandibular dentition by en-masse distalization using bone screw skeletal anchorage. The Damon passive self-ligating bracket system was selected (Ormco, Orange, Calif.), which incorporated arch flow mechanics that defined both flow mechanics of the self-ligating bracket along the archwire and the distal drift of the initial archwire itself. The third molar extraction was carried out before beginning the treatment.
Treatment Progress
Initial leveling and alignment were achieved with 0.013″ CuNiTi, 0.014 × 0.025″ CuNiTi, and 0.018 × 0.025″ CuNiTi archwires. There was increased patient comfort with CuNiTi wires.1, 5Low torque brackets in the upper anteriors were preferred for the correction of proclination, whereas standard torque was used in the lower anteriors for maintaining the roots of lower incisors in the cancellous bone (Figure 5).
Initial Bonding.

0.013″ CuNiTi Initial Light Round Wire Phase.

0.014 × 0.025″ CuNiTi High-Technology Edgewise Phase.

0.018 × 0.025″ CuNiTi High-Technology Edgewise Phase.

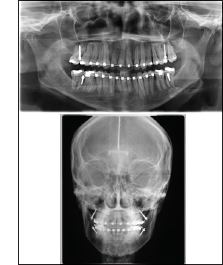
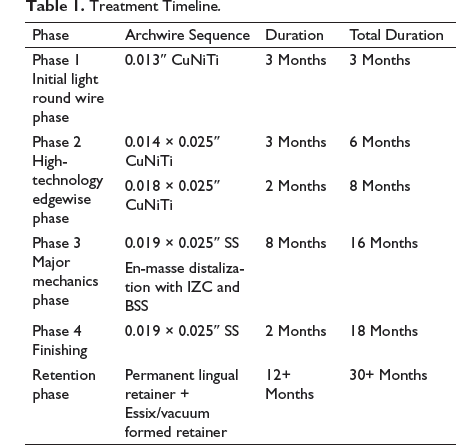
After the leveling and alignment stage, extra-radicular infrazygomatic and buccal shelf bone screws were used for the full-arch distalization of both the arches without any interference of the roots of teeth. The 0.019 × 0.025″ SS archwires were used for the distalization of both dentitions, using stainless steel infrazygomatic bone screws (BioRay A1-P, 2 × 14) with a long collar in the infrazygomatic crest region between the first and second maxillary molars extra radicularly. BioRay A1-P, 2 × 10 stainless steel screws were then placed in the buccal shelf region between the first and second maxillary molars. Extra-radicular infrazygomatic and buccal shelf bone screws caused the full-arch distalization of both the arches without any interference with the roots of teeth. An orthopantomogram and a posteroanterior cephalogram were taken to check the position of bone screws (Figure 7). Retraction mechanics were performed by applying force by connecting the power chains from the screw on one side (including lateral and central incisors) to the screw on the other side. The force of 250 gm was applied in all the quadrants (Figures 6 and 7). The en-masse distalization of all maxillary and mandibular dentition was completed in 8 months, with a total treatment period of 18 months (Table 1). The long axis of the upper incisors was parallel to the facial axis (Figure 8).
Orthopantomogram and PA Cephalogram After the Insertion of the Screws.
En-Masse Distalization with IZC and BSS Bone Screws.

Lateral Cephalogram After Completion of Distalization.

Treatment Timeline.
Treatment Progress
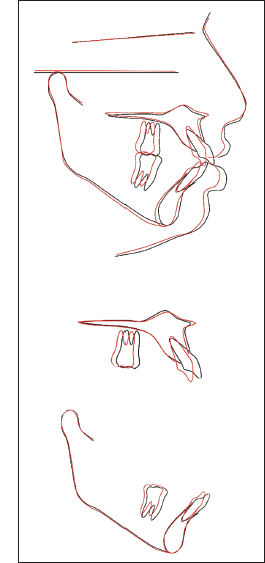
Post-treatment records show that treatment goals have been achieved. Post-treatment pictures have shown amazing improvements in lip profile and facial aesthetics, which has led to the retraction of the anterior teeth. The relationship of Class I molar and canine was established, with ideal overjet and overbite (Figures 9 and 10). Cephalometric superimposition has shown that maxillary molars were distalized by about 5 mm at the crown level and 4 mm at the apex level; maxillary incisors retracted by 6 mm, and mandibular incisors by 5 mm. The upper lip retracted by 2 mm and the lower lip by 3 mm, both coming in the standard range relative to E-line. The superimposition of pre- and post-cephalometric tracings showed that there was a clockwise rotation of the maxillary dentoalveolar complex, as the applied force was below the center of resistance to the maxillary dentition. The interlabial gap and incisal display at rest were closed, and it had reached appropriate nasolabial, labiomental sulcus, and joint angles (Table 2; Figures 11 to 13). Following a 12-month and 20-month follow-up, it was revealed that the occlusion was stable with satisfactory facial aesthetics (Figures 14 to 16).
Post-treatment Extraoral Photographs.

Post-treatment Intraoral Photographs.

Post-treatment Panoramic Radiograph.
Post-treatment Lateral Cephalogram.
Cephalometric Superimposition.
1-Year Post-treatment Follow-Up.

20 Months Post-treatment Follow-Up Extraoral Photographs.

20 months post treatment followup Intra-Oral Photographs.

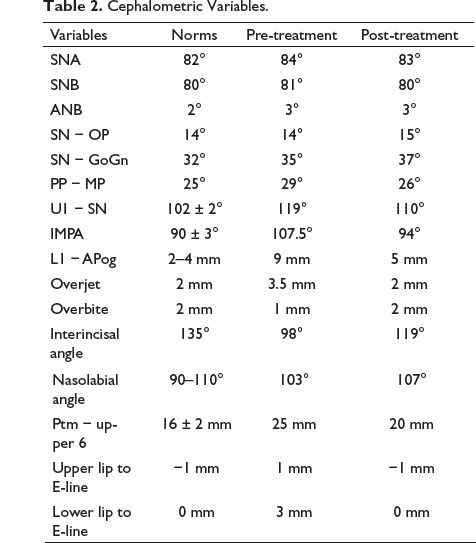
Cephalometric Variables.
Discussion
The changes in the face produced as a result of treatment were directly related to skeletal and dentoalveolar alterations that were planned as treatment goals for the patient. Facial aesthetics were the main reason for seeking orthodontic treatment.
Bimaxillary protrusion characterized by severely proclined maxillary and mandibular incisors could be corrected with orthodontic treatment. The soft tissue implied strained and protruded upper lips, creating a severe convex profile. The treatment often involved extraction of all first premolars to provide space for the retraction of anterior teeth. Cases with mild-to-moderate bimaxillary protrusion with a pleasant profile where soft tissue implies moderately convex toward straight profile generally raised the question for the extraction line of orthodontic treatment with first premolars, as the space required to retract the anteriors was less than the extraction space. Also, these patients usually wanted to avoid the removal of healthy teeth other than the third molars. In mild-or-moderate bimaxillary protrusion, the required space for incisal retraction was usually small as compared to the premolar size, and this could lead to improper use of extraction space. 6 Four premolar extraction treatments may be recommended when significantly improved incisor tension and soft tissue profile were required for patients. The space available from the extraction space of the third molar distal to the second molar could be used to distalize the entire dental arch by taking the help of skeletal anchorage. Before the introduction of mini-implants for skeletal anchorage, such distalization was achieved using traditional appliances such as headgear, modified Nance arches, and pendulum appliances.4–7The traditional appliances lacked control and also faced problems in patient compliances.
The mini-implant anchorage provides better anchorage control and minimal anchorage loss as compared to conventional distalizers. 8 For the distalization of the dental arches, the position of the mini-implant placement plays an important role. 1 The sites like the infrazygomatic crest region, buccal shelf area, and retromolar region are with thicker cortical bone layer. The placement of screws at a distance away from the tooth root is preferred to avoid interference with dental movements.9–11
In the present case, the passive self-ligating Damon system along with the infrazygomatic and buccal shelf bone screws provided a minimal friction environment for the full-arch distalization. 12 So, the force generated gets directly transmitted to the teeth and the supporting structures without any interference. 7 The Damon system mechanics demonstrate the lip bumper effect, similar to using lip bumper appliance due to the pressure from the orbicularis muscle that can move the teeth distally. 1 The low torque brackets in the upper anteriors were proved to be beneficial for the proclination correction, while the standard torque brackets in the lower anteriors provided the roots to be positioned in the cancellous bone for better stability. The center of resistance (Cres) of the maxillary dentition was shown to be close to the center of the premolar roots. 13 The position of the miniscrews in relation to the Cres determined the magnitude and direction of the force vector and helped to achieve arbitrary arch rotation. 14 The direction of force was kept below the center of resistance to the maxillary complex, which resulted in a clockwise rotation of the maxillary dentoalveolar complex. 15 If the retraction of maxillary incisors would have been planned, following the premolars extraction, it could have resulted in undesirable profile flattening.
Thus, an ideal overjet and overbite were achieved in the present case, with ideal incisal inclination in both the arches. The patient was very happy with her teeth and face and was more confidently smiling at her follow-up visit.
Conclusion
This case report demonstrates the en-masse distalization of both maxillary and mandibular arches by application of extra-alveolar bone screws along with passive self-ligation bracket system, instead of treatment with extraction and traction, for the correction of bimaxillary protrusion. A pleasant attractive smile, passive lip seal, and a balanced facial profile were achieved. The treatment results were stable at 20 months after the treatment completion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Written informed consent was obtained from the subject for the use of photographs for publication.